NEXT GENERATION ROTAVIRUS VACCINES - WHO Product Development for Vaccines Advisory Committee 26-27 June 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NEXT GENERATION ROTAVIRUS VACCINES
WHO Product Development for Vaccines Advisory Committee
26-27 June 2018
Duncan Steele, Carl Kirkwood, Lyou-Fu Ma
Confidential and proprietary data
© 2014 Bill & Melinda Gates Foundation
CURRENT SCENARIO FOR ROTAVIRUS VACCINES
Robust pipeline of live, attenuated oral rotavirus vaccines
• WHO pre-qualified and globally introduced
• Nationally licensed and in use in country
• New vaccines in development
Global impact of rotavirus vaccines
• Global status of rotavirus vaccine introductions
• Global impact and vaccine effectiveness
Rationale for developing parenterally delivered, non-replicating rotavirus vaccines
• Modest efficacy and effectiveness of the current live, attenuated rotavirus vaccines => better efficacy
• Potential increased safety profile of non-replicating rotavirus vaccines
• Opportunity for combination vaccines with routine childhood vaccines
• Potential lower COGS
• Potential for alternative immunization schedules
CONFIDENTIAL © Bill & Melinda Gates Foundation | 2
Dormant WHO PQ
National
LIVE ATTENUATED, ORAL ROTAVIRUS VACCINES license
Discovery &
Phase 1 Phase 2 Phase 3 Market
preclinical
Vaccine pipeline is diverse including:
Rotarix
• Multiple live-attenuated oral vaccines GSK
Live-attenuated
oral (WHO PQ)
• Non-replicating candidates
RotaTeq
Merck
“Current” licensed generation vaccines:
ROTAVAC
• Three WHO PQed products Bharat Biotech
• National licenses, mainly in private
market Liquid BRV RotaSIIL
Liquid BRV
• These aim to match performance of Shantha Biotechnics Serum Institute Serum Institute
Rotarix/RotaTeq vaccines Liquid BRV Rotavin
• Offer domestic mfg. options, add to BUTANTAN Brazil Polyvac, Vietnam.
supplier base / sustain competition Lamb rotavirus
Live-attenuated, oral
Liquid presentation
Lanzhou Institute of
Bharat Biotech
Biological Products
Next generation parenteral vaccines Liquid BRV
• Aim to exceed / meet performance of WUHAN China
Rotarix/RotaTeq vaccines RV3-BB
• Offer potential additional safety DCVMs include: Biofarma, Indonesia
Bharat Serum
• Offer potential lower costs BioFarma Hilleman Heat stable pentavalent
• Offer potential combination Polyvac Wuhan
Hilleman
MSD, India
opportunities for increased coverage Shantha Butantan
Langzhou
© Bill & Melinda Gates Foundation | 3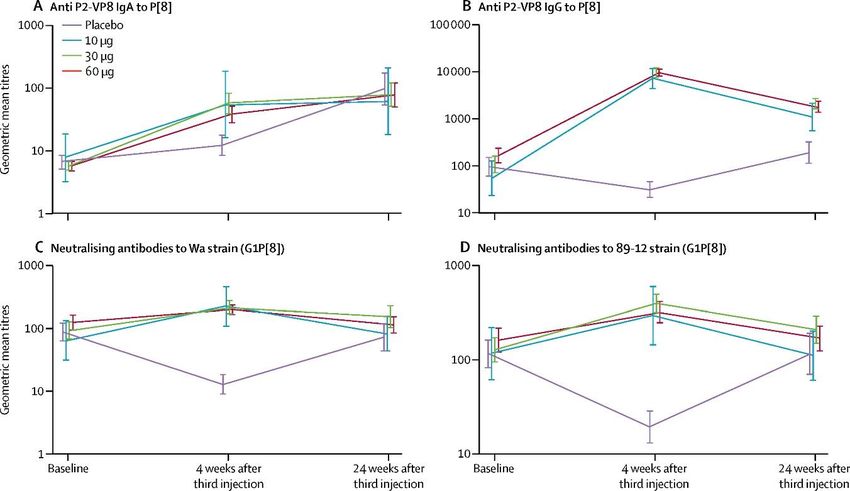
GLOBAL ROTAVIRUS VACCINE INTRODUCTIONS
92 countries have introduced by December 2017
New Gavi country introductions
2017: Lesotho, Cote D’Ivoire, Pakistan (phased national introduction
ongoing)
2018: Afghanistan, Uganda, DRC, Nepal, Benin, Bangladesh (Uttar
Pradesh will also introduce)
2019 (expected): Nigeria*, CAR, Myanmar, Lao PDR
Source: International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health. VIEW-hub Global
Vaccine Introduction and Implementation Report, June20, 2018 © Bill & Melinda Gates Foundation | 4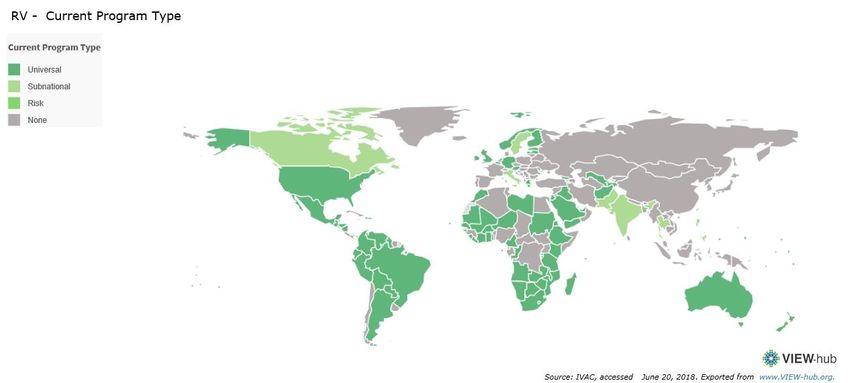
ROTAVIRUS VACCINE EFFICACY (PRE-LICENSURE) WAS SIMILAR IN
SIMILAR SETTINGS (i.e. HIGH AND LOW INCOME COUNTRIES)
Efficacy against severe rotavirus disease in first year of life
US/Finland/Other India
RotaTeq 98% (88.3,100) RotaSIIL 36% (11.7, 53.6)
India
ROTAVAC 56.3% (12.8, 73.3)
Niger
PK Kulkarni
George Armah Samba Sow RotaSIIL 66.7% (49.9, 77.9)
Southeast Asia
Nita Bhandari
RotaTeq 51.0% (12.8, 73.3)
Latin America/Finland
Rotarix 84.7% (71.7,92.4)
Southeast Asia (high)
Rotarix > 96%
Africa
Shabir Madhi Nigel Cunliffe RotaTeq 64.2% (40.2, 79.4)
Rotarix 61.7 % (44.0, 73.2)
Dang Duc Anh K Zaman
Sheila Isanaka
Vesikari T, Matson DO, Dennehy P et al. NEJM 2006; 354:23-33; Ruiz-Palacios GM, Perez-Schael I, et al. NEJM 2006; 354:11-22; Madhi SA, Cunliffe NA, Steele AD et al. NEJM 2010; 362:346-
357; Zaman K, Anh DD, Victor CV et al. Lancet 2010; 376:615-23; Armah GE, Sow S, Breiman RF et al. Lancet 2010; 376:606-614; Bhandari N, Rongsen-Chandola T, Bavdekar A, et al. Lancet
2014; 383:2136-43; Isanaka S, Ousmane G, Langendorf C, et al. NEJM 2017;376:1121-30; Kulkarni PS, Desai S, Tewari T, et al. Vaccine 2017; 35:6228-37 © Bill & Melinda Gates Foundation | 5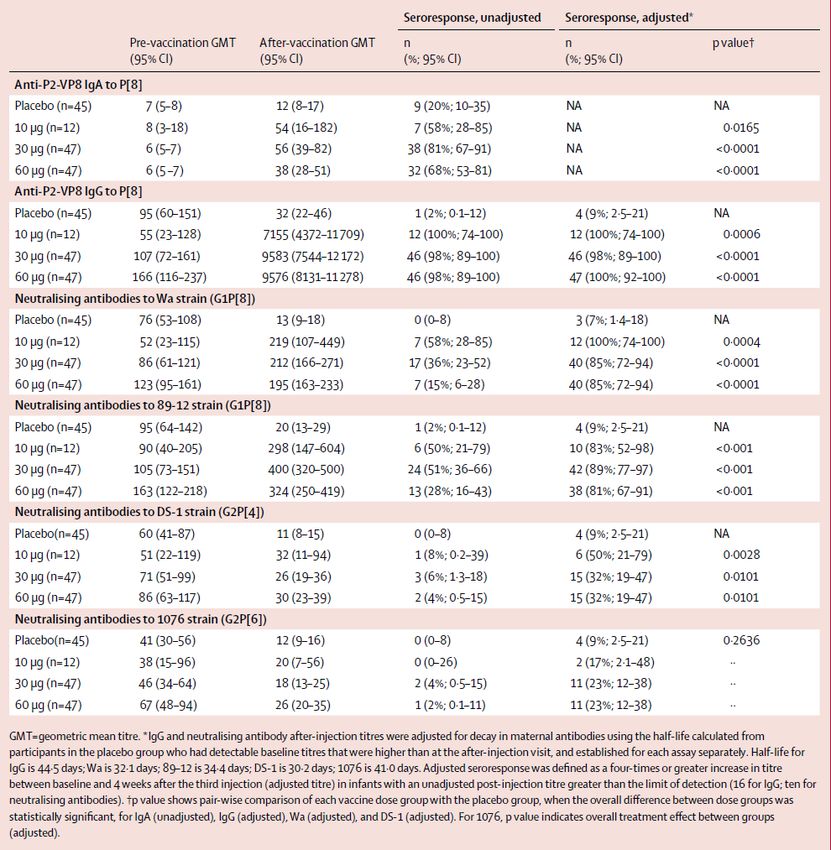
SUMMARY OF ROTAVIRUS VACCINE EFFECTIVENESS STUDIES 57 articles from 27 countries Among children
ROTAVIRUS DISEASE BURDEN AFTER ROTAVIRUS VACCINE INTRODUCTION
Attributable proportion of rotavirus severe diarrhea is still high, despite vaccine introduction and
uptake in African countries (provisional unpublished data)
Kenya (RVIDA, 1st year data) Tanzania
Source: Karen Kotloff, UMD and Eric Houpt and colleagues, UVA CONFIDENTIAL © Bill & Melinda Gates Foundation | 7
WHAT HAVE WE LEARNT ABOUT LIVE, ORAL ROTAVIRUS VACCINES?
• Despite enormous success of live attenuated, oral rotavirus vaccines several issues remain:
o A lower protective efficacy in the first 1-2 years of life (~50-60%) in developing countries in Asia
and Africa against moderate-to-severe rotavirus diarrhea
o Waning efficacy in the second year of life with little evidence of protection in the second year as
compared to the protection in "high-income“ countries (>95%)
o Limited indirect protection in impoverished, high risk settings
• Lower national coverage of rotavirus vaccine than DPT-3 / pentavalent vaccine rates in most
countries
• Vaccine costs are still relatively high.
• Despite an overall acceptable safety profile, intussusception rate seems to be slightly
increased by the live oral rotavirus vaccination (occurrence 1 to 3 /100 000 vaccine
recipients) in developed countries
Thus non-replicating, parenterally delivered rotavirus vaccines may provide viable alternative
CONFIDENTIAL © Bill & Melinda Gates Foundation | 8
CHALLENGES FOR ORAL ROTAVIRUS VACCINES
Multiple clinical immuno studies
• 2 v 3 doses of Rotatrix
• With/without breastfeeding
Factors that lower Factors that affect • Interference from maternal ab
virus titre antibody responses • Interval between doses
• Booster dose at 9 mo
• Transplacental maternal • Nutritional status
• Enteric pathogen interference
antibodies • Environmental enteropathy • Zn / probiotic co-administration
• Breast milk antibodies • Microbiota
• Stomach acid/proteases • Micronutrient deficiency Multiple host studies
• Co-administration of other • Early & constant exposure • Microbiome
vaccines to other gut pathogens • Blood group antigen /Lewis
• Other co-morbidities secretor status
• Environmental enteropathy
Glass RI, Jiang B, Parashar U. Vaccine 2018; 36:2233-36; Patel M, Shane AL, Parashar U et al, J Infect Dis 2009; 200:39-48 © Bill & Melinda Gates Foundation | 9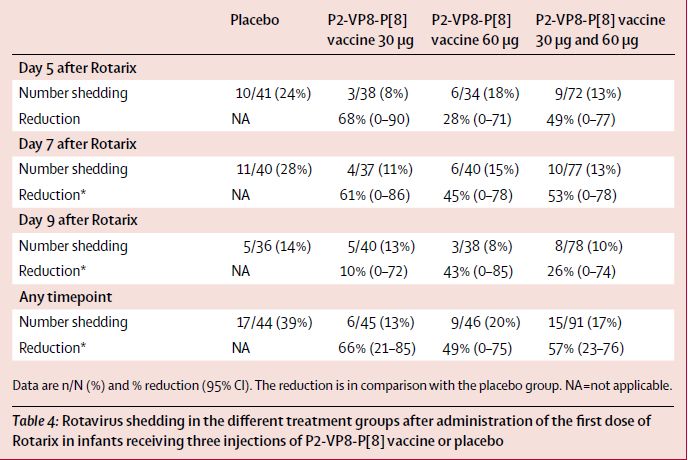
NON-REPLICATING, PARENTERAL ROTAVIRUS VACCINES
Pre-
Discovery Phase 1 Phase 2 Phase 3 Licensure
clinical
NRRV (P2-VP8*)
PATH
Inactivated
Rotavirus
CDC/SII
Non replicating
Expressed
VP6 protein
VLP Potential benefits include:
VP2/6;
VP2/6/7 • Lower COGs
• Higher efficacy profile
Combo-
VP6 with
• Decreased signal of intussusception
norovirus VLP • Potential for use in combination vaccine
• Potential for alternative dosing schedules
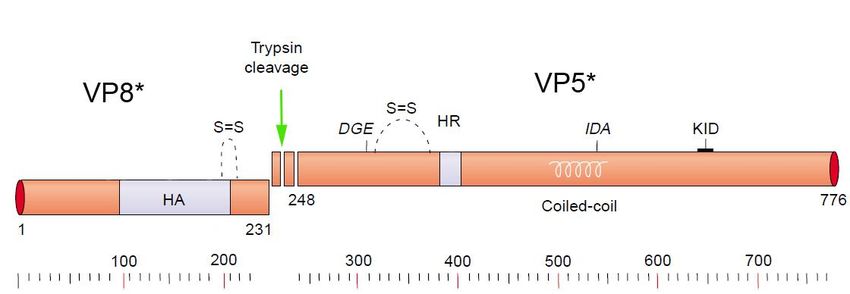
CONFIDENTIAL © Bill & Melinda Gates Foundation | 10NON-REPLICATING ROTAVIRUS VACCINE (NRRV – P2-VP8* TV)
VP4 hemagglutinin
• Developed by PATH, using NIH constructs. * VP7 outer capsid
• SK Vaccines, Korea - commercial partner
*
• Trivalent vaccine candidate based on:
• truncated VP8 subunits of P[4], P[6] and P[8]
genotypes (major circulating human rotavirus
genotypes)
• fused to tetanus toxin P2 CD4 epitope VP6 inner capsid
• expressed in E.coli (T7 promoter)
Hsc70 binding
site
• adsorbed to aluminum hydroxide
• parenteral IM administration route
Fusion domain
ΔVP8*
*
*
Wen X et al. Vaccine 2014; Wen X et al. HVI 2015 © Bill & Melinda Gates Foundation | 11CLINICAL DEVELOPMENT OF P2-VP8* MONOVALENT CANDIDATE
Phase 1 safety study in US adults Phase 2 age-descending, dose-escalating study of the
monovalent vaccine candidate (P2-VP8* P[8]) in toddlers
and infants in South Africa
Monovalent P2-VP8* P[8] was well
tolerated and immunogenic Serum antibody geometric mean titres (unadjusted)
• 4-fold rises of both IgA and IgG
responses observed
• Increasing GMTs with dose and titres
• Homologous N-Abs observed in ~50%
of subjects
• Responses to P[4] and P[6] had lower
GMTs
Fix A, Harro C, McNeal M et al. Vaccine 2015; 33:3766-72; Groome MJ, Koen A, Fix A et al, Lancet Infect Dis 2017; 17:843-53 © Bill & Melinda Gates Foundation | 12Serum antibody responses PHASE 2 SAFETY/IMMUNOGENICITY IN TODDLERS AND INFANTS Shedding of Rotarix after 3-dose P2-VP8* vaccine Groome MJ, Koen A, Fix A et al, Lancet Infect Dis 2017; 17:843-53 © Bill & Melinda Gates Foundation | 13
AGE-DESCENDING, DOSE-ESCALATING STUDY OF THE TRIVALENT P2-
VP8* VACCINE IN SOUTH AFRICAN INFANTS
• Phase 1/2 study in South Africa – initiated in March 2016
• Healthy adults, toddlers and infants
• Dose-escalation: 15 => 30 => 90 µg of total antigen
• Infants received 3 IM doses, one month apart, co-administered with EPI vaccines
• Enrolled in two stages, DSMB review before progression to Phase 2
• Enrollment closed in May 2017 – 558 infants enrolled
• Final visit for primary data (28 days after last study vaccination) – 18 August 2017
• All dose-levels in infants well tolerated and no safety signals observed
• Immunogenicity results showed robust immune responses (n=139/arm)
A priori “go” criteria were met and a decision to progress to Phase 2b/3 efficacy study,
with early futility read.
CONFIDENTIAL © Bill & Melinda Gates Foundation | 14TWO DATA SLIDES WITHHELD OF THE P2-VP8* TRIVALENT
CLINICAL TRIAL IN SOUTH AFRICA
CONFIDENTIAL Bill & Melinda Gates Foundation | 15INACTIVATED ROTAVIRUS VACCINE (IRV) WITH GROWTH AND
STABILITY
>99% TLP
G1P8 G2P4
~ 107 ffu/ml
~ 108 ffu/ml
G1P4
CDC-9 strain ● 107 ~ 108 titer in Vero cells
● Predominant (>90%) triple-layered
● Stable during USP & DSP
Jiang B et al, Vaccine 2008; Jiang B et al, HVI 2008 © Bill & Melinda Gates Foundation | 16IRV-CDC9 SHOWS IMMUNOGENICITY AND PROTECTION IN ANIMAL
MODELS
Induces cross-neutralizing-antibody to homotypic
IM route protects against oral challenge in
and heterotypic strains
10000 gnotobiotic piglets
pre dose 1
post dose 1
post dose 2
post dose 3
1000
Placebo IRV- CDC9
Antibodies (GMT)
100
10
Wa G1P[8] MW333 G8P[4] WI61 G9P[8]
Days of rotavirus shedding in stool after oral challenge (measured
by EIA)
Jiang B, Wang Y, Glass RI. Human Vac & Immunotherap 2013; 9:1634-37; Wang Y, Azevedo M, Saif LJ et al Vaccine 2010; 28:5432-36
Bill & Melinda Gates Foundation | 17
Wang Y, Vlasova A, Velasquez DE et al. PLoS One 2016; 11:e0166038ONE DATA SLIDE OF UNPUBLISHED RESULTS OF CO-
ADMINISTRATION OF IRV-CDC9 AND IPV IN RAT MODEL
© Bill & Melinda Gates Foundation | 18IRV-CDC9 DEVELOPMENT: PROGRESS TO DATE AT SERUM INSTITUTE
Procurement of strains and related regulatory work completed.
Preparation and characterization of seed viruses completed.
Production procedure (pilot scale) standardized.
Inactivation kinetic study on pilot scale (one liter) completed.
Immunogenicity & cross protective immunity in animals established.
Assays validated, stability (up to 9 months) and potency completed.
Future plans
• Large scale production development process optimization (one year).
• Animal Toxicity materials preparation (six months).
• First in human study should start by Mid 2019
• Combination vaccine R&D – proposed with IPV
CONFIDENTIAL Bill & Melinda Gates Foundation | 19APPROXIMATE DEVELOPMENT TIMELINES FOR LEAD CANDIDATES
2018 2019 2020 2021 2022 2023 2024 2025
cGMP Multinational P2b/3 Futility/Efficacy Trial with active comparator for
PATH/SK Chemicals
Local Registration WHO PQ
Stand Alone Manuf P3 prevention of severe RV gastroenteritis in healthy infants
Trivalent P2-VP8
MFDS
Vaccine
Value Proposition / Health
Economics of various options
Formulation Combination
Combination Vaccine Vaccine Formulation cGMP Manuf
Clinical immunogenicity
Feasibility bridging trial
NRRV+ Penta/Hexa Scale up
Immunization Schedule Clinical immunogenicity Trial- Prime (oral
RV vax) / Boost (trivalent P2-VP8)
Ph2: Immunogenicity Age
GLP Tox Adult Phase 1 Ph3 clinical efficacy
Traditional path Descending
IRV CDC9
CDC/SIIL
IND Local Registration
MFDS
cGMP Proc Validation/CGMP Manuf P3
Manuf Ph1
Ph2/3 Age De-escalation to
Ph3 booster extension study for efficacy
booster population
Licensure as a toddler booster
dose in ORV countries Proc Validation/cGMP Local Registration
Manuf for Ph3 TBD
Last updated: July 19, 2018 © Bill & Melinda Gates Foundation | 20HIGH-LEVEL VALUE PROPOSITION OF NEXT GENERATION ROTAVIRUS
VACCINES
Strategic goal: To develop a parenterally administered alternative to currently available live attenuated oral rotavirus
vaccines (LORVs) which is safe, provides increased relative efficacy and is more affordable to reduce the morbidity and
mortality associated with severe rotavirus gastroenteritis (SRVGE) in infants and toddlers residing in low resource settings
THAT WILL Increase relative vaccine efficacy over existing LORVs
(new benefits Provide a parenteral route of administration to circumvent the purported mechanisms resulting in
over existing suboptimal efficacy of LORVs in infants and toddlers in low resource settings
alternative)
Supply for public sector purchase at a lower price per dose and per regimen rotavirus vaccine than
currently available LORVs
Has the potential to be co-formulated with other parenterally delivered pediatric combination vaccines
to further reduce cost-of-goods sold (COGS), costs of vaccine delivery, and burden on the cold chain.
BECAUSE Immunization engenders antibody response that exerts protective effect at the gut level
(Reasons to Combining with EPI vaccines facilitates delivery and reduces associated costs
invest in
product) Enhanced efficacy and ease of administration, small footprint in cold chain, reduced vaccine wastage
Efficient, high throughput, low cost manufacturing platform. Greatly reduced supply constraints
Bill & Melinda Gates Foundation | 21Gavi prices:
Rotarix – $4.38/course
TARGET PRODUCT PROFILES - NEW ROTAVIRUS VACCINES RotaTeq - $9.60/course
RotaVac BRV-PV Lyo RV3-BB P2-VP8*-TV IRV
Characteristic (Bharat Biotech) (Serum Institute) (PT Biofarma) (PATH / SK Vaccines) (CDC / Serum Institute)
Indication Prevention of severe rotavirus gastroenteritis
Target Population Infants Infants Infants and Neonates Infants Infants
Route of Administration Oral Oral Oral IM IM
1 dose vial TBD
1 or 2 dose vial 1 dose vial
Presentation / Formulation 5 dose vials (0.5mL/d) Combo product with Combo product with
(2mL liquid) (2mL liquid)
penta or hexa IPV
3 doses 3 doses 3 doses
3 doses
Dosing Schedule (6, 10, 14wk DTP (6, 10, 14wk DTP (6, 10, 14wk DTP 3 doses
(6,10,14wk or 2,4,6mo)
schedule) schedule) schedule) (6, 10, 14wk DTP)
Duration of Protection 2 years 2 years 2 years 2 years 2 years
Vaccination Strategy Routine Routine Routine Routine + Penta Routine + IPV
Expected Efficacy 56% 36% - 67% 56 - 73% 75% (TBD) 75% (TBD)
Price per Dose $0.98 $1.70 (TBD) $1.17 (TBD) $0.85 (TBD) TBD
Licensure Date Q2 2014 Q4 2016 2020 2022 (TBD) 2024+ (TBD)
WHO PQ Date Q1 2018 Q4 2018 2022 2024 (TBD) 2025+ (TBD)
CONFIDENTIAL © Bill & Melinda Gates Foundation | 22NEXT GENERATION INTERVENTION TARGET PRODUCT PROFILE
Variable Minimum Optimistic
Indication* Prevention of severe rotavirus gastroenteritis in infants and toddlers Prevention of severe rotavirus gastroenteritis in infants and toddlers
Target Population* Individuals ~6 weeks to 2 years of age during primary EPI series (co- Neonates through children 2 years of age during primary EPI series (co-
administration) administration)
Target Countries GAVI-eligible and Lower-Middle Income Countries GAVI-eligible and Lower-Middle Income Countries
Efficacy* >75% >75%
Duration of Protection Through 2nd year of life Through 2nd year of life
Onset of Immunity 2 weeks after 3rd dose 2 weeks after 2nd dose
Indirect (Herd) Protection Yes Yes
Safety Clinically acceptable safety profile Clinically acceptable safety profile
Co-administration EPI series EPI series
Presentation Liquid formulated with Alum Liquid formulated with Alum
Vaccine in presentations from one to five 0.5-ml doses filled in a “2R” vial Vaccine in presentations from one to five 0.5-ml doses filled in a “2R” vial
conforming to ISO 8362 dimensions. Vial height 3.5 cm conforming to ISO 8362 dimensions. Vial height 3.1 cm or less, for reasons of
volume reduction and dimensional harmonization.
Route of Administration and Intramuscular Intramuscular
dosing frequency 3 doses at 3-8 week intervals, starting at 6 weeks of age 2 doses at 3-8 week intervals, starting at birth
Vaccine Volume (cm3 /dose) 0.5ml/dose 0.5 ml /dose
17cm3 17cm3
Stability / Shelf Life 2 years at 2-8C ;VVM-30 (30 days @40C, >3 years at 2-8C) VVM-30 (30 days @40C, >3 years at 2-8C)
Product Registration Path Marketing Authorization Application from NRA designated as functional by Marketing Authorization Application from NRA designated as functional by
WHO - Local license/WHO PQ WHO - Local license/WHO PQ
WHO Prequalification Date 2023 2022
Primary Target Delivery Channel GAVI and Lower-Middle Income Countries GAVI and Lower-Middle Income Countries
Clinical Endpoint for Licensure Efficacy Efficacy
© Bill & Melinda Gates Foundation | 23COMBINATION OPTIONS – PREFERENCE UNDER DIFFERENT CONDITIONS
(A GATES FOUNDATION PERSPECTIVE)
Conditions where this combination would be preferred
1 Heptavalent vaccine • Formulation for Heptavalent is feasible AND
(Penta+IPV+NexGenRV) • Price for Hepta is less than or equal to Hexa 1 plus NextGenRV
•
Formulation for Hepta is not feasible
2 Removal of IPV shot in combination with Penta makes space for
Hexavalent-1 (Penta+IPV) &
NextGenRV NextGenRV injection in the schedule, if efficacy can support
replacement of ORV
• Hexa1 exists but countries prefer to unbundle because Hexa1 price
3
is > Penta + 2 doses of IPV
Hexavalent-2
• OR Hexa1 supply insufficient to cover demand in the 2023-2027
(Penta+NextGenRV) & IPV
AND Hexa2 is ready in that time period
• OR After 2031, countries no longer want IPV
4 • Formulation and price are prohibitive in the options above
NextGenRV+IPV Combo & • 2 doses of NextGenRV provides sufficient protection
Pentavalent • OR an oral neonatal dose oral provides sufficient protection in
conjunction with the NextGenRV+IPV combo
Last updated: July 19, 2018 CONFIDENTIAL © Bill & Melinda Gates Foundation | 24DEVELOPMENT CONSIDERATIONS
Clinical development
• Choice of comparator for Phase 3 efficacy studies – no correlate of protection identified
• Innovative immunization schedules and strategies – prime boost options
Manufacturing and formulation development
• Selection of manufacturing partner (requires a compelling business case)
• Stand-alone or combination vaccine strategies
• RV + pentavalent vaccine or hexavalent vaccine
• RV + IPV
Policy and introduction
• Policy and regulatory pathways need to be examined and developed
• PPC and gPPP required
Full Public Health Value Proposition
CONFIDENTIAL © Bill & Melinda Gates Foundation | 25THANK YOU Last updated: July 19, 2018
SUBUNIT ROTAVIRUS VACCINE (VP6 INNER CAPSID PROTEIN)
Vaccine Developer(s) Development
Expressed Cincinnati Children’s VP6 expressed in E. coli as a fusion protein with maltose binding protein, and
rotavirus proteins Hospital Med Cent, USA administered with attenuated heat-labile toxin LT (adjuvant).
(based on
rotavirus VP6 inner Animal studies:
capsid) • Immunogenic (via CD4+ T cells)
• Protected in challenge studies in mice
Vaccine research Rotavirus VP6 - self-assemble into oligomeric structures (nanotubes, tubular
center/University of and spherical structures) or produced using a Baculovirus expression system
Tampere Finland
Animal studies:
• Immunogenic, induce strong humoral and T cell immunity generated CD4+
CTLs with the potential to lyse RV-infected target cells.
• Protective in small animal studies (predom. Homotypic)
Combined RV - norovirus vaccine candidate:
Murine challenge:
• showed protection against RV shedding observed regardless of delivery
route (intramuscularly, intranasally or a combination)
CONFIDENTIAL © Bill & Melinda Gates Foundation | 27SUBUNIT ROTAVIRUS VACCINE (VLP)
Vaccine Developer(s) Development
Virus like Mitsubishi Tanabe Pharma Rotavirus VP2, VP6, VP7 and NSP4 (from G1P[8] strains)
particle Co-op., Japan. Plant based production: VLPs are produced by transient expression in Nicotiana
approach benthamiana plants using Agrobacterium vectors transfected with the rotavirus
genes
Animal studies:
• induced the significant high level of anti-Wa IgG in dose dependent.
• homologous neutralizing antibodies was statistically higher than the placebo
group
Baylor College of Medicine, Various Constructs: VP2/VP4/VP6/VP7 VLP produced in baculovirus expression
USA system.
Animal studies - murine
• Highly Immunogenic
• Various delivery routes compared IM, IN and oral.
• Parenterally or intranasally gave highest mean protection from challenge
• Protective small animals (predominantly homotypic)
CONFIDENTIAL © Bill & Melinda Gates Foundation | 28You can also read