On the AMU Influenza (and pneumonia) - Dr Nick Scriven Acute Physician CHFT President Society for Acute Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Influenza ( ) and pneumonia
on the AMU
Dr Nick Scriven
Acute Physician CHFT
President Society for Acute Medicine
Influenza Influenza spreads around the world in yearly outbreaks 3-5million cases of severe illness Approx 250,000 - 500,000 deaths About 20% of unvaccinated children and 10% of unvaccinated adults are infected each year. In the northern and southern parts of the world, outbreaks occur mainly in the ‘winter’ Around the equator, outbreaks may occur at any time of the year. Death occurs mostly in the young, the old, and those with other health problems. Larger outbreaks known as pandemics are less frequent
What is flu?
Influenza viruses are RNA viruses that make up four of the seven genera of the
family Orthomyxoviridae
Influenza virus A
H1N1 - Spanish flu in 1918, Swine flu in 2009
H2N2 - Asian flu in 1957
H3N2 - Hong Kong Flu in 1968
H5N1 - Bird Flu in 2004
Influenza virus B – humans, seals and ferrets!
Influenza virus C - less common, humans, pigs, dogs
Influenza virus D – only isolated 2011, no humans yet
Pandemics
Name of pandemic Date Deaths Case fatality rate Subtype involved
possibly H3N8
Asiatic or Russian 1889–1890 1 million 0.15%
or H2N2
Flu
Spanish flu
1918–1920 20 to 100 million 2% H1N1
Asian Flu 1957–1958 1 to 1.5 million 0.13% H2N2
Hong Kong Flu 1968–1969 0.75 to 1 million
Virology
Structure Replication
Virion is 80–120 nm in diameter
Viral envelope containing 2 glycoproteins +
central core (viral RNA genome)
Influenza A genome - 11 genes on 8 pieces of
RNA, encoding11 proteins inc
haemagglutinin (HA), neuraminidase (NA),
Haemagglutinin (HA) and neuraminidase (NA)
are the two large glycoproteins on the outside
of the viral particles.
Influenza A viruses are classified into subtypes
based on antibody responses to HA and NA.
These different types of HA and NA form the
basis of the H and N distinctions in, for
example, H5N1.
There are 18 H and 11 N subtypes known, but
only H 1, 2 and 3, and N 1 and 2 are commonly
found in humans.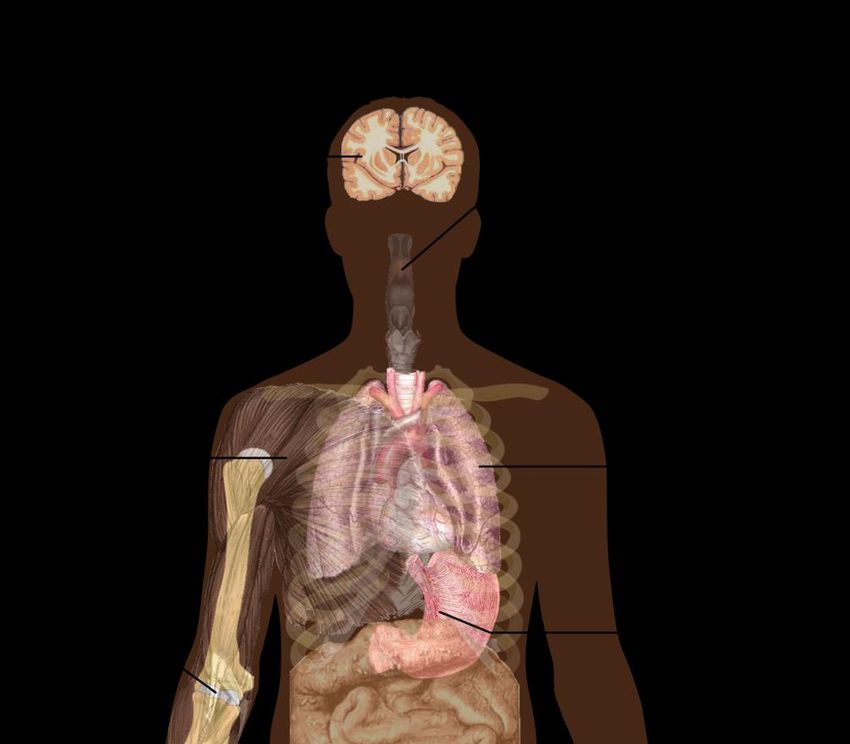
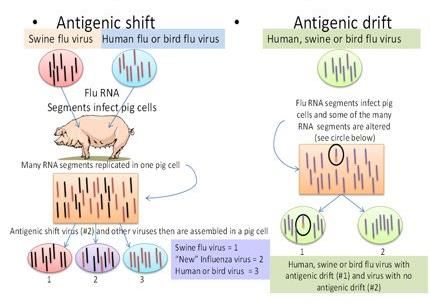
Drift and Shift
Drift
natural mutation over time
can cause loss of immunity or
vaccine inefficiency/mismatch
occurs in Flu A and B
Shift
two or more different strains of a virus
combine to form a new subtype having a
mixture of surface antigens
only Flu A
UK DATA 2018/19
Influenza Like Illness Rates

Hospital Data 2018/19
ICU DATA 3,245 ICU admissions (1015 A(H1N1), 242 A(H3N2), 1954 A(unknown), 34 B)) 317 deaths in UK this season 96 admissions to ECMO centres
Virology 2018/19
Influenza Transmission
Usually symptoms 1-4 days after Influenza can be spread in three
infection but some (? 30%) could be main ways
asymptomatic or mild illness only direct transmission (when an
Transmission can start 24hrs pre infected person sneezes mucus
symptoms directly into the eyes, nose or
mouth of another person)
Peaks around 48hr and usually
airborne (when someone inhales
stopped by Day 5 the aerosols produced by an
In elderly and infected person coughing, sneezing
immunocompromised can be or spitting)
transmittable for up to 9 days (30% hand-to-eye, hand-to-nose, or
of elderly secreting at 7 days in 1 hand-to-mouth - contaminated
study) surfaces or from direct personal
contact such as a handshake.
Antivirals reduce viral sheddingFlu Symptoms
Symptoms of influenza onset 24-48
hrs after infection
Usually the first symptoms are chills,
body aches, fever with body
temperatures ranging from 38-39°C
It can be difficult to distinguish
between the common cold and
influenza.
Symptom: sensitivity specificity
Diarrhoea is not usually a symptom of Fever 68–86% 25–73%
influenza in adults, although it has Cough 84–98% 7–29%
been seen in some human cases of
Nasal congestion 68–91% 19–41%
the H5N1 "bird flu“ and can be a
symptom in children All three findings, especially fever, were less sensitive
in people over 60 years of age.Treatment
Prevention – Vaccination
Cure or symptomatic?
Simple measure
Amantidine – resistance ~100% in A, no use in B
Neuraminidase inhibitors- Oseltamiver/ZanamivirUK Vaccinations 2018/19
3 vaccines used:
Adjuvanted trivalent flu vaccine (aTIV) - people aged >65
Quadrivalent vaccine (QIV) - children aged from 6 months to 2 years and in
adults ages 18 -65 who are at increased risk because of a long term health
condition.
Live attenuated influenza vaccine (LAIV) (nasal spray).The age groups
targeted in England for this vaccine in 2018/19 were 2-3year olds (through
their GP surgery) and school aged children in reception - Year 5 (schools).Vaccination data (May 2019)
Proportions of people in England who had received the 2018/19 influenza vaccine in targeted
groups
48.0% in under 65 years in a clinical risk group
45.2% in pregnant women
72.0% in 65+ year olds.
43.8% in 2 year olds and 45.9% in 3 year olds.
Influenza vaccine uptake by frontline healthcare workers show 70.3% were vaccinated by 28
February 2019,Vaccine Effectiveness (All FLU A)
For 6 months to end Jan 2019 from 6 European studies
In primary care settings among all ages, VE against confirmed influenza A
ranged - 32-43%
Patients aged 18–64 years ranged from 32% (EU-PC) to 55% (DK-PC).
In children aged 2–17 years in UK-PC, the VE of LAIV4 was 80%
Among target groups for influenza vaccination, VE was 59%
VE against laboratory-confirmed hospitalised influenza A among all ages was
38%Vaccine Effectiveness (A(H1N1))
In the primary care studies, VE against confirmed influenza A(H1N1)pdm09 -
all ages – 45 - 71%
In UK-PC, the VE of LAIV4 among children aged 2–17 years – 87%
In hospital-based studies among patients aged >65 years VE was 29-37%. VE
among those aged 18–64 years was 49%.
To date, all A(H1N1)pdm09 viruses characterised in Europe were
antigenically similar to the vaccine virusCochrane Review (2014) and NIHR (2016)
Oseltamivir and zanamivir have non-specific effects on reducing the time to
alleviation of influenza symptoms in adults (not in asthmatic children) —
oseltamivir reduced the time by 16.8 hours
Treatment of adults with oseltamivir had no significant effect on
hospitalisations.
Prophylaxis with either oseltamivir or zanamivir may reduce symptomatic
influenza in individuals and in households
Oseltamivir increases the risk of adverse effects, such as nausea, vomiting,
psychiatric effects and renal events in adults and children — oseltamivir in
the treatment of adults increased the risk of nausea (NNTH = 28 ) and
vomiting (NNTH = 22)Oseltamivir treatment for influenza in adults:
a meta-analysis of randomised controlled trials
Joanna Dobson, MSc, Prof Richard J Whitley, MD, Prof Stuart Pocock, PhD, Prof Arnold S Monto, MD
Lancet 2015
In the intention-to-treat infected population
21% shorter time to alleviation of all symptoms
The median times to alleviation were 97·5 h for oseltamivir and 122·7 h for placebo
Fewer lower respiratory tract complications requiring antibiotics >48h after randomisation
Fewer admittances to hospital for any cause
Oseltamivir increased the risk of nausea and vomiting
No recorded effect on neurological or psychiatric disorders or serious adverse events.Complicated influenza:
Influenza requiring hospital admission and/or with symptoms and signs of lrti, cns
involvement and/or a significant exacerbation of an underlying medical condition.
Risk factors for complicated influenza:
a. Neurological, hepatic, renal, pulmonary and chronic cardiac disease.
b. Diabetes mellitus
c. Severe immunosuppression.
d. Age over 65 years.
e. Pregnancy (including up to two weeks post partum).
f. Children under 6 months of age.
g. Morbid obesity (BMI ≥40).Severe immunosuppression:
a. Severe primary immunodeficiency.
b. Current (within six months) chemotherapy or radiotherapy
c. Solid organ transplant recipients on immunosuppressive therapy.
d. Bone marrow transplant recipients currently, or within 12 months of receiving
immunosuppression.
e. Patients with current graft-versus-host disease.
f. Patients currently receiving high dose systemic corticosteroids (equivalent to ≥40 mg
prednisolone per day for >1 week) and for at least three months after treatment has stopped.
g. HIV infected patients with severe immunosuppression (CD4Treatment Notes
At risk population - including pregnant women:
Oseltamivir (PO). Do not wait for laboratory confirmation. Treatment should be started as soon as possible, ideally
within 48 hours of onset.
Severely immunosuppressed patients:
Some influenza subtypes are associated with a greater risk of developing oseltamivir resistance, and the selection
of first line antivirals in severely immunosuppressed individuals should take account of the dominant circulating strain
of influenza.
Oseltamivir PO is the first line treatment, unless the dominant circulating strain is influenza A(H1N1), in which
case use zanamivir (INH).
Treatment should start as soon as possible
If clinical condition does not improve take a specimen for resistance testing and consider other possible causes.
When oseltamivir is indicated based on the above advice use 75mg PO twice daily for 10 days
Suspected or confirmed oseltamivir resistant influenza in a patient who requires treatment:
Zanamivir (INH). Treatment should be started as soon as possible
Management of patients for whom zanamivir is indicated, who are unable to self-administer inhaled zanamivir:
Patients who are severely immunosuppressed and cannot take inhaled zanamivir should receive oseltamivir PO.
Patients who have suspected or confirmed oseltamivir resistant infection and cannot take inhaled zanamivir should be
considered for nebulised aqueous zanamivir.Viral susceptibility to standard
treatment
990 influenza A(H1N1) viruses have been tested for oseltamivir susceptibility-
968 were fully susceptible and 22 were resistant
(all susceptible zanamivir)
238 and 223 influenza A(H3N2) viruses have been tested for oseltamivir and
zanamivir susceptibility - all were susceptible.
Three influenza B viruses have been tested for both oseltamivir and zanamivir
and all were susceptibleComplications of Influenza
Pulmonary
Extrapulmonary
Sam Ghebrehewet et al. BMJ 2016;355:bmj.i6258Pulmonary Complication
Primary influenza pneumonia
Secondary bacterial pneumonia – Strep , Staph, Haem
Superadded infection with unusual pathogens – Chlamydia, Legionella,
Aspergillus
Exacerbation underlying lung disease
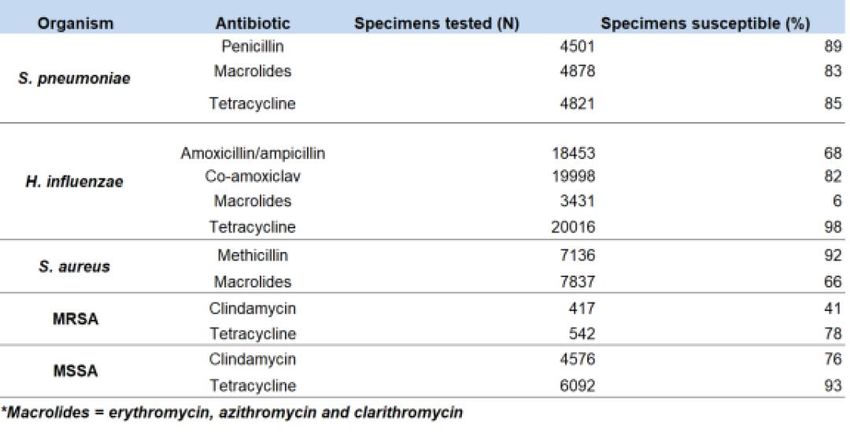
ARDSPneumonia drug susceptibility (2019)
Proportion of all lower respiratory tract isolates of Streptococcus pneumoniae, Haemophilus
influenza, Staphylococcus aureus, MRSA and MSSA tested and susceptible to antibiotics.Extrapulmonary complications
Pericarditis/myocarditis – 1 study 50% of hospitalised flu patients had abn ECG (2005
clin inf dis)
Myocardial infarction
Myositis
Encephalopathy (Reye’s Syn)
Encephalomyelitis/transverse myelitis
Aseptic meningitis
Guillain- Barre
Rhabdomyositis
AKI
Encephalitis lethargica (historical)Other ‘Bugs’ we worry about
Avian Influenza Middle East respiratory
(February - April 2019)
syndrome coronavirus (MERS-
CoV)
Influenza A(H5) viruses
Since September 2012 WHO has been notified
no new laboratory-confirmed human of 2,419 laboratory-confirmed cases of
cases of influenza A(H5) virus infections infection with MERS-CoV (836 deaths).
were reported to WHO.
In UK to May 2019, 5 cases of MERS-CoV, (3
Influenza A(H7N9) imported, 2 linked cases)
1 new laboratory-confirmed human case Since September 2012, 1,515 suspected cases
of influenza A(H7N9) virus infection in the UK that have tested negative.
were reported to WHO from China
From March - April 2019, Saudi Arabia
Influenza A(H9N2) reported 45 additional cases of MERS-CoV
infection (13 deaths). Of these 9 cases,
1 new laboratory-confirmed case of including 1 death, were linked to the
influenza A(H9N2) virus infection was outbreak in Wadi Aldwasir city.
reported to WHO from China. Avian
influenza A(H9N2) viruses are enzootic The latest ECDC MERS-CoV risk assessment
in poultry in China. highlighted that risk of widespread
transmission of MERS-CoV remains very low.And now the bad news……..
In conclusion
Have outlined
last year’s data
Current treatment guide
Virology/Vaccine
Some gloom and doom
Have not talked about CAP as there’s nothing new!You can also read