Multiple Sclerosis in the Underserved: Updates in Symptomology, Pharmacology, and Practice - Academy of Neurologic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Multiple Sclerosis in the Underserved:
Updates in Symptomology,
Pharmacology, and Practice
Thursday, February 22, 2018
CSM, New Orleans
Speakers
Sara Migliarese, PT, PhD, NCS, Associate Professor, Winston-Salem State University
Doris Molina-Henry, PhD, Assistant Professor, Winston-Salem State University
Prudence Plummer, PT, PhD, Associate Professor, University of North Carolina at Chapel Hill
Session Objectives • Identify the most common symptoms associated with MS in underserved patient populations and compare those to that of adults from majority US populations. • Identify health inequities that exist for adults with MS from underserved populations.
Session Objectives • Describe recent updates in pharmacological interventions for MS and understand the variations in responses to those regimes in underserved populations. • Apply current research in MS to the treatment of common mobility complications experienced by underserved populations. • The speakers have no disclosures to declare.
Session Outline: Introduction • 11:00 – 11:40 • 1) Discuss MS epidemiology and prevalence for majority and underserved US populations. • 2) Describe the most common MS symptoms exhibited by underserved US populations and compare/contrast them to majority populations. • 3) Discuss the health inequities that exist for underserved adults with MS and how that impacts physical therapy practice.
Pharmacology and Multiple Sclerosis • 11:40-12:15 • 1) Overview of pathophysiology and current pharmacological agents in the management of MS. • 2) Describe potential pathophysiological explanations for the variations in MS symptoms observed between underserved US populations when compared to the majority of the population. • 3) Discuss the variations in response to key pharmacological agents and health inequities that relate to pharmacological therapies experienced by underserved populations.
Status of the Evidence for Mobility Rehabilitation in
Multiple Sclerosis
• 12:15-12:50
• 1) Critically appraise the current evidence for various rehabilitation
approaches (e.g., strengthening, aerobic training, gait training with or
without robotic assistance, dual-task training, balance training) to improve
mobility in MS, including gait speed, endurance, functional mobility, and
fall risk.
• 2) Discuss current evidence limitations and knowledge gaps regarding
mobility rehabilitation in MS.
• 3) Describe the steps needed for best practice implementation and
considerations for building the evidence base to guide physical therapy
practice in MS.
• 12:50 – 1:00 : Questions & AnswersSession Outline: Introduction
1) Discuss MS epidemiology and prevalence for
majority and underserved US populations.
2) Describe the most common MS symptoms exhibited by underserved
US populations and compare/contrast them to majority populations.
3) Discuss the health inequities that exist for underserved adults with
MS and how that impacts physical therapy practice.
SJM2018CSMBrief Overview of MS
• Chronic recurrent inflammatory disorder of the CNS
• Injury to myelin sheaths, oligodendrocytes, and to a lesser extent, the
axons and nerve cells themselves
• Symptoms vary depending on location of plaques within the CNS
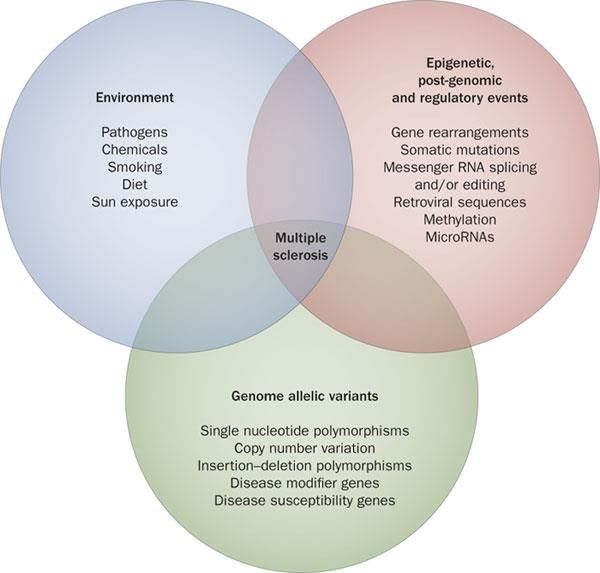
• Thought to be an interaction between genetic predisposition and
environmental factors
• MS types were defined in 19961
SJM2018CSMRevised Phenotypes of MS
• 2014 new recommendations were published in Neurology1
• Retained & refined former 1996 descriptors to separate types of MS
based on disease activity (clinical relapse rate and imaging findings)
and disease progression1
• Added Clinically Isolated Syndrome (CIS)
• Added Radiologically Isolated Syndrome (RIS)
SJM2018CSMModifiers of Basic Phenotypes of MS
• Relapsing-Remitting – ACTIVE (RR-active) (worsening vs. progressing)
• Relapsing-Remitting – NOT ACTIVE (RR-not active)
• Primary-Progressive – ACTIVE (PP-active) (former PRMS)
• Primary-Progressive – NOT ACTIVE (PP-not active)
• Disease activity is defined by clinical assessment of relapse occurrence or
lesion activity; progression is determined by degree of disability worsening
• Eliminated Primary-Relapsing MS with inclusion of disease activity modifier
SJM2018CSMModified by Disease Progression
• Primary-Progressive MS – not progressing (PPMS – not progressing)
• No change in past year
• Secondary-Progressive MS – active & progressing (SPMS – active &
progressing)
• For RRMS- use the term ‘worsening’ in place of progressing and only use
‘progression’ for those in the progressive phase of MS
• Use ‘benign’ and ‘malignant’ with caution
SJM2018CSMCommon Signs & Symptoms & Prevalence2
• Fatigue 83.1%
• Heat sensitivity 80.0
• Difficulty walking 67.2
• Stiffness & spasms 63.1
• Bladder problems 59.8
• Memory & other cognitive problems 55.8
• Pain & other unpleasant sensations 54.3
• Emotional & mood problems 37.5
• Vision problems 37.4
SJM2018CSMCommon Signs & Symptoms & Prevalence2
• Dizziness or vertigo 36.2%
• Bowel problems 34.5
• Tremors 30.2
• Sexual problems 29.9
• Difficulty moving arms 23.5
• Swallowing problems 21.8
• Speech problems 20.2
• Seizures 2.1
SJM2018CSMUnfavorable Prognostic Indicators2
• Male
• Onset of symptoms after 40 yoa
• Initial symptoms involving cerebellum, mental function, or urinary
control
• Initial symptoms that affect multiple regions of the body
• In the first years after onset, attacks are frequent, or short time
between first 2 attacks
• Incomplete remissions
• Rapid progression to disability
SJM2018CSMEtiology
• Presumed autoimmune disorder3
• Complex interaction among genetic predisposition, sex, environment
• Uncertainty about role of race. MS differs in both incidence and
clinical expression for different ethnic groups4
• Minority populations have a higher incidence (newly diagnosed cases)
of MS compared with their ancestral countries of origin4
• Only 1% of research literature address minority populations with MS5
SJM2018CSMSJM2018CSM
General Prevalence5,6
• 2.3 million world wide
• 1 million in the US living with MS
• 65% with RRMS eventually develop SPMS
• 15% diagnosed with PPMS from onset
• Most diagnosed between 20-50 yoa
• More common in Caucasians of northern European ancestry, farther
from equator, but prevalence varies
• 3 x more common in women than men (hormones may play a factor)
SJM2018CSMNewer Data on US Incidence
• Khan 20157 study that reviewed incidence:
• 1 million people in US living with MS
• 10.2 % rate in AA and 47% increased risk of MS when compared to
Caucasians
• 6.9 % rate in Caucasians
• 2.9% Hispanic Americans with 50% lower risk when compared to Caucasians
• 1.4% Asian Americans, 80% lower risk when compared to Caucasians
Similar findings in large Gulf-War-era military veterans study
SJM2018CSMDebunking the MS myths
• The idea that African-Americans don’t get MS was based mainly on
two pieces of data:
• A 1979 study of 5,300 World War II and Korean War veterans that
found that Caucasian males were approximately twice as likely to get
MS as AA males
• The overall lack of MS diagnoses among black people in Africa
• Need better data!5
SJM2018CSMKey to the Discrepancies
• Out of nearly 60,000 published articles about MS, only 113, or about
0.002 percent, focus on African-Americans5
• Some previous studies show that African-Americans, particularly
females, are actually diagnosed with MS much more frequently than
people of European descent
• Recent studies indicate the opposite findings
SJM2018CSMMore Recent Findings
• A 2012 study of military personnel published in Military Medicine
reported 46 % more cases of MS in blacks than in non-Hispanic
whites.7
• A 2013 study of 496 newly diagnosed people conducted by Dr.
Langer-Gould found that blacks had a 47 % increased risk of MS
compared with whites. The study also found that among blacks,
women had triple the risk of MS compared with men.5
SJM2018CSMIs MS new or Underrecognized?
• 26 % of blacks have a family history of MS, a rate similar to that of
whites. “So it could be that it’s not a new disease in African-
Americans, but just under-recognized.”
• Theory: people with darker skin tones don’t transform sunshine into
vitamin D as easily as people with lighter skin and thus may have an
increased risk of MS.
• Not found in Langer-Gould study: “But that doesn’t explain why our
study showed that Hispanics and Asians have a lower risk of MS than
Caucasians.”5,8
SJM2018CSMWhy the Under-representation?
• Minorities not represented in most research studies
• Legacy of distrust (Tuskegee Syphilis Experiment)
• Tradition of self-help (hide symptoms and rely on themselves)
• African-American women may have the superwoman mentality….no
room in their life for MS…it’s just “stress”
• No government requirement to track MS, so numbers may be
scientifically sound. 1 million in US living with MS (23,000 are
veterans) via MS Prevalence Initiative in 20143
SJM2018CSMDifferences in Ethnic Cohorts with MS Related
to Incidence
• African-Americans develop MS at half the rate of white Americans :
one in 1,500 rather than one in 750 (Inside MS Oct-Nov. 2016)4
• Diagnosis for AA may be faster (one year from onset) (USCF study) vs.
2 years for white Americans5
• Not the same stats for a neighborhood clinic looking for ailments
more prominent in populations (HRN, DM, high cholesterol)
• Not everyone agrees that ethnicity does not impact speed of
diagnosis
• Treatment is different
SJM2018CSMHispanic and Asian Americans8
• Incidence for Hispanics: 8.2% vs. Caucasians at 9.3% and AA at 12.1%
• Mortality highest among whites, then blacks, Hispanics, American
Indians/Alaska Natives, and then Asians and Pacific Islanders
• Mortality highest for whites after age 55 and highest for blacks,
Hispanics, and Asians younger than age 55
• More severe disease course for minorities may contribute to this
increased mortality rate, greater opticospinal MS
• Onset for US-born Hispanics at younger age
• Degree of disability is worse for immigrant Hispanics
SJM2018CSMSession Outline: Introduction 1) Discuss MS epidemiology and prevalence for majority and underserved US populations. 2) Describe the most common MS symptoms exhibited by underserved US populations and compare/contrast them to majority populations. 3) Discuss the health inequities that exist for underserved adults with MS and how that impacts physical therapy practice.
Clinical Picture Regardless of Prevalence &
Incidence5,8
• MS can manifest differently in African-Americans
• Average age onset in AA = 38.3 years
• Onset differs by geography (east vs west US)
• 1-2 year delay in diagnosis
• AA have higher Multiple Sclerosis Severity Score (MSSS) than whites
at diagnosis (5.6 vs. 4.5)
SJM2018CSMSymptomology & Disease Presentation8
• African Americans are more likely to experience more relapses (after
48 weeks) & shorter time to second MS attack
• More likely to have multifocal signs from the start
• Greater lesion volume, atrophy and diffuse tissue damage on
neuroimaging
• African Americans are more likely to experience greater disability and
poorer recovery
• African Americans are at greater risk for needing ambulatory
assistance earlier in the disease course
SJM2018CSMSymptomology & Disease Presentation8 • African Americans are more likely to develop involvement of the optic nerves and spinal cord (opticospinal MS) and inflammation of the spinal cord (transverse myelitis), cerebellar dysfunction, and cognitive dysfunction • Optic-spinal MS in AA = 17% vs. 8% in Caucasians • Transverse myelitis in AA = 28% vs. 18% in Caucasians • Onset of MS is generally more severe
Unfavorable Prognostic Indicators2
• Male
• Onset of symptoms after 40 yoa
• Initial symptoms involving cerebellum, mental function, or urinary
control
• Initial symptoms that affect multiple regions of the body
• In the first years after onset, attacks are frequent, or short time
between first 2 attacks
• Incomplete remissions
• Rapid progression to disability
SJM2018CSMMSFit9
SJM2018CSMMSFit9 SJM2018CSM
Impact of Increased Disability in MS
• Increased risk for osteoporosis10
• Increased incidence of falls (typically low trauma stumbles/falls)
• Mild disability = 41.6% fall at least 1x/yr., 66.4% mod disability, 62.1% severe
• Increased immobility leading to low bone mineral density (BMD) and
fracture risk
• Repeated courses of corticosteroids, muscle weakness, and vitamin D
deficiency may also impact BMD
SJM2018CSMWhat Does Gait Look Like in More Disabled
Adults with MS?
SJM2018CSMGeneral MS Gait Characteristics &
Disability11,12
• 90% have gait instability and 50% fall13
• Significant reduction in velocity & step length
• Increase in cadence to compensate for step length & maintain speed
• Increased spasticity in hamstrings (increased knee flexion by almost 7
degrees at heel strike)
• Increased spasticity in ankle plantarflexors
• Extended activity of the tibialis anterior during swing and sustained
during early stance
SJM2018CSMBy Gait Cycle
• Initial Contact and Loading Response
• Increased spasticity in ankle plantarflexors
• Extended activity of the tibialis anterior during swing and sustained during
early stance
• Mid stance and terminal stance
• Increased dorsiflexion angle due to flexed knee
• Increased quadriceps activity and plantar flexors, but not increased knee or
hip extension ROM
SJM2018CSMGait Cycle continued
• Pre-swing and toe-off
• Excessive dorsiflexion leads to increased heel contact and tibial forward tilt
• Decreased plantarflexion propulsion force
• Ultimate decrease in gait speed
• Swing
• Hip flexor activity increased to carry limb through swing due to decreased
propulsion forces at toe-off
• Take home message: AA tend to have more disability involving gait
SJM2018CSMCombating Osteoporosis in MS10
• Educate lifestyle changes such as
• Smoking cessation
• Reducing alcohol intake
• Increasing physical activity, progressive resistance training
• Optimizing vitamin D status
• Fall prevention to avoid fractures
SJM2018CSMSession Outline: Introduction 1) Discuss MS epidemiology and prevalence for majority and underserved US populations. 2) Describe the most common MS symptoms exhibited by underserved US populations and compare/contrast them to majority populations. 3) Discuss the health inequities that exist for underserved adults with MS and how that impacts physical therapy practice.
Barriers for Minority Patients with Chronic
Diseases 14
• Limited insurance
• Low income
• Lower education levels, computer literacy skills, employment
• Language barriers
• Access to specialized MS clinics
• Care from a neurologist
• Lower quality mental health care, increased rates of depression
• Cultural barriers (Hispanics and AA)
• Living rurally
SJM2018CSMDoes Activity Level Play a Role in Prevalence?
• A 2016 survey of people with MS published in Archives of Physical Medicine
and Rehabilitation15 found that, on, average, African-Americans exercise less
than people of northern European ancestry. And exercise has been shown
repeatedly to have positive effects on physical mobility, cognition and mood.
While the reasons for African-Americans’ lower exercise rates aren’t clear,
researchers hope to drill deeper into this issue and address it with new
strategies.
• http://www.momentummagazineonline.com/a-fresh-perspective/
SJM2018CSMDoes Lifestyle Play a Role in Prevalence?
• Lifestyle-linked health conditions like obesity, diabetes, high blood
pressure, high cholesterol and heart disease impact MS14
• Addressing these problems can slow disease progression
• 69 % of black men and 82 % of black women are overweight or
obese16
SJM2018CSMImpact on Physical Therapy
• All evidence indicates that the earlier individuals begin treatment, the
more promising their long-term health outcomes
• Many groups are outside of access to health care14
• African-Americans in SNF did not receive more medications than
white adults with MS despite more physical & cognitive disability15
• Lack of financial resources can limit needed equipment
• Need osteoporosis screening and fall prevention
• Stress physical activity!!!!
SJM2018CSMClinical Options for Addressing Unmet Needs
and Health Disparities
• Recruit African-Americans for studies…include “African-American” in
names, designs, events
• Recruit religious leaders to conduct self-help groups; AA are more
spiritual than whites
• “Walking with Faith”
• MSFit: “Participants looked like me”
• MS Society’s Eastern North Carolina Chapter.
Annual conference just for AA started in 2002
SJM2018CSMPractice Insights
• Promote patient education, medication adherence, symptoms
management, and healthy lifestyle (regardless of race)
• Education is a key
• Develop clinical practice guidelines for minority groups
• Promote Nurse Navigators and MS Navigators
• Refer to a neurologist
• Work with the African American Advisory Council within the NMSS
• Screen for osteoporosis and fall risk
SJM2018CSMMS Navigators
• Service of the National MS Society
• Professionals skilled in finding information/resources for people with MS
• Connect with others living with MS
• Assistance with financial issues
• Deal with a crisis, maintain independence
• Access educational programs
• Phone: 1-800-344-4867 (business hours M-F)
• Email: contactusnmss@nmss.org
• Facebook: facebook.com/NavigatorMS
SJM2018CSMAdditional Resources
• National African American Advisory Council
Advises on the best approaches to reaching and engaging the African American
community: nationalMSsociety.org/AfricanAmericansandMS
• Dr. Hodges, an associate professor at the University of North Carolina at Chapel
Hill School of Social Work who lives with multiple sclerosis.
• Under her volunteer leadership, the Chapter’s African-American Conference was
created, the first such program for the Society nationwide. The conference
continues to be an effective outreach to African-Americans with MS.
SJM2018CSMSpecialty Clinics & Pro Bono Clinics
• Wayne State’s MS clinic treats more than 5,000 patients annually and
is the largest center in the world for African-Americans (700 patients)
• https://mscenter.med.wayne.edu/resources
• Pro bono clinics associated with DPT programs
• MSFit
SJM2018CSM• Community partnership that grew from a need for resources for
exercise for adults with MS in the NC Triad area (about 500,000 in
population)
• Partners: WSSU alumni whose mom has MS, WSSU DPT program,
Gateway YWCA
• Alumni created a board of directors comprised of a local neurologist
who leads the local MS specialty clinic, 2 WSSU faculty members,
NMSociety rep, YWCA rep)
• Created a Foundation called MSFit Foundation
SJM2018CSMDevelopment
• Board and foundation created
• Clinic location in underserved community, free of charge
• YWCA membership discounted for MSFit participants
• Foundation pays for memberships
• WSSU DPT students provide services under faculty supervision
• WSSU DPT students also organize a yearly fundraiser with proceeds
supporting MSFit Foundation
• Clinic hours for students are built into a class schedule
SJM2018CSM= Service Learning
• Students work in pairs for fitness/wellness screenings for this mobile
clinic
• Reflection assignment for the first experience at MSFit
• Documentation assignments
• Additional volunteer opportunities outside of class time
• Newest addition is a MTYoga class (medical therapeutic yoga)
SJM2018CSMTake Home Messages: Section One
• AA have a higher incidence/prevalence of MS
• AA and Hispanics with MS may have a higher level of disability
• AA with MS may have more barriers to optimal healthcare: Try….
• Earlier interventions
• Education
• MS Navigators
• Community support groups
• Pro bono clinics that promote lifestyle changes, exercise
SJM2018CSMReferences Section One
1. Lubin FD, et al. Defining the clinical course of multiple sclerosis. Neurology. 2014, 83:278-286.
2. Cohen ET, Csiza L, Karpatkin HI. PTNow Multiple Sclerosis Clinical Summary. 2016. APTA. Available at http://www.ptnow.org.clinical-summaries-detail/multiple-
sclerosis-ms.
3. https://www.nationalmssociety.org/About-the-Society/MS-Prevalence
4. www.nationalmssociety.org/InsideMS. The African-American Experience of MS. October-November 2006.
5. Langer-Gould A, Brara SM, Beaber BE, Zhang JL. Incidence of multiple sclerosis in multiple racial and ethnic groups. Neurology, 2013; 80(19): 1734-1739
6. http://www.progressivemsalliance.org/progressive-ms/facts-and-figures/
7. Wallin MT, Culpepper WJ, Coffman P, Pulaski S, Maloni H, Mahan CM, Haselkorn JK, Kurtzke JF; Veterans Affairs Multiple Sclerosis Centers of Excellence Epidemiology Group.
The Gulf War era multiple sclerosis cohort: age and incidence rates by race, sex and service. Brain. 2012 Jun;135(Pt 6):1778-85.
8. Khan O, Williams MJ, Amezcua L, Javed A, Larsen K, Smrtka JM. Multiple sclerosis in US minority populations. Neurol Clin Pract. 2015; April. 132-142.
9. Rivas-Rodriguez E, Amezcua L. Ethnic considerations and multiple sclerosis disease: variability in the United States. Neurol Clin, 2018. 36:151-162.
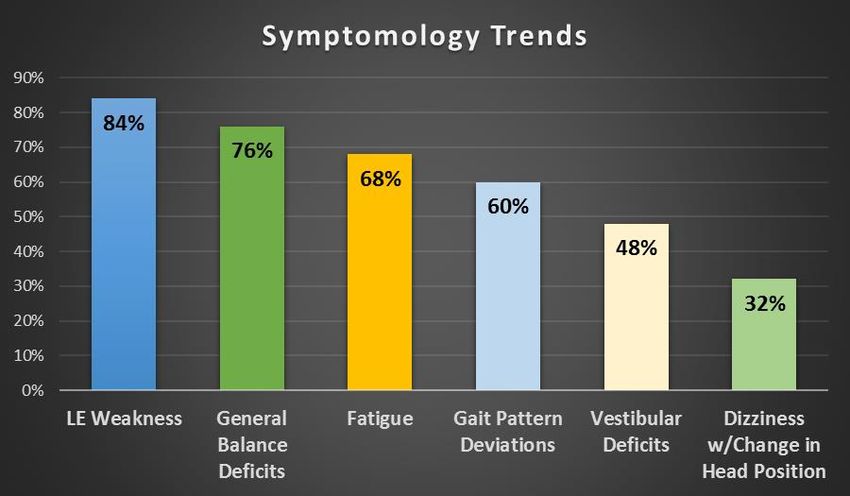
10. Migliarese S, Molina-Henry D, Nichols G, Duncan J. Symptomology in adults with multiple sclerosis in a community-based free clinic. Poster presentation at APTA
CSM, San Antonio, TX. Feb. 15, 2017.
10. Gibson JC, Summers GD. Bone health in multiple sclerosis. Osteoporos Int. 2011; 22:2935-2949.
11. Kelleher KJ, Spence W, Solomondis S, Apatsidis D. The characterization of gait patterns of people with multiple sclerosis. Disabil Rehabil, 2010; 32(15):1242-1250.
12. Motl RW, Goldman MD, Benedict RHB. Walking impairment in patients with multiple sclerosis: exercise training as a treatment option. Neuropsychiatr Dis
Treat.2010; 6, 767-774.
13. Rosenblum U, Melzer I. Reliability and concurrent validity of the narrow path walking test in person with multiple sclerosis. JNPT. 2017;41(1):43-51.
14. Goodman N, Morris M, Boston K Financial inequality: Disability, race and poverty in America. National Disability Institute;
http://nasuad.org/sites/nasuad/files/Disability-Race-Poverty-in-America.pdf, Accessed December 7, 2017.
15. Buchanan RJ, Martin RA, Wang S, Kim M. Racial analysis of longer-stay nursing home residents with multiple sclerosis. Ethnicity and Disease. 20016; 16:159-165.
16. http://www.momentummagazineonline.com/a-fresh-perspective/
17. https://stateofobesity.org/disparities/blacks/; Special Report Racial and Ethnic Disparities in Obesity; Accessed December 7, 2019
SJM2018CSMPathogenesis, pharmacology and genetic variation Doris Molina-Henry, PhD Assistant Professor Winston Salem State University
Pathogenesis, Pharmacology and
Genetic Variation
• 1) Overview of pathophysiology and current pharmacological agents
in the management of MS.
• 2) Describe potential pathophysiological explanations for the
variations in MS symptoms observed between underserved US
populations when compared to the majority of the population.
• 3) Discuss the variations in response to key pharmacological agents
and health inequities that relate to pharmacological therapies
experienced by underserved populations.Pathogenesis Multiple Sclerosis • Inflammatory demyelinating disease of the CNS. • Associated with autoimmunity, specifically immune-mediated myelin destruction. • Pathogenesis controversial: autoimmune disease or autoimmune reaction?1 • Lymphocyte responses against myelin antigens lead to focal demyelination, axon loss, and gliosis all which underlie lesion formation.2
Pathogenesis of multiple sclerosis • Dysregulation of both innate and adaptive immunity • Multiple immune cells involved • Immune dysregulation triggers aberrant lymphocytic responses.3,4 • Myelin-reactive CD4+ T cells play a central role • Inflammation tied to demyelination and neurodegeneration especially in acute and relapsing MS.4
Pharmacology • No pharmacological treatment is effective in arresting the neuro- axonal damage or restoring myelin. • Therapies enhance patient quality of life, reduce inflammation, reduce frequency and severity of acute attacks, delay disease progression. • Pharmacological targets: • Inflammatory response - corticosteroids • Immune response – Disease Modifying Drugs (DMDs) • Symptom management
Corticosteroids5
• Act on intracellular signaling pathways to modify inflammatory gene
transcription.
• Only short-term use recommended
• Prednisone (Deltasone, Cordrol)
• Prednisolone (Orapred)
• Methylprednisolone (Solu-Medrol)
• Bethamethasone (Celestone)
• Dexamethasone (Decadron)Corticosteroids5 • Inhibit enzymatic breakdown of the blood-brain barrier • Inhibit leukocyte response to antigens • Prevent migration of certain leukocytes in CNS • Suppression of proliferation and function of certain T-lymphocytes • Inhibit pro-inflammatory cytokines • Promote expression of anti-inflammatory cytokine TGF-beta • Manage acute episodes of MS or exacerbations. • Shorten length of attack and rapidly reduce inflammation. • Do not decrease the risk of future relapses, progression or disability.
Disease Modifying Drugs
• Introduced in the 1990
• Beta-interferon (beta-IFN) was the first FDA approved treatment, 1993
• Slow down the progression, decrease frequency and severity of acute attacks,
delay progression of disability and cognitive decline related to MS6
• Most effective if started early in the course of the disease
• Early DMDs were injectable or infusedParenterally Administered DMDs • Beta interferons (beta-IFNs) • 1a: Avonex, Rebif • 1b: Betaseron and Extavia • Glatiramer acetate (GA, Copaxone)7 • Mild side effect profile and efficacious
Parenterally Administered DMDs
• Monoclonal antibodies – highly efficacious but may have severe
potential complications7,8.
• Natalizumab (Tysabri), Daclizumab (Zenapax), Alemtuzumab (Campath-1H)
and Rituximab (Rituxan)
• Alemtuzumab (Lemtrada)7
• Antibody against CD52 antigen found in surface of numerous immune cells
• Relapsing for of MS, used when other medications are ineffective
• Reduces relapses and progression of disability
• Chemotherapeutic agents7,8
• Mitoxantrone (Novantrone)Oral DMDs 2010 and on…
• Fingolimod (Gilenya)7,8
• First oral medication approved for RRMS
• Reduction of lymphocytes and potential migration
• Decreased frequency of acute attacks and delays accumulation of physical
disability
• Dalfampridine (Amypra)7
• improves walking speed
• K+ channel blockerOral DMDs 2010 and on…
• Dimethyl fumarate (Tecfidera)7
• Neuroprotective and anti-inflammatory properties
• Decreased relapse rate
• Peginterferon beta-1a (Plegridy)7
• Longer lasting that other interferon formulations
• Decrease inflammation and neuroprotection, reduces disability progression
and brain lesions
• Teriflunomide (Aubagio)7,8
• Immunomodulator – may reduce over-activation of immune cells
• Decreased relapse rateMost recent intervention
• FDA approved first drug for Primary Progressive MS on March 28th,
20179
• Ocrevus (ocrelizumab) intravenous infusion
• Treats relapsing and primary progressive MS (PPMS)
• Thought to be more effective than Rebif (interferon beta-1a)
• Reduced relapse rates
• Reduced worsening of disability
• Common adverse reaction observed in clinical trials: upper respiratory tract
infectionGenetic underpinnings of MS • MS-prone genotype results from multiple independent or interacting polymorphic genes. • Interaction of these genes exerts a small or moderate effect to the MS overall risk.10 • Genes encoding antigen presenting molecules within the major histocompatibility (MHC) region account for the largest component of genetic risk for MS.11 • Human leukocyte antigen (HLA) immune response locus on the MHC.
Genetic underpinnings of MS • Association of HLA locus with MS risk has been observed across all populations studied. • HLA-DRB1 gene, more specifically DRB1*15:01 risk allele - documented as having the strongest association with MS risk.12 • Explains up to 10.5% of genetic variance underlying risk.13
Genetic underpinnings of MS • DRB1*15:01 has been associated with disease severity.14,15 • MS in AA showed risk to be firmly attributed to DRB1*15:01 or *15:03.16 • Immunochip study of MS risk in AA demonstrate substantial overlap between AA and European MS variants.17 • 7 single-nucleotide polymorphisms in 5 genes of interest were found significantly associated with MS in AA 18 • Sample size and instruments are limitations.
Pharmacogenetics of MS • Clinical response to DMDs is variable across individual patients. • Genes play modulatory response on DMT response, carriers of certain gene variant combinations may benefit from one therapy over another.19 • Wave of the future – personalized pharmacotherapy. • Limited data on AA and other underserved populations
Ethnicity and clinical response to
treatment
• AA and Hispanics may be less responsive to interferons
• Interferon beta-1a thought to be less effective in AA than WA based on
experience of more exacerbations and number of MS lesions following
24-48 weeks of beta-IFN 1a treatment.20
• Caveat: small population size
• AA and Hispanics MS patients respond better to Natalizumab therapy.
• Post-hoc analysis demonstrated that Natalizumab therapy improved the
relapse rate and accumulation of brain lesions in patients of African
descent with relapsing MS.References Section 2 • 1. Stys PK. Multiple sclerosis: autoimmune disease or autoimmune reaction? Can J Neurosci 2010 Sep;37 Suppl 2:S16-23 • 2. Wekerle H. Lessons from multiple sclerosis: models, concepts, observations. Ann Rheum Dis 2008 Dec; 67 Suppl 3:iii56-60 • 3. Miljkovic D, Spasojevic I. Multiple sclerosis: molecular mechanisms and therapeutic opportunities. Antioxidants Redox Signal 2013; 19:2286–2334. • 4. Yadav SK, Mindur JE, Ito K, Dhib-Jalbut S. Advances in the immunopathogenesis of multiple sclerosis. Curr Opin Neurol. 2015 Jun;28(3):206-19. • 5. Oger, J. (2007) Multiple Sclerosis for the Practicing Neurologist. New York, NY: Demos Health; 5: 59-64. • 6. Cross A.H. and Nainsmith R.T (2014) Established and novel disease-modifying treatments in multiple sclerosis. J Internal Med 275: 350-363 • 7. Ogbru O. (2015), Drugs used for Treating Multiple Sclerosis. Retrieved from: https://www.rxlist.com/script/main/art.asp?articlekey=99954 • 8. Loma L and Heyman R. Multiple Sclerosis: Pathogenesis and Treatment. 2011 Sep9(3): 409-416 • 9. FDA approves new drug to treat multiple sclerosis. (2017, March 29). Retrieved from: https://www.fda.gov/newsevents/newsroom/pressannouncements/ucm549325.htm • 10. Hollenbach J.A. and Oksenberg J.R. (2015) The immunogenetics of multiple sclerosis: A comprehensive review. J. Autoimmun. 64:12-25
References Section 2 • 11. Consortium TIMSGCtWTCC. A high-density screen for linkage in multiple sclerosis. Am. J. Hum. Gen.. 2005;476:214–219 • 12. Ramagopalan SV, Knight JC, Ebers GC (2009) Multiple sclerosis and the major histocompatibility complex. Curr Opin Neurol 22: 219–225. • 13. Consortium TIMSGCtWTCC. Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature. 2011;476:214–219 • 14. Hensiek AE, Sawcer SJ, Feakes R, Deans J, Mander A, Akesson E, et al. HLA-DR 15 is associated with female sex and younger age at diagnosis in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2002;72:184–187 • 15. Celius EG, Harbo HF, Egeland T, Vartdal F, Vandivik B, Spurkland A. Sex and age at diagnosis are correlated with the HLA-DR2, DQ6 haplotype in multiple sclerosis. J Neurol Sci. 2000;178:132–135. • 16. Oksenberg JR, Barcellos LF, Cree BA, Baranzini SE, Bugawan TL, Khan O, et al. Mapping multiple sclerosis susceptibility to the HLA-DR locus in African Americans. Am J Hum Genet. 2004;74:160–167. • 17. Consortium TIMSGCtWTCC. An ImmunoChip study of multiple sclerosis risk in African Americans. 2015;138 (Pt 6):1518-30. • 18. Johnson BA, Wang J, Taylor EM, et al. Multiple sclerosis susceptibility alleles in African Americans. Genes Immu 2010; 1(4):343- 33 • 19. Tsareva E., Kulakova O., Boyko A., Favorova O. Pharmacogenetics of MS: personalized therapy with immumomodulatory drugs. Pharmacogenet. Genomics 2016 (3): 103-15. • 20. Cree BAC, Al-Sabbagh A, Bennet R. Response to Interferon Beta-1a Treatment in African American Multiple Sclerosis Patients. Arch Neurol. 2005;62(11):1681-1683.
Status of the Evidence for Mobility Rehabilitation in MS Prue Plummer, PT, PhD Associate Professor University of North Carolina at Chapel Hill
Session Objectives 1. Critically appraise the current evidence for various rehabilitation approaches to improve mobility in people with MS (PwMS) 2. Discuss current evidence limitations and knowledge gaps regarding mobility rehabilitation in MS 3. Describe the steps needed for best practice implementation and considerations for building the evidence base to guide physical therapy practice in MS
Importance of mobility in PwMS • Reduced ambulatory activity is associated with greater disability and lower quality of life1 • Slower walking speed2 and use of an assistive device2,3 are associated with falls in PwMS • Mobility impairment is one the most common features of MS • Often used to track disease progression
What is a “therapeutic benefit” in mobility in PwMS? • 20% improvement in Timed 25-Foot Walk Test4 • MCID for comfortable gait speed: • 0.14 m/s5 (PwMS) • 0.10-0.17 m/s6 (systematic review of mixed adult pathology, including MS) • MCID for 6 min walk test: • Not established in MS • MDC = 82 m (269 ft) in PD • MDC95 for 2 min walk test: 19.2 m (63 ft)
In people with MS, does “physical therapy” improve mobility? Systematic review evidence: • Home or outpatient PT (1x/wk, 8 weeks) is “probably effective” for improving balance and gait in PwMS who can walk 5m7 • “Exercise training” may improve walking endurance and gait speed,8,9 but not T25FW or TUG9 • “Exercise therapy” may improve DGI scores10 • “Exercise training” improves mobility by ⅟5th SD11 • “Exercise training” improves mobility-related activities12
In people with MS, does “strength training” improve mobility? Systematic review evidence: • “Progressive resistance training”13 • Strong evidence PRT improves muscle strength • Inconsistent effects on functional mobility (endurance, gait speed, TUG) • “Strength training”14 • Improves muscle strength • No significant improvements in functional mobility (endurance, gait speed)
In people with MS,
does “FES” improve mobility?
Meta-analysis (low quality studies):15
In PwMS with foot drop, FES has an immediate and ongoing orthotic effect,
but no therapeutic effect:
• Improved gait speed by 0.05 m/s (immediate orthotic effect)
• Improved gait speed by 0.08 m/s (ongoing orthotic effect)
• No change in gait speed without the device over time (no therapeutic effect)In people with MS,
does “gait training” improve mobility?
Systematic review evidence:16
• Treadmill training, body-weight supported treadmill training, robot-
assisted treadmill training
• Improve gait speed and endurance
• Unclear if one method is superior to another
• Limited evidence available
Pooled data from 6 “gait training” RCTs:17
• Mean pre-post change in gait speed 0.06 m/s (95% CI: 0.02, 0.10)In people with MS,
does pharmacological treatment improve mobility?
Dalfampridine
Evidence from two Phase 3 clinical trials:18,19
• “Responders” improved 0.16 m/s (95% CI: 0.12, 0.19)
• “Non-responders” improved 0.05 m/s (95% CI: 0.03, 0.06)
• Placebo improved 0.03 m/s (95% CI: 0.01, 0.05)
• Overall improvement in gait speed (pooled responders and non-
responders) 0.07 m/s (95% CI: 0.05, 0.08)17In people with MS, does “dual-task gait training” improve mobility? Evidence from one pilot RCT:20 • Dual-task training tends to increase dual-task gait speed more than single-task training • No between-group differences in single-task gait speed Currently very little evidence available in MS
In people with MS,
does “yoga” improve mobility?
Meta-analysis of RCTs:21
• No effect of yoga on mobility compared to usual care
SMD = -0.20 (95% CI: -0.69, 0.30)
• No effect of yoga on mobility compared to exercise
SMD = -0.11 (95% CI: -0.63, 0.41)In people with MS,
does “whole-body vibration” improve mobility?
Meta-analysis of RCTs:22,23
• No training effect on TUG versus control:
SMD = -0.07 (95% CI: -0.34, 0.20)22
WMD = 0.31 (95% CI: -0.91, 3.42)23
• No training effect on gait speed versus control:
SMD = 0.17 (95% CI: -0.22, 0.57)22
SMD = 0.42 (95% CI: -0.78, 1.62)23
• No training effect on endurance versus control:
SMD = 0.25 (95% CI: -0.06, 0.55)22In people with MS,
does “balanced-based torso weighting”
improve mobility?
Evidence from one small RCT:24
• BBTW may have immediate improvements in gait speed versus no-
weight condition
• 8.5% improvement in T25FW time in BBTW groupReferences (section 3)
1. Block VA, Pitsch E, Tahir P, et al. Remote Physical Activity Monitoring in Neurological Disease: A Systematic Review. PLoS One 2016;11:e0154335.
2. Gianni C, Prosperini L, Jonsdottir J, et al. A systematic review of factors associated with accidental falls in people with multiple sclerosis: a meta-
analytic approach. Clin Rehabil 2014;28:704-716.
3. Gunn HJ, Newell P, Haas B, et al. Identification of risk factors for falls in multiple sclerosis: a systematic review and meta-analysis. Phys Ther
2013;93:504-513.
4. Goodman AD, Brown TR, Cohen JA, et al. Dose comparison trial of sustained-release fampridine in multiple sclerosis. Neurology 2008;71:1134-1141.
5. Paltamaa J, Sarasoja T, Leskinen E, et al. Measuring deterioration in international classification of functioning domains of people with multiple
sclerosis who are ambulatory. Phys Ther 2008;88:176-190.
6. Bohannon RW, Glenney SS. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: a systematic
review. J Eval Clin Pract 2014;20:295-300.
7. Haselkorn JK, Hughes C, Rae-Grant A, et al. Summary of comprehensive systematic review: Rehabilitation in multiple sclerosis: Report of the
Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2015;85:1896-1903.
8. Latimer-Cheung AE, Pilutti LA, Hicks AL, et al. Effects of exercise training on fitness, mobility, fatigue, and health-related quality of life among adults
with multiple sclerosis: a systematic review to inform guideline development. Arch Phys Med Rehabil 2013;94:1800-1828.e1803.
9. Pearson M, Dieberg G, Smart N. Exercise as a therapy for improvement of walking ability in adults with multiple sclerosis: a meta-analysis. Arch Phys
Med Rehabil 2015;96:1339-1348.
10. Sa MJ. Exercise therapy and multiple sclerosis: a systematic review. J Neurol 2014;261:1651-1661.
11. Snook EM, Motl RW. Effect of exercise training on walking mobility in multiple sclerosis: a meta-analysis. Neurorehabil Neural Repair 2009;23:108-
116.
12. Rietberg MB, Brooks D, Uitdehaag BM, et al. Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev 2005:CD003980.13. Kjolhede T, Vissing K, Dalgas U. Multiple sclerosis and progressive resistance training: a systematic review. Mult Scler 2012;18:1215-1228.
14. Cruickshank TM, Reyes AR, Ziman MR. A systematic review and meta-analysis of strength training in individuals with multiple sclerosis or
Parkinson disease. Medicine (Baltimore) 2015;94:e411.
15. Miller L, McFadyen A, Lord AC, et al. Functional Electrical Stimulation for Foot Drop in Multiple Sclerosis: A Systematic Review and Meta-
Analysis of the Effect on Gait Speed. Arch Phys Med Rehabil 2017;98:1435-1452.
16. Swinnen E, Beckwee D, Pinte D, et al. Treadmill training in multiple sclerosis: can body weight support or robot assistance provide added
value? A systematic review. Mult Scler Int 2012;2012:240274.
17. Plummer P. Critical Appraisal of Evidence for Improving Gait Speed in People with Multiple Sclerosis: Dalfampridine Versus Gait Training.
Int J MS Care 2016;18:105-115.
18. Goodman AD, Brown TR, Edwards KR, et al. A phase 3 trial of extended release oral dalfampridine in multiple sclerosis. Ann Neurol
2010;68:494-502.
19. Goodman AD, Brown TR, Krupp LB, et al. Sustained-release oral fampridine in multiple sclerosis: a randomised, double-blind, controlled
trial. Lancet 2009;373:732-738.
20. Sosnoff JJ, Wajda DA, Sandroff B, et al. Dual task training in persons with multiple sclerosis: a feasibility randomized controlled trial. Clin
Rehabil 2017;31:1322-1331.
21. Cramer H, Lauche R, Azizi H, et al. Yoga for multiple sclerosis: a systematic review and meta-analysis. PLoS One 2014;9:e112414.
22. Kantele S, Karinkanta S, Sievanen H. Effects of long-term whole-body vibration training on mobility in patients with multiple sclerosis: A
meta-analysis of randomized controlled trials. J Neurol Sci 2015;358:31-37.
23. Kang H, Lu J, Xu G. The effects of whole body vibration on muscle strength and functional mobility in persons with multiple sclerosis: A
systematic review and meta-analysis. Mult Scler Relat Disord 2016;7:1-7.
24. Widener GL, Allen DD, Gibson-Horn C. Randomized clinical trial of balance-based torso weighting for improving upright mobility in people
with multiple sclerosis. Neurorehabil Neural Repair 2009;23:784-791.You can also read