MIDCENTRAL DISTRICT HEALTH BOARD - MIDCENTRAL DHB
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MidCentral
District Health
Board
Agenda
Clinical Council
Distribution
Council Members
• Dr Simon Allan (Chair)
• Gail Munro (Ex-officio)
• Dr Don Baken
• Fiona Bradley Date: 7 April 2021
• Jane Ayling
• Tim Dunn
• Celetia Williams Time: 5.15-7.15pm
• Sophie Loveridge
• Dr Garry Forgeson
• Dr Nader Fattah Place: Seminar Room,
• Dr Nicola Pereira Arohanui Hospice
• Raeleen Toia
Management Team
Judith Catherwood, General Manager, Quality
and Innovation
Dr Kelvin Billinghurst, Chief Medical Officer
Gabrielle Scott, Executive Director, Allied Health
Celina Eves, Executive Director Nursing
Jodie Hickey, Committee Administrator
Council Secretary Contact Details:
Jodie.hickey@midcentraldhb.govt.nz
Next Meeting Date: May 2021
Deadline for Agenda Items: 19 April 2021
1
Midcentral District Health Board
Clinical Council Meeting
Wednesday 7 April 2021
1. KARAKIA 5.15PM
He Karakia Timata
Kia hora te marino
Kia whakapapa pounamu te moana
Hei huarahi mā tātou I te rangi nei
Aroha atu, aroha mai
Tātou I a tātou I ngā wā katoa
Hui e tāiki e
May peace be widespread
May the sea be smooth like greenstone
A pathway for us all this day
Give love, receive love
Let us show respect for each other
2. APOLOGIES
3. NOTIFICATION OF LATE ITEMS 5.20PM
4. CONFLICT AND/OR REGISTER OF INTERESTS 5.25PM
4.1 ADMENDMENT TO REGISTER OF INTEREST
Pages 4
5. COVID 19 VACINATION CAMPAIGN 5.35PM
Discussion: Clinical Council members to continue discussing
Covid 19 vaccination plan and how the Clinical
Council can support the plan.
Discussion to be led by Dan Hirst, Covid 19 Response Manager
6. FUTURE OF PHARMACY 6.05PM
Pages: 6-22
Documentation: Pharmacy Engagement project
Discussion: Clinical Council members to discuss the workforce
engagement project and determine how the
Clinical council can support prioritized activities
Discussion to be led by Fiona Bradley, Clinical Council member and Dr Nader
2Fattah, Clinical Council member
7. AGENDA ITEMS 6.45PM
Pages: 23-27
Documentation: Clinical Council Focus Areas 20-21
Recommendation: Is recommended that the Clinical Council review
the Clinical Council focus areas and confirm the
Agenda items for the next meeting
8. MATTERS ARISING 6.55PM
Pages: 23
Documentation: Clinical council matter arising
Recommendation: Clinical Council to update the matters arising
schedule
9. LATE ITEMS 7.00PM
10. MINUTES OF THE PREVIOUS MEETING 7.05PM
Pages: 29-32
Documentation: Clinical Council 3 March 2021 Minutes
Recommendation: is recommended that the Clinical Council confirm
the 3 March 2021 Clinical Council minutes to be
true and correct record
11. MEETING CLOSED 7.15PM
Nāku te rourou nāu
Te rourou ka
Ora ai te iwi
(With your basket and mine the people will be fed)
Go in peace
3Register of Interests: Summary, March 2021
Name Date Company/Organisation Nature of Interest
Allan, Simon 22.8.17 Central PHO Board Member.
22.8.17 MidCentral DHB Employee – Palliative Care Specialist.
22.8.17 Cancer Society Manawatu Member of Executive.
22.8.17 Arohanui Hospice Director, Palliative Care.
Ayling, Jane 11.12.19 THINK Hauora Member THINK Hauora Board
25.8.17 Royal NZ College of General Practitioners Assessor.
1.7.18 J Ayling – contractor Locum primary health care nurse contractor.
Transformational leadership coach
4.11.20 Cook Street Healthcare Employee
Baken, Don 11.9.17 Massey University Employee - Clinical Psychologist/Research
Co- ordination/Regional Lead Psychology &
Social Support Initiative.
Bradley, Fiona 6.9.17 Green Cross Health Ltd Shareholder
16.2.21 THINK Hauora board Member
16.2.21 Contractor Locum Pharmacist (MidCentral Pharmacies)
16.2.21 MidCentral Community Pharmacist Group Pharmacy Project Facilitator
Tim Dunn 24.6.20 Occupational Therapy NZ Member
24.6.20 Occupational Therapy Board of NZ Contractor
24.6.20 MidCentral Employee
Fattah, Nader 7.11.17 THINK Hauora Chair, Clinical and Digital Governance Committee
Trustee, THINK Hauora Board
Principal Medical advisor
7.11.17 Best Care (Whakapai Haoura) General Practitioner
7.11.17 Youth One Stop Shop General Practitioner
14.2.19 MidCentral DHB Member, Primary, Public & Community Advisory
Group
1.8.19 Ministry of Health HISO Member
Garry Forgeson 18.6.19 MidCentral DHB Employee – Oncologist
1.8.17 Cancer Society of New Zealand Inc Board Member
18.6.19 CSNZ Central Districts Division Board President
24.8.17 PNH Regional Cancer Treatment Trust Member
Loveridge, Sophie 20.6.19 Kauri Healthcare Employee - Registered Nurse
Pereira, Nicola 1.8.17 MidCentral DHB Employee – Paediatrician, and, Deputy Clinical
Director, Child Health.
1.8.17 Advanced Paediatric Life Support Instructor.
1.8.17 Royal College of Paediatrics & Child Health Member.
(UK)
1.8.17 Royal Australasian College of Physicians Member.
1.8.17 Paediatric Society of New Zealand Member.
1.8.17 Ministry of Health Technical Expert Assessor for MoH Audits.
Williams, Celetia 30.6.20 AUT University Employee - Lecturer at AUT University Department
of Paramedicine
30.6.2 St John Ambulance New Zealand Employee - Intensive and Extended Care
Paramedic
30.6.2 Vivere New Zealand Trust Founding member and Trustee
30.6.2 AUT University Doctoral candidate
30.6.2 Oranga Tamariki Caregiver
30.6.2 Australasian College of Paramedicine Member
4Clinical Council members
attendance record
August September October November February March
Dr Simon Allan
Dr Don Baken
Fiona Bradley
Jane Ayling
Tim Dunn
Celetia Williams
Sophie Loveridge
Dr Garry Forgeson
Dr Nader Fattah
Dr Nicola Pereira
Raeleen Toia
5For:
Endorsement
Approval
Noting
Discussion
To: Clinical Council
Author: Fiona Bradley
Date of meeting: 7 April 2021
Subject: Community Pharmacy Engagement project
RECOMMENDATION
That the Clinical Council:
• Note the update on the recent community pharmacy engagement mahi/ work
• Endorse the prioritised Roadmap that outlines the key areas of focus/projects for the next
12-months
• Discuss and consider other ways to support and influence this work within the DHB
1. PURPOSE
To provide the Clinical Council with an overview of the work undertaken locally with the community
pharmacy network through two workshops and the development of a roadmap (projects).
2. Background
Community pharmacy is being increasingly challenged by a range of factors impacting the sustainability of
its workforce and pharmacy as a business, in particular:
• Challenges around attracting and retaining pharmacists to the profession and to the region,
especially locums
• An increasingly competitive landscape
• A well-recognised need for improved communication and flow of information between primary and
secondary care
• A complex funding and regulatory environment.
These factors are not limited to MidCentral. However, MidCentral Community Pharmacy Group (MCPG) as
a membership group representing local community pharmacies and THINK Hauora as the Primary Health
Organisation (PHO) for the MidCentral community, are collectively looking for ways to support the
sustainability of the community pharmacy workforce within the district and strengthen connections within
primary and secondary care.
This requires engaging directly with those working within community pharmacies to share issues,
challenges and opportunities, generate ideas, and identify priorities. It also requires integration (where
appropriate) of regional and national primary health care strategies such as He Korowai Oranga (New
Zealand’s Maori Health Strategy), the Pharmacy Action Plan 2016-2020, Implementing Medicines New
Zealand 2015 to 2020 and, in particular, the Pharmacy in MidCentral Strategy with its guiding principles of
people-centric, better health outcomes and best practice.
Holding a workshop with the community pharmacy network would ensure solutions are relevant to the
unique challenges and opportunities of this workforce and the district and build upon national and regional
frameworks. The initiative follows on the back of a recent THINK Hauora and General Practice network
engagement to find solutions related to GP workforce sustainability.
6Two workshops have been completed with the community pharmacy network, led by Chard Consulting
around the “Future of Community Pharmacy”. The workshops were hosted at THINK Hauora and funded
through MCPG and THINK Hauora.
The first workshop was held prior to Christmas (December 2020) and at such a busy time of year, it was
amazing to have a strong turnout and to have a good discussion to contribute to this work.
The first workshop was an opportunity for the Network to:
- build on the foundation established by the Pharmacy in MidCentral Strategy (2019)
- “look up and out” at what we’ve achieved and what’s happening around us
- brainstorm practical actions we can take to sustain our workforce
- consider draft infographics and use these to prompt discussion of the current health and pharmacy
environment, nationally and in the MidCentral district.
- critique and add to the information, identify data gaps on the infographics
- provide their opinion on the issues and opportunities that face the network today.
The second workshop was at the start of February 2021 with a smaller number of attendees. The pharmacy
network was shown the final infographics, which had been updated to incorporate feedback from the
attendees at the first workshop and addressed identified data gaps where this information could be obtained.
The infographics are attached. The first 1-8 of these are an environmental scan of key data and
information around the current state and future trends facing community pharmacy and the
pharmaceutical workforce – globally, nationally, and regionally.
The infographics 9-12 (insights, covid experiences, influence and control) are the "raw outputs" and ideas
directly shared from those attending the workshops. These share what pharmacists are currently
experiencing, thinking and feeling. These were used and taken into consideration in putting together the
Roadmap. These will provide valuable background for the next phase of design and development work on
the Roadmap focus areas (projects).
The set of infographics will be used to broaden engagement with a wider stakeholder network. These
visuals are a great set of tools to highlight what’s important for community pharmacy in MidCentral,
provoke further conversation and direct action to the right places.
One of the key outputs from the workshops was to come up with an achievable set of actions that would
really make a difference to community pharmacy and can be realistically achieved, this developed into the
“roadmap”.
At the second workshop, the Network was asked to prioritise the opportunities and issues so that this could
be captured into a roadmap of areas of focus (projects) for the next 12-months and beyond.
Four key priority themes emerged from the first session that were explored further at the second
workshop:
1) Ways of Working - explore the potential of general practice and community pharmacy
collaboration across our district, and come up with a possible programme of work.
2) MidCentral Pharmacy Network - what resources are available to tap into and how to leverage the
strengths of the MidCentral community pharmacy network (including MCPG).
3) Digital Health - expand on the technology and communication actions identified that could make
significant efficiency gains and reduce workforce and customer frustration.
4) Workforce (retention and recruitment) - strategies to grow our workforce and retain skills within
the district
A Steering Group has been formed that includes the following members:
MCPG Fiona Bradley, James Carroll, and Clare Hynd
MDHB Graeme Gillespie
THINK Hauora Nader Fattah, Ian Vickers, and Lyn Daly
7Following the second workshop, the Steering Group met to review the draft roadmap and the Networks
prioritised activities. The Group selected a hero project and five smaller projects to focus on over the coming
12-months. The summarised Roadmap is attached. With such willingness from the Network to think beyond
‘what is’ to ‘what could be’, the future of community pharmacy in MidCentral looks bright despite the
challenges.
It is intended that the design and development work required for the focus areas (projects) will be completed
by a mix of MCPG, MDHB, THINK Hauora, community pharmacy, and general practice teams. Working groups
will be established for most of these activities and this will continue to reinforce the strong and collaborative
working relationship between community pharmacy and general practice. Expressions of interest will be
distributed to the network to develop these working groups.
Other ideas and project areas raised at the workshops have not been lost. They have been captured in a
“future possibilities” document to review and consider further in 12-months time.
There is a lot of work that could be undertaken with and for community pharmacy. The Steering Group has
tried to identify the key projects which are achievable and will make the most significant difference to the
Network when achieved. The “Hero Project” has also identified an opportunity to support General Practice
and in turn, create shifts in the way we work across the different parts of the health system and health
workforce in MidCentral.
MCPG are working to distribute the infographic material and the attached Roadmap to the community
pharmacy members so that the members know the outcome of their contribution at the workshops.
3. BUDGET
A budget has not as yet been established however, THINK Hauora will provide skilled resources for some
activity and has agreed to contribute $20k one-off funding to commence these activities. MDHB has
requested a business case be developed in an attempt to seek funding to support the hero project.
A barrier to the success of this work is funding. The intention is to pilot the “Hero Project” in a small number
of pharmacies (after an expression of interest and selection process). The pilot would need funding and also
following an evaluation process, longer term sustainable funding would need to be sourced to allow this work
to continue and be up-scaled to more pharmacies.
4. GOVERNANCE
The Steering Group agreed that, notwithstanding MCPG’s duties to its community pharmacies, the
governance for much of this activity would fit well with THINK Hauora’s Clinical and Digital Governance
Committee (CDGC) as this THINK Hauora Board sub-committee consists of Māori, primary healthcare,
including MCPG, and DHB representation. This established governance body already exists and considers
now any changes to the way we fund and deliver care in our district.
MCPG has endorsed that CDGC governs the Roadmap activity and associated funding.
5. Conclusion
We want to keep the momentum going. Pharmacists are engaged and excited about the possibilities this
work presents.
We ask the Clinical Council to:
- consider the information presented in the infographics for background and,
- understand the global, national and local context community pharmacy operates within and,
- endorse the direction and projects outlined in the Roadmap and,
- consider any key ways to influence and support the work of the Roadmap to help drive it forward.
8Background
Pharmacy in MidCentral Strategy is a strategic document developed between MidCentral Community Pharmacy and MidCentral DHB Planning and Funding in 2018.
Following on from this strategy the MidCentral Community Pharmacy Group (MCPG) and community pharmacies, MDHB and THINK Hauora partnered to complete
a series of pharmacy workforce sustainability workshops based on similar approach taken with general practice teams in the district.
MCPG and THINK Hauora jointly funded Chard Consulting to lead the workshop sessions. Chard Consulting developed a set of infographics with the community
pharmacy network that make visible the challenges and opportunities facing community pharmacy globally, nationally, and locally. The network also developed a
roadmap of activities, based around the concepts in the Pharmacy in MidCentral Strategy, and prioritised the activities that would make the most difference.
A Steering Group has since meet to further review the roadmap and this document provides a high-level overview of the prioritised activities for the next 12-months.
District principals
The Steering Group aims are to:
1. develop and/or share ways of supporting community pharmacy within the community health environment
2. work with the network to address pharmacy workforce sustainability
3. increase access and choice to affordable healthcare for consumers
4. foster an effective partnership to consider new business model opportunities
5. enact the areas of focus within the “Pharmacy in MidCentral Strategy”
6. localise any health system changes
7. improve digital health connectivity, workflows and literacy.
Current roadmap
Themes Prioritised area of focus Actions – initial phase Timing
Workflow redesign (Hero Project) • Establish working group, TOR etc Development stage
• Identify minor ailment type services that can be provided by • Use data to prioritise the most impactful actions – equity March – end of May
Ways of working
pharmacy for acute, low complexity AND long-term lens applied
Design stage
condition management • Develop project plan with stage gates and likely pilot
sites. June – Nov
• Unify triage processes so GPT’s direct patients to the • Develop business case and budget. (mindful of flu/imms pressures)
pharmacy
9Themes Prioritised area of focus Actions – initial phase Timing
Digital Literacy • Establish working group, TOR etc. May – November 2021
• Ensure community pharmacies digital environment meets • Review pharmacies IT infrastructure
interoperability standards • Capture pharmacy systems environment diagrams
(to ensure all parties understand the information systems,
Project is a precursor to other projects apis/transport mechanisms in the current pharmacy environment)
• Check meets with MoH digital, data and tech policy &
nHIP approach
Digital health
• Survey to understand digital literacy – mainly around
cyber risk.
Access to Information • Establish working group, TOR etc. May – December 2021
• Access to the Shared Electronic Health Record (SEHR) • Discuss with network and vendor
• Assess pharmacy IT environment & cyber risk
Need to complete above project first protocols/literacy
• Develop project plan and budget and likely pilot sites
• Implement and adjust PIA
• Comms to the community
Workflow improvements • Establish working group, TOR etc. Development stage
• Improve communication channels and existing processes • Develop project plan and outcomes i.e. key contacts at March – end of May
working
Ways of
between community pharmacy teams (CPTs) and general CPT and GPTs, CPT/GPT rules of engagement for email
Design stage
practice teams (GPTs) etiquette, dedicated line or direct communication
channels between CPT/GPTs. June – Nov
Pharmacy workforce development • Establish working group, TOR etc. April 21 – April 22
• Explore options for promoting pharmacy to school leavers • Develop project plan and outcomes i.e. identify
Workforce
• Explore options for developing intern recruitment and pharmacies that wish to offer internships, promote
retention internships outside of the district, identify continuing
• Explore options for supporting pharmacist education education and post-grad training needs.
requirements / opportunities.
National Advocacy MCPG plan to: April 21 – July 22
• Monitor the Health System Review (HSR) changes on behalf • influence to help ensure that Service Funding and Cost
MidCentral
Pharmacy
Network
of district Pressure Reviews (commissioned via TAS) are not lost in
• Ensure that any health system pharmacy related changes are HSR changes
reflected in the district’s Pharmacy in MidCentral Strategy • identify new service opportunities for community
pharmacy.
10GLOBAL CONTEXT AND TRENDS
Aging People are living longer – average life expectancy is now
population 73.2 years (1950: 47 years) – with health and social
services needed for increasing numbers of older people
Climate Climate change has health and
Chronic The health burden of long-term conditions, such as heart disease, change social consequences
diseases diabetes, depression, dementia and musculoskeletal conditions, is
growing and accounts for an estimated 73% of all deaths
Toxic Toxic air is a global epidemic and is responsible
Multi- Increasing numbers of people – not just air for the premature deaths of 6.5 million people
morbidity the aged – are living with more than each year
one chronic health condition that can
increase medicine complexity
Consumer Consumers have increased health care service/support Wellness The wellness market grew from $3.7 trillion in
Expectations expectations and health literacy (albeit “Dr Google” can culture 2015 to $4.5 trillion in 2019 – growing at nearly
be problematic); emphasis on relationship-based rather twice the rate of the global economy
than didactic service delivery
Health system Health systems are considering ROI across “lifetime of Technology Technology advances and clinical innovation are
decentralisation care”. Positioning care “closer to home” is resulting in transforming healthcare and provide great
more services delivered in, and by, community benefits for people, but are often very expensive
providers. New providers are emerging and may be superseded within a few years
Equity There are inequities in access to health
and in exposure to health risk factors Robotics Use of robots to improve accurate dispensing of
among different groups medicine is increasing; the global pharmacy
automation market is projected to grow from
$5.1 billion in 2019 to $7.8 billion by 2021.
Housing The global housing affordability crisis is increasing,
with a direct impact on the number of people living
in overcrowded or poor housing conditions Information Information technology developments can
revolution make information more accessible and
empower people by giving them ownership
Ways of New ways of working are emerging; increase in online health and of their health information
working wellbeing service delivery and pharmaceutical home delivery
demand, workforce beginning to work remotely, changing primary
Supply COVID-19, political decision-making and low levels of
care workforce roles
chain stock are disrupting/impacting the supply chain
Infections New infections and antibiotic
and resistance are emerging
resistance
Collaboration There is a growing trend towards partnership
and and collaboration across industries, sectors
Global COVID-19 presents unprecedented partnership and organisations
pandemic challenges to public health, food
systems and the world of work
Sources: Worldometer; World Health Organisation; Global Wellness Institute; BCC Research: Pharmacy Automation – Technologies and Global markets
11NATIONAL CONTEXT AND TRENDS
Government Equity Unsustainable models Acute
focus on: National focus on
WIDE
Cost of providing services patient
FUTURE VIEW OF
Mental health addressing inequity in through current model services
Diabetes health outcomes for recognised by NZ Treasury
disadvantaged
RANGE OF
Child poverty, health as unsustainable in the
HEALTH AND
and wellbeing patients and long term
Māori & Pacific peoples population groups
STRATEGIC Vision Adult
DISABILITY SYSTEM
oral
Inequalities in health health
system wages and Growing workforce Acute
DRIVERS shortages in Tertiary &
increasing wage quarternay Behavioural specialist
expectations is health sector, services Well Child Support Care advice
impacting the compounded by an Tamariki coordination
aging workforce Ora
workforce model A connected and Podiatry
School
based
Child &
adolescent
Residential
care
whānau-centred network services oral health
NZ Health Strategy
National focus on Primary mental Community /
Vision
developing a Emphasis on Te Tiriti
of services, that meet health &
General
All New Zealanders
patient-centric, based partnerships
to improve health addictions parent / whānau Practice
Live Well
integrated model of
care, with individualised and wellbeing for people where they are at
Stay Well Māori - Whānau Ora, Home based
Get Well
medicine management
and proactive outreach Mauri Ora, Wai Ora and are supported by Population care & support
health services
simple to access and easy
Community
Emphasis on
collaboration and
Reducing barriers to to navigate systems, tools Physiotherapy Palliative
care
Maternity diagnosis
access calls for closer Planned
networks between
community, primary
to home services and and locations Specialist Outreach
services Needs
Medicines
optimisation inpatient
involving patients, diagnosis services
and secondary health assessment
whānau and community
care to create one in decision making
team Dietetics/
Nutrition Community
pharmacies
Shared data Obesity is becoming
New Zealand has an Potential replacement more common with
aging population of electronic health long-term health and
with increasing record with National social impacts -10% of
multi-morbidity Health Information NZ children are obese Planned
Platform specialist
advice
Source: BMC Health Research: Service provision in the wake of a new funding model for community pharmacy Source: Health and Disability System Review Final Report Pūrongo Whakamutunga March 2020
GENERAL DIGITAL
?
Increasingly complex cases Shortage Consumers have
• Population getting older and sicker of GPs limited visibility of
PRACTICE • 1 in 4 New Zealanders report multimorbidity
• Growing mental health issues HEALTH own information
portals,
Increasing number of
TRENDS
• Primary care consultation rates increasing
faster than population growth Aging
workforce
TRENDS apps, devices and health
literacy websites
Low health provider
digital literacy esp. for
cyber security and privacy
Wait times
pressured Need for more responsive
primary care services
for Maori
Home visits
less frequent
Demand for
services outside
IT infrastructure
investment needed to
improve cyber security
! Data driving health
investment decisions
AFTER HOURS of usual hours
Emerging
transdisciplinary teams
COVID-19 pressure
Clinical guidelines and Integration of health
from increasing costs, change support not always systems high priority (nHIP)
fluctuating patient need, available for digital health changes
Expansion of
General Practice roles burnout/low morale,
uncertainty
12THE CHANGING FACE OF
COMMUNITY PHARMACY IN NEW ZEALAND Increase call on services in
weekend by people
avoiding A&E
ACTIONS BEING TAKEN TO ADDRESS COMPETITIVE THREAT
Developing alternative revenue streams e.g. being part of a funded trial Increasing patient
COMPETITIVE Offering new services and products e.g. natural products expectation for triage in
community pharmacy
IMPACT Changing location – moving into higher traffic areas, locating close to doctors’ surgeries
Combining with other businesses to gain economies of scale and share costs
1 Reduced retail
revenue, decreasing
Minimum standards for pharmacy owners/operators
Investment in digital health/technology to enable access to information
average net profit Promote value of in-person relationships Complex multi-morbidities resulting in
CHA more medicine complexity S
ets
before tax (NPBT) Support for long term / multi-morbidity conditions
N GIN I O N
AT
ark
G NEEDS / EXPEC T
erm
’ es
Sup
t
d g e ci
a 2 Less opportunity to CHANGING BUSINESS MODELS FUNDING MODEL CHANGES
INCRE u
B‘ arm build patient and
ASI ph pharmacist Integrated Community Pharmacy Services Agreement:
N
Changing demographics Number of
ve relationship New Providers community • Introduced 1 October 2018
at i pharmacies • Governs the services pharmaceutical service providers
te r n re Amalgamation
Al lthca can provide
G
h e a • Aims to enable greater flexibility within service delivery
3 People less aware of
COM
Also influenced by individual DHB practices around pharmacy contracts and a more patient-centred services model
support available • Defines services as core, advanced and enhanced
r c h a s e e g
Online pu e ,
through community
COMMUNITY o u s
PETITIVE LAND
Chemist Wa r e h pharmacy PHARMAC:
h , A m a zo n DECLINING NPBT Taking a more directive approach to:
Zoom Healt
PHARMACIES an d o t h e r g l o b a l o n l i n e • DHB spend on vaccines, community and cancer medicines
• Which medicines are funded in primary and secondary care
e s
e t p l a c
4
8
r k
1000 ma Increased risk of
OVER
medicinal harm
NEED FOR REGULATORY CHANGE
Average % of total sales
throughout
6
Busines
ses offe Regulations around
New Zealand retail go ring
o d
offered s traditional
by phar ly 5 Vulnerable business
model - stress and
4 pharmacy ownership have
not kept pace with:
macies
S
challenges around
C
2 • Changing business
A
dealing with models
P
2013
2014
2015
2016
2017
2018
2019
E change, ownership • Changing patient
0
less attractive expectations
• Interpretation of
regulations
To be addressed by the
Therapeutic Products Bill
(still to be passed)
13COMMUNITY PHARMACY’S ROLE
WITHIN PRIMARY HEALTH CARE TOP SERVICES
12
PROVIDED BY
NEW ZEALAND
COMMUNITY
PHARMACIES
Service Funding source
1 Education/advice on prescription medicines to individuals Non funded
2 Education/advice on OTC medicines e.g. cold/flu Non funded
3 Prescription dispensing Core funding
4= Patients registered with LTC service LTC funding
The wider 4= Medicines disposal DHB funding
The broader COMMUNITY PHARMACY HEALTH &
6 Preparation and dispensing of compliance aids (e.g. blister packs) Non funded
COMMUNITY DISABILITY SYSTEM
7 Education/advice on health concerns Non funded
Advice and Delivery of
Dispensing of services (funded,
support for medication 8 ECP consultations Patient/DHB (0-25 yrs) funded
patient non-subsidised
self-management and free) to 9 Extemporaneously compounded preparations services Specific services funding
Community of health improve health
engagement and outcomes 10 UTI treatment (TMP accredited) Patient funded
partnership
11 Home delivery service Non funded
Decision support to
Access and
PATIENT ensure patient 12 Methadone program Specific services funding
Informed, choices support
referral to health outcomes
community-based engagement &
resources
empowered
Connected
Investment in systems and
solutions to clinical
optimise medicine informatics
supply and the WHĀNAU/CARER GENERAL PRACTICE
workforce Proactive & Proactive &
productive collaborative
interaction and engagement with
engagement practitioners
Source: Health and Disability System Review Final Report Pūrongo Whakamutunga March 2020 Source: BMC Health Research: Service provision in the wake of a new funding model for community pharmacy
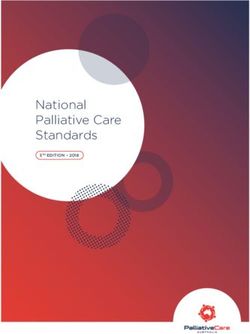
14DISTRICT CONTEXT AND TRENDS
PHO
enrolments:
DISTRICT V NATIONAL
AGING POPULATION 161,408
The aged population is growing, as is the need for aged care. Horowhenua, Ōtaki 65.8% 52.9%
40,714 highly deprived
and Tararua have particularly high proportions of older residents in population
ratio of dependent population
61,529 high needs
(under 15s and over 65s) to working population
YOUNG MĀORI Total population
A greater population of young Māori than old
Māori
26.4% 24%
people in MidCentral live with a disability
Pasifika
MENTAL HEALTH Asian
A greater share of people impacted by 35.4% 32%
mental health than other districts 26%
34% 65 yrs & over
21% estimated obesity
32%
DISABILITIES MidCentral
District attracts people with disabilities population 23% 19.9%
due to being flat, affordable, and having 4% growth
extensive services and programmes adults diagnosed with mood/anxiety disorders
2018 to 2028
REFUGEES
As a refugee resettlement centre, (170 per year - predominantly 38.9k 68% 11%
Afgani, Bhutanese and Myanmar), Palmerston North is dealing Projected number of 36.5k 7%
with health needs that the district has not experienced before General practices not accepting new
people with INCREASE enrolments
multimorbidity
TRANSIENT POPULATION GP FTE demand
Three tertiary institutions and three NZ Defence Forces (who provide medical and
(conservative)
2018 2028
pharmaceutical services for serving personnel) 46% 31%
PEOPLE LIVING IN DEPRIVATION
29.3% of people in MidCentral live in areas designated as most deprived (levels 9-10)
MIDCENTRAL DHB REGION General practices with at least one vacancy
in New Zealand – greater than 60% for Horowhenua and Ōtaki. Some people
struggle to access public transport or have enough petrol to travel distances
proportion of population 25% 15%
Patients cannot get a time when wanting GP or
GROWING ETHNIC DIVERSITY %
By 2030, over 50% of MidCentral people under 25 will not Manawatu 17 nurse healthcare
record New Zealand European as their main ethnicity %
MidCentral
Palmerston North 49 District GP shortage continues
GREATER VOLUMES
%
Three age groups with greater volume than nationally population Tararua 10
1 0-4 184,200
2 Students % 120
3 80 and over
Horowhenua 18 115
GP FTE demand
%
Ōtaki 6 2018
GP FTE supply
2028
Sources: DHB population profiles 2018-2028; MDHB: Pharmacy in MidCentral Overivew 2018 2018 NZ Index of Multiple Deprivation NZ Medical Workforce Survey 2019; General Practice workforce Survey (TRNZCGP) Report
$3.5+ billion of initiatives bringing people to the district (not included in population projections)
Ohakea Turitea Taraika Napier Linton
Gorge
270 – 2,500 wind turbines Horowhenua Kiwi residential Road Camp
Transmission Road
people 140 people Business Rail development $50m $89m
Gully 500
$239m – $256m Park $200m ~ 2500 houses people
$289m
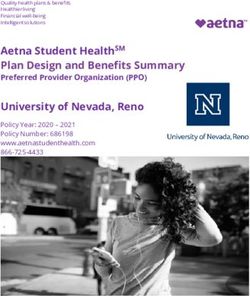
15COMMUNITY PHARMACY COVERAGE & SERVICES
ACROSS THE DISTRICT
NUMBER OF COMMUNITY PHARMACIES PROVIDING SERVICE
NUMBER OF Feilding
Dannevirke
PHARMACIES Sanson 2 1 Number of community pharmacies providing service
0 Community pharmacy services
Across district
Palmerston Nt
Horowhenua
Manawatū
Ōtaki
Tararua
(Levin, Foxton)
(Fielding)
(Dannevirke, Pahiatua)
Ashhurst
Rongotea 0 Woodville
0 Palmerston Depot Var
Himatangi North iety After hours 8 5 0 1 0 1
mo of
0 20 del bus
DIF s an ine Vaccinations 13 10 1 1 0 1
FER d ss
PHA ENT Long term conditions programme 32 21 5 3 1 2
Pahiatua R M
acr AC IZE S
Foxton oss Y TE Age-related residential care services 7 4 1 1 0 1
1 1 the AM
dist S Community residential care services 10 5 1 1 1 1
rict
MC Emergency contraceptive pill 30 19 5 3 1 2
coo PG
rd i
of i nat =
nfo or Paediatric gastroenteritis 32 21 5 3 1 2
rma
Shannon tion Smoking cessation/vaping service 30 20 4 3 1 2
0 Clozapine services 11 5 3 2 0 1
Levin People
access pharmacy CPAMS (anti-coagulation management) 4 0 2 1 0 1
5 in different ways Methadone services 24 14 5 2 1 2
and places All MidCentral
Subsidised special foods service 32 21 5 3 1 2
community pharmacies
also provide: Total number of pharmacies 32 21 5 3 1 2
Under 14s after hours dispensing
Ōtaki Does not include Woodville depot
Sharps container disposal
1 Mental health high frequency dispensing Source: MDHB: Pharmacy in MidCentral Services Overview 2019
prior to Fielding pharmacies going from 3 to 2
Safe and efficient disposal of unused medicines Tec
(SEDUM) hn
Mid olog
Cen y u
me tra sed
dic l f in
DISPENSING TU A N N O R T H N U A I
ati o
on r disp
W A
A 9 Pharmacists A R U
S T O
W HE K
TA 2
:T
ON ensin
WORKFORCE R 7 Pharmacists R 52 Pharmacists 12.9 Pharmacists Pharmacists
IQ g
N
Ō
O
TA
E
2020 MCPG
MA
HOR
PALM
workforce data Technicians
13 8.5 Technicians 59 Technicians 22.9 Technicians 2 Technicians
0 Interns 0 Interns 6 Interns 2 Interns 0 Interns
3 Pharmacists to 10,000 3.9 Pharmacists to 10,000 6.1 Pharmacists to 10,000 3.9 Pharmacists to 10,000 2 Pharmacists to 10,000
7.6 Dispensing 9.2 Dispensing 13.8 Dispensing 10.8 Dispensing 3.9 Dispensing
workforce workforce workforce workforce workforce
to 10,000 to 10,000 to 10,000 to 10,000 to 10,000
Numbers per role are headcount not FTE – some work part-time 16OUR NATIONAL PHARMACEUTICAL WORKFORCE
WORKFORCE WAYS OF SUPPLY/DEMAND
WORKING
Relatively young workforce More women than men Work 40+ hours per week Growing workforce – and likely to continue to grow
4000
42% me 59%
Pharmacists
(including pharmacist prescribers)
female male
dia
under 35 years 3000
t s
37.6
n age
ac i s t s
a r m sta n 66.6% 33.4%
Ph s s i years Stress in community pharmacy 2000
rib i n g
a c yA 18%
e s c rm s t s
Pr Pha r mac i
55 years + Pharmacists twice 1000 Non-practising Pharmacists
P h a
150-200 scripts per as likely to make * Intern Pharmacists
Pharmacist = guideline dispensing errors 0 Pharmacist Prescribers
for safe workload by the when operating 2016 2017 2018 2019 2020
n s Commitment to study and training
ici a Australian pharmacy board under high stress
c h n
c y Te (Source: IPANZ) *Deferral of mid-year assessment centre, due to the COVID-19 pandemic, has resulted in
rm a Pharmacist 96% graduate from the University of Auckland or Otago reduced transfers from the Intern Pharmacist scope of practice to Pharmacist, reflected by
Pha year tertiary
the increased number of currently registered interns
qualification
- final year as intern 13% hold a postgraduate clinical qualification in Early Career Community
medicine management Pharmacists* But overall capacity staying the same…
10 years or less experience post-graduation
Practicing Pharmacists per 10,000 population
pharmacists commit to ongoing training and education ECPs describe a flexible working
Prescribing MOST
– often after hours environment as having enough staff or 8
Pharmacists
access to locums to easily cover leave/time 7 2,418 pharmacy
Additional
off or not stress about taking leave technicians
years of 57% ECPs* use online discussion groups to connect with colleagues
6
study 5
(Census 2018)
88% 4
Pay levels for dispensing workforce (www.careers.govt.nz) describe day-to-day work as moderately 3
Demand expected
or extremely stressful 2
to grow by 9%
Pharmacy Pharmacist 1-5 Pharmacist 5+
2016
2017
2018
2019
2020
Interns 1 over next decade
technicians years’ experience years’ experience
$45,000 $42,000- $50,000- $75,000- 0
per year
$xx,000 $75,000 $100,000
Why Pharmacists stop practicing
Pharmacy workforce diversity Types of pharmacists
60% Seeking employment Not
renewed
African experience burnout or significant Full-time study status
Indian unmanageable stress
Middle Other health
Eastern Other profession Overseas
Asian Community
European pharmacists Building careers
Other Māori Retired
Pasifika 65%
are satisfied with their career Other
New Zealand
European Other Parenting
Hospital leave Non-health
MOST role
pharmacists
General Practice
want better information on career
Teaching research oportunies and pathways
Pharmaceutical industry Source: Pharmacy Council Annual Report 2019; Pharmacy Council Workforce Demographic Report 2020;
DHB
Pharmacy-related
www.careers.govt.nz; PSNZ Early Pharmacists’ Consultation: Building Blocks Report July 2020
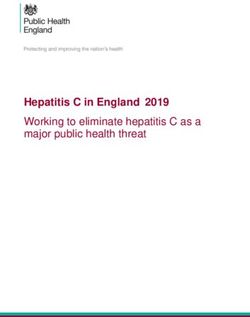
PHOs www.career.govt.nz 17OUR DISTRICT PHARMACEUTICAL WORKFORCE
WORKFORCE WAYS OF WORKING SUPPLY/DEMAND
Estimated pharmacist headcount to 10,000 people
Relatively young workforce, but an older
profile than NZ wide
i s t s
mac nt s GP DEMAND
Ph a r
s s ista SHORTAGE FOR
rib i n g
a c yA 42% 29% PHARMACY
SUPPORT
e s c rm s t s Northland 6.13
Pr Pha r mac i under 35 years 55 years +
Ph a
Auckland 9.88
a n s
h n ici Counties Manukau 6.98
Te c Role Number practising in MidCentral
macy MidCentral Waitematā 9.11
h a r As at March 2020
P Bay of Plenty 8.31
has the
Waikato 5.74
SIXTH LOWEST
Pharmacists Hauora
83 number of Lakes 5.62 Tairāwhiti 5.71
pharmacists Taranaki 8.33
Whanganui 6.82 Hawke’s Bay 7.85
Hard to fill vacancies to population
MidCentral 5.82
Intern Pharmacists 8 of all Wairarapa 4.68
New Zealand Nelson
Hutt Valley 8.08
Marlborough 8.69
DHBs Capital & Coast 8.58
West
Coast 4.94
Pharmacy Technicians 105 Stress/burnout
(including trainees) Canterbury 8.29
South Canterbury 5.98
Other Clinical Support Staff 47
Like other parts of
Less time for patients Southern 9.55 New Zealand,
MidCentral has
pharmaceutical
workforce vacancies
Pharmacy expertise also provided
outside of community pharmacy
through the hospital and the primary
care support pharmacy team Lack of district
Medication errors locums (only 3-4
(8% of patients experience a prescribing or
dispensing medication error) now serving
district)
Source: Pharmacy Council Workforce Demographic 2020, MDHB Pharmacy in MidCentral Services Overview 2019; MCPG data 18COMMUNITY PHARMACY
INSIGHTS
STRENGTHS WEAKNESSES
• Resilient, highly qualified and competent workforce that delivers • Process issues between GPTs and pharmacy cause pressure and resentment
• Group of people who are passionate about health care delivery • Contract rules negate ability to charge to offset increasing coordination of benefits
• Pharmacy as a group is adaptable and strongly focused on problem solving (as evidenced during COVID) • Business efficiencies don’t always lead to better patient care e.g. loss of personal connection
• Strong local relationships with consumers – a friendly and available “face” in the community • As a SME, cost of doing business, adhering to legislation, changing market and demands etc.,
are impactful yet no obvious plans to collaborate or consolidate between pharmacy owners
• Offer local and essential services
• A lack of data to identify population health continuous improvement opportunities and
• Same day service/delivery demonstrate pharmacies’ value/return on investment within the health system
• Locally Eclair is a useful information system • Inability to influence stock supplier relationships
• Quality processes reliability reduces medicines related harm • Increasing demand for services with no associated funding stream
• MidCentral district has a representative group (MCPG) for collaborative projects with DHB and/or PHO INT • Retail revenue diminishing, increased transaction costs (credit cards + payWave) INT
ERN ERN
AL • Challenges around recruitment and retention of rural workforce AL
• Limited voice nationally to influence policy
• Pharmacy owners act independently
OPPORTUNITIES BARRIERS
• Promote “shop local” to maximise relationship potential • Changing environment is pressuring financial viability and workforce resilience
• Promote that relationships improve self-management and medicines adherence • Consumer affordability and expectations are noticeably changing which doesn’t always match
the pharmacy business model
• Develop a business case around the benefits delivered by community pharmacy around medicines literacy and
adherence due to strong consumer relationships • Current commissioning/funding approach drives behaviour i.e. doesn’t always think about the
patient journey, lack of discretionary funding
• Work collaboratively with other community providers on community solutions (have a voice in the community)
• Inability to influence stock supply commissioning/management
• Agree a community pharmacy change programme to help owners get ready for upcoming health review changes
• Some auditing processes may not add value
• Increase the range of community clinical services available/funded via community pharmacy
• Insufficient collaboration with other healthcare providers to ensure community pharmacy
• Use stock and dispensing data to reduce medicines waste services are well utilised
• Develop digital health tools to create efficiencies and better access to information • Mixed perceptions around benefits of prescribing pharmacy training
• Promote pharmacy as an achievable health career option EXT EXT
ERN • Disconnected IT systems and processes can cause risk, inefficiency and communication issues ERN
• Centralise prescribing via commonly used health system tools i.e. Medimap AL AL
• Take advantage of the “digital age” - online awareness, information distribution
• Promote a national voice for pharmacy that improves legislation and pharmacy sustainability
19FROM OUR EXPERIENCES
NAVIGATING COVID-19…
We need to get better at... We need to retain and build on...
Funding Prescriptions
• Accessing funding for minor ailments • E-prescribing practices (with improved functionality)
• DHB funding negotiations • Synchronised medication supply
• Advocating for service funding currently performed at no charge
Patients
Digital health • Good relationships with patients – increased trust, people
view pharmacy as more important,
• Using technology to enable ease of communication between
pharmacist and GPT, particularly around script messaging • Being accessible to patients for information, vaccinations,
minor ailments, advice
• E-prescribing technology stability - need practical ‘one system’
• Managing patient expectations e.g. speed of service,
• One national health system/database
counselling etc.
• Accessing IT support
• Managing patient expectations around speed of service /
wait times (e.g. patients calling ahead)
Communication
• Feedback via NZePS (through MOH) Staff
• GP and community pharmacy communication channels • Safe working practices e.g. less exposure to illness
• Streamlining communications re repeats/wastage (keep using screens)
• Allocating time/reducing script pressures for patient conversations • Medicine charts
• Collaborating with other health providers around patient care • E-access to detailed patient information via patient
management system and shared electronic health record
Patients
Vaccinations
• Managing patient expectations around access to ‘their medicine’,
and wanting to get the whole amount even if not needed • Increased vaccination coverage, especially flu vaccines for
people with long term conditions
• Triaging minor ailments
Communication
Business
• Improving people’s knowledge of pharmacy services
• Ensuring business models develop clinical roles within and roles
community pharmacy
• Using information and communication forums provided
• Retaining revenue / covering loss of income by MCPG
20SUSTAINABLE COMMUNITY PHARMACY
Workforce d
• Develop a
evelopment
d istrict pharm
developmen acy workfor
t framework ce
retention, re encompass
cruitment a ing
developmen nd professio
t aims nal
Digital h
m
eal
e
t
n
h
t
• Promote p
• Develop a
harmacy as
n intern pro
a great plac
e to work
develo p gramme
h • Develop a
i ca t i o n w i t recruitment
e c o m m u n programme
• I m p r o v
providers t i o n
in f o r m a
e a c c e s s to
• I m p r o v
i c e s w h e r e
e a l t h s e r v
i l i s e te l e h
• Ut
p p r o p r i a te
a l t h
d i g i t a l h e a
i m p r o v i n g
• Fo c u s o n
con n e c t i v i t y
u c t u r e Ways of working
i n fra s t r
e c h n o l o g y
t
• R e v i e w • Identify and promote minor ailment
type services
• Participate in MDT meetings
• Discuss different ways of working with
the hospital and ARCs
• Grow understanding with the district
Pharmacy collaboration primary health
• Arrange opportunities for pha • Identify new service opportunities
rmacy to meet
and collaborate on topics of inte through legislation
rest
• Create learning environments • Grow and communicate pharmacy
where we
share/learn from each other triage before contacting GP
• Arrange opportunities for pha • Support consumer medicines literacy
rmacy owners
to meet and think strategically
about
sustainable pharmacy business
models
• Discuss how staff and resourc
es
can be shared
21SUSTAINABLE COMMUNITY PHARMACY
Workforce d
evelopment
• Advocate
health fo r remunerat
Digital g e s w i t h i n
reflects year
responsibili
s of study an
ion that
d level of
e fo r c h a n ty
• Advocat orrect repeat
c • Advocate
NZePS to l in k c o d e t o for support
for recruitin
m s a n d retaining wo
proble rkforce g and
patient
I Q a r o u n d
k w i t h TO N
• Wor r o v e m e n t s
te m i m p
sys n al
n g to n a t i o
e s s a g i
• Enable m tal
t i e n t p o r
pa
Ways of
• E n h
wo
a
rk
n
in
c
g
e a u d i t in g
-
p
fo
r
c
o
u
c
s
e
e
s s
d
e s to
a r n i n g
be more le
Community pharmacy m e a s u r e a n d
• Find ways to o f t h e
s i b i l i t y
visibility and advocacy increase vi i t y
c o m m u n
complete r o v i s i o n
i c e p
• Expand the definition of community pharmacy pharmacy serv
services to include non-service work
• Advocate for increased funding for services
and ‘the things we do every day’ (non-funded)
• Advocate for legislation changes
• Grow the community pharmacy voice at
national level and across primary health care
• Heighten understanding around the
role of community pharmacy and
current/potential efficiencies
community pharmacy can provide
primary health care
22Clinical Council Focus Areas
2020-2021
LEAD/
ITEM INFLUENCE MONITOR FREQUENCY RESPONSIBLE DATE METHOD
INITIATE
Equity
Tracee Te Huia, Maori health indicators – Deep dive
Maori Health General
TBC
Manager, Maori
Health
Hauora (Whanau
TBC
one stop
Patient
TBC
Experience
Workforce
Keyur Anjaria, Ensure the workforce has the
General resources and skills required.
Manager, Mixed ethnicity and diversity within
People and the workforce
Culture Workforce encouraged to work to
Workforce TBC utilise skills/specialties to ensure the
greatest impact
Initiate District wide workforce plan
Staff survey results
Unintended bias and racism in the
workplace
Kath Cook, Clinical Council to influence
CEO Communication between
Intersectoral MidCentral Universities/Tertiary partners
Development DHB and Discuss progress with Kath Cook and
Kelvin May 2021 potential involvement of Council in the
Billinghurst creation of a workplan
Chief
Medical
Officer
23Understand health workforce outside
Workforce plan of the hospital – district wide
workforce plan
Digital
Sue Pond, Project Support base value of telehealth based
Manager, EPMO, on patient feedback
Telehealth Bronwen Warren, Request telehealth utilisation report
Programme including acceptability by patients
Manager, EPMO
and Barbara Ruby,
Planning and
Integration Lead,
Acute and Elective
services
Steve Miller, Chief TBC Clinical Council to continue to support
Digital Officer, IT/Digital health. Functioning digital
IT Platform Digital Services platform will reduce errors and
improve communication.
Mental Health
TBC Nicola to bring to Clinical Council
CAFS meeting to determine how the Clinical
Council can support
Vanessa Caldwell, TBC Vanessa to attend and present to
INF (Ward 21 Clinical Executive, Clinical Council
Design) Mental health and
Addictions
Raeleen Toia, TBC Raeleen to bring to Clinical Council
Te Ara Rau Clinical Council meeting to determine how the Clinical
Member Council can support
Chris Hocken, TBC Chris Hocken to attend the Clinical
Consumer Projects Council meeting to discuss.
PT Experience lead, Mental health MARAMA “Real time feedback” IPAD
and Addictions board
24Communications
• Screen saver – Jodie Hickey to
book, Clinical council members to
determine the content
Promote the • Sound bite – Regular
Clinical Council Communications to workforce
• Profiles – Profiles to be set up and
updated as required
• Portals- use of to promote eg Child
Health
Mar 2021 Work with Jonathan to develop useful
two way interactive site
Website
Operational
TBC Clear referral process/criteria to
ensure patients’ needs are meet
Health Pathways
Colin Thompson, TBC Fiona to lead in pharmacy initiative
Medical Advisor Service integration and delivery
Diabetes
Kath Cook, CEO May 2021 Review progress
Facilities MidCentral DHB Continue to monitor
Development
25Two way pairing network brings issues
Cluster/Delivery to Council’s attention
Planning
Judith Catherwood, Feb 2021 Assist in effective CG model and
Clinical General Manager, deployment
Quality and
Governance
Innovation and
Kelvin Billinghurst,
Chief Medical
Officer
Clinical Council achievements 2017-2020
• PANE service
• Chair of Council on FRAC
• Te Awa governance- seat (2 by chance) on the governance of this important work
• Review of major projects- including “speaking up for safety”, staff survey (MCH), CNS review, Lab services Contract, DHB Pharmacy Contracting,
Integrated Service Model, Locality Planning
• Community pharmacy facilitation and establishment of conjunctivitis treatment in Retail Pharmacy
• Mental Health- ward 21 re-build
• Cluster pairing establishment
• Referral process, medical letters and general communication secondary to primary
• Facilities review- mitigation plan (together with Combined Medical Staff) and influencing strategic building plan
• Equity issue – influencing and monitoring Maori Health Outcome Indicators
• Consumer Council- chair’s presence on Consumer Council, two way influence, joint programme of Councils with Mental Health, Equity and shared
patient/whanau centered interest model.
• Engagement in MDHB strategy refresh
26• Clinical Governance - development of the quality agenda, shared governance approach and the new committee structures
27• Schedule of Matters Arising
Matter Raised Scheduled Responsibility Method Status
Facilities Development – Clinical 4 Sep 19 5 May 2021 Judith Catherwood, Verbal Ongoing
Council to continue to follow the General Manager Update/Report
facilities development progress Quality and
Innovation
Persistent Pain Service, Clinical 4 Sep 19 7 April 2021 Deborah Davies, Primary, Report Open
Council to follow the Implementation Public and Community
of the Persistent Pain Service. Health
Te Awa Strategy – Clinical Council to 4 Sep 19 TBC Steve Miller, Chief Verbal Update Open
Follow the progress of the Te Digital Officer
Awa Strategy.
Clinical Council to continue to support 7 Aug 19 TBC Judith Catherwood, Verbal Update Open
the development of the Clinical General Manager, Quality
Governance Framework and
Innovation/ Dr Simon
Allan, Clinical Council
Chair/ Clinical Council
Members
Communications – Clinical Council to 4 Sep 19 TBC Dr Simon Allan, Clinical Report Ongoing
work with Communications on ideas Council Chair/Jodie Hickey,
to boost profile and keep audiences Clinical Council
updated on initiatives the Clinical Administrator
Council are involved in.
Work Program 2019/20 to be 2 Sep 19 ongoing Dr Simon Allan, Clinical Workshop Open
developed. Fluid document, to be Council Chair
brought back to each meeting and
updated as items of interest arise
Primary Care Workforce 12 Mar 21 2 Jun 21 Chiquita Hansen, CE Update Ongoing
THINK Hauora
28MIDCENTRAL DISTRICT HEALTH BOARD
Minutes of the Clinical Council meeting held on Wednesday 3
March 2021 at 5.15 pm, Board Room, Palmerston North Hospital
CLINICAL COUNCIL MEMBERS PRESENT
• Dr Simon Allan (Chair)
• Dr Don Baken
• Fiona Bradley
• Dr Nader Fattah
• Sophie Loveridge
• Jane Ayling,
• Dr Garry Forgeson
• Dr Nicola Pereira
• Raeleen Toia
• Celeita Williams
• Gail Munro (ex-officio)
IN ATTENDANCE
• Judith Catherwood, General Manager, Quality and Innovation
• Chiquita Hansen, CE THINK Hauora
• Dr Paul Cooper, Medical Advisor Acute Care
• Kelvin Billinghurst, Chief Medical Officer
• Jodie Hickey, Committee Administrator
1. KARAKIA
2. APOLOGIES
Apologies were received from Council Member Tim Dunn
3. NOTIFICATION OF LATE ITEMS
There were no items raised.
4. CONFLICT AND/OR REGISTER OF INTEREST
There were no items raised.
5. IMPROVED ACCESS TO PRIMARY CARE
Chiquita Hansen and Dr Paul Cooper attended to discuss steps that are been
taken to alleviate the issues with access to primary care in the MDHB region.
Members engaged in a robust conversation. Ideas and potential solutions to
specific issues were discussed.
29You can also read