Onycholysis Dr Shyamalar Gunatheesan Skin Health Institute (Nail Clinic) 17/03/2021 - NET
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Onycholysis Dr Shyamalar Gunatheesan Skin Health Institute (Nail Clinic) 17/03/2021

Onycholysis • No conflict of interest

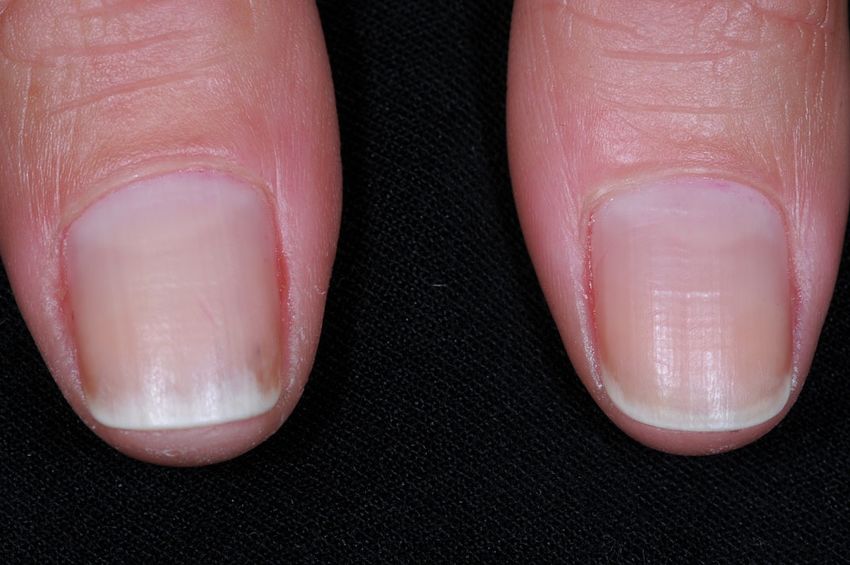
Onycholysis
• Detachment of the nail plate from the nail bed at the distal end and/or lateral
attachments
• Creates a subungual space that gathers keratin debris and dirt
• Water accumulates, secondary bacterial and yeast infection
• Not inflammatory unlike chronic paronychia
• White or yellow discolouration due to air under nail, sequestered debris, shed
squames and glycopyrotein exudate
• Pseudomonas causes green/black discolouration
Onycholysis • Idiopathic : • Psoriasis : Yellow , wavy margin between normal nail and separated area , glycoprotein deposition • Photo-onycholysis : sudden onset , due to drugs or chemical interaction with sun • ‘Sculptured onycholysis’, due to cleaning with sharp instrument • Hypothyroidism, hyperthyroidism, hyperhidrosis, impaired circulation

Idiopathic onycholysis • Painless separation of the nail from the bed • Overzealous manicure, frequent wetting, cosmetic solvents • Minor traumatic element- more common in abnormally long nails • Affected nails tend to grow very quickly • Starts at the tip and extends to involve the distal third of the nail bed • Microbial colonization with Candida albicans and other bacteria.

Idiopathic onycholysis • If the condition persists for several months, the nail bed becomes dark and irregularly thickened • Mostly seen in females • The longer it lasts, the less likely is the nail to become reattached due to keratinization of the exposed nail bed

Psoriasis • 50% of psoriatics have nail involvement • Nail pits • Onycholysis • Subungual hyperkeratosis • Nail plate discolouration • Splinter haemorrhages • Acute and chronic paronychia

Psoriasis- Onycholysis • Focal nail bed parakeratosis produces an oily spot or salmon patch • Extension of this area to the free edge produces onycholysis • Has a reddish brown margin • Or onycholysis may commence at the distal edge • Disruption of the onychocorneal band • Progressive

Onycholysis due to psoriasis
Psoriasis and onycholysis
Onycholysis with damage due to acrylates
Onycholysis with acute perniosis
Mrs MM 72 year-old, 12m green nails
Rx Itraconazole pulse X3, vinegar
Onycholysis : tips
• Lots of causes, patients usually have long nails, like to have manicures
• Secondary pseudomonas causes green or black discolouration
• Chronic candida infection may prolong course
• Can try oral anticandidal agent, eg itraconazole 400mg/day for 1 week a month
for 3 months
• Fluconazole 200mg 2X/weekOnycholysis: candida Rx Pre Rx Post itraconazole
Onycholysis, candida Pre Fluconazole Post Fluconazole
Onycholysis and pseudomonas
Onycholysis post Rx
Vinegar and itraconazolePre and Post Fluconazole
75 year-old man, longstanding nail problems, culture negative, hyphae
Post fluconazole 200mg 2/week 4 months
Pre and post fluconazole
Pre and Post Rx! Nails longer!
Fluconazole
• Demonstrates rapid uptake to the nail
• Detected at the distal end of the nail plate within 1 day of treatment
• With 150mg weekly for 12mths- detected in nail plate for at least 6mths after
discontinuation
• Inhibits cytochrome P-450 enzyme lanosterol 14@ demethylase with resultant
inhibition in the conversion of lanosterol to ergosterol.Fluconazole- Safety profile • Well tolerated • Nausea, vomiting, diarrhoea • Rash • Headache • Rare side effects- paraesthesia hands and feet, confusion, seizures, dizziness • Rare severe liver disease • Leukopenia, agranulocytosis, thrombocytopenia, increased cholesterol
Fluconazole • Ventricular dysfunction- congestive cardiac failure • Rare cases of prolongation of the QT interval • Caution with proarrhythmic conditions
Fluconazole-Drug Interactions
• Thiazides- reduces clearance of fluconazole
• Calcium channel blockers-watch for edema and hypotension
• Diabetic drugs- sulfonylureas- watch for hypoglycaemia
• Statins- atorvastatin, lovastatin, simvastatin- risk of myopathy and
rhambdomyolysis
• Anticoagulants- warfarin- haemorrhage
• NSAIDs- non selective and the COX-2 inhibitors
• Hormonal contraceptives- effect unpredictableWhat’s new with nail psoriasis Rx?
• Iontophoresis: small electrical charge to deliver medications through the skin
• Dexamethasone: 100ml distilled water, 3ml dexamethasone sodium (8mg in
2ml)
• Electrodes placed on the dorsum of the hands
• 4mA of current applied through the solution
• 20 mins
• Weekly for 4-6 monthsIONTOPHORESIS
Study of DI from 1996-2011
• 27 patients identified with adequate follow-up
• All patients had at least 3 months of weekly DI
• Some had other Rxs too eg creams
• Photos taken before, during after
• NAPSI scores done on photos
Dexamethasone iontophoresis for the treatment of nail psoriasis- Quynh Van
Le, Anne Howard Australas J Dermatol.2013NAPSI scoring
• The target nail is graded for features of nail matrix and nail bed psoriasis
• Nail matrix psoriasis- Pitting, leukonychia, red spots in the lunula, nail plate
crumbling
• Nail bed psoriasis- Onycholysis, splinter haemorrhage, oil drop sign, nail bed
hyperkeratosis
• Max score per quadrant is 2
• Max score per nail is 8Dexamethasone iontophoresis study
• Treatment was ceased when no more improvement was being gained, or if
patients developed side effects
• NAPSI scoring was done by one investigator, no blinding.DI : Results
• 18 female, 9 male, 30-83 years
• Number of nails involved ranged from 1-10 (mean 8)
• Number of treatments ranged from 9-102 (mean 42)
• 22 patients showed some improvement ie 81%DI : results
• 22 patients showed an improvement clinically and according to NAPSI scores
ie 81%
• 2 patients had no improvement according to NAPSI scores but improved said
their nails felt stronger!
• Range of NAPSI improvement was 1-25 (mean 8)DI : results
• 3 patients had DI alone
• Others had topical calcipotriol and steroids
• One had oral anti-candidal therapy
• 2 patients had relapses which responded to re- treatments
• 1 patient had 3 relapses over 12 years and was successfully re-treated each
timeDI results • 5 patients failed to improve after 12-40 treatments • 2 of those patients were still happy with treatment! • One patient reported painful fissuring of the fingertips: this resolved with time
Dexamethasone iontophoresis • Relatively easy to set up. • Relatively cheap • Very few side effects • Happy patients • Works best for distal nail disease ie onycholysis • Not set up for toenails!
Pre and post iontophoresis
Pre and post iontophoresis
Pre and post iontophoresis
Pre and post iontophoresis
Pre and post iontophoresis
Pre and post iontophoresis
?Iontophoresis for psoriasis, fluconazole for others, Mrs CG
Pre and post fluconazole
Toenails, trauma +/- fungal, psoriasis
Summary : Tips for Onycholysis
• Keep nails short, out of soaps and detergents
• Do not use sharp objects under nails
• Think of anti-yeast oral Rx , especially if there are hyphae
on microscopy
• Iontophoresis for nail psoriasisCONTACT Dr Shyamalar Gunatheesan Skin Health Institute (Nail Clinic) Speaker
You can also read