Antithrombotische Therapie bei ACS: Müssen wir etwas ändern? - Prof. Dr. med. Dirk Sibbing
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Antithrombotische Therapie bei ACS: Müssen
wir etwas ändern?
Prof. Dr. med. Dirk Sibbing
20. Oktober 2018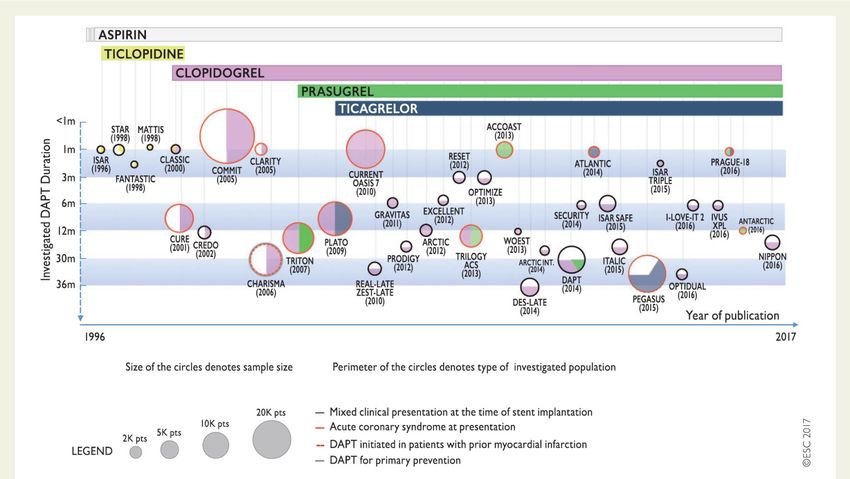
COI • Research grants: Roche Diagnostics, Daiichi Sankyo • Speaker fees / Advisory board activities: Sanofi, Bayer, Astra Zeneca, Pfizer, Daiichi Sankyo, Haemonetics, BMS

20 Jahre DAPT Studien
35 Studien
>225,000
Patienten
ESC DAPT Guidelines, Valgimigli et al., EHJ 2017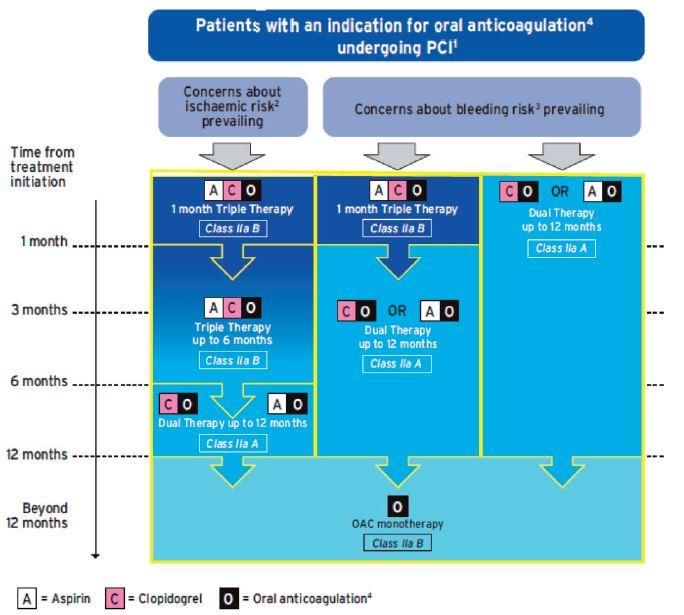
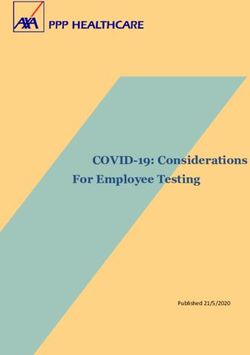
2018 ESC Guidelines:
Antithrombotika
Apixaban
Anticoagulant drug
Edoxaban Bivalirudin
Rivaroxaban Enoxaparin UFH Dabigatran
VKAs
Factor Xa
Fibrinogan
Tissu Factor Coagulation Prothrombin Thrombin
(Tissue lesion) cascade
Fibrin
Aspirin
Antiplatelet drug
TxA2
GPIIb/IIIa
DAPT activation
ADP
Clopidogrel GPIIb/IIIa Inhibitors
Prasugrel (Abciximab, Glycoprotein IIb/IIIa receptor
Ticagrelor Eptifibatide, Soluble mediators (ADP, TxA2)
Cangrelor Tirofiban) Clot-bound thrombin/FXa
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018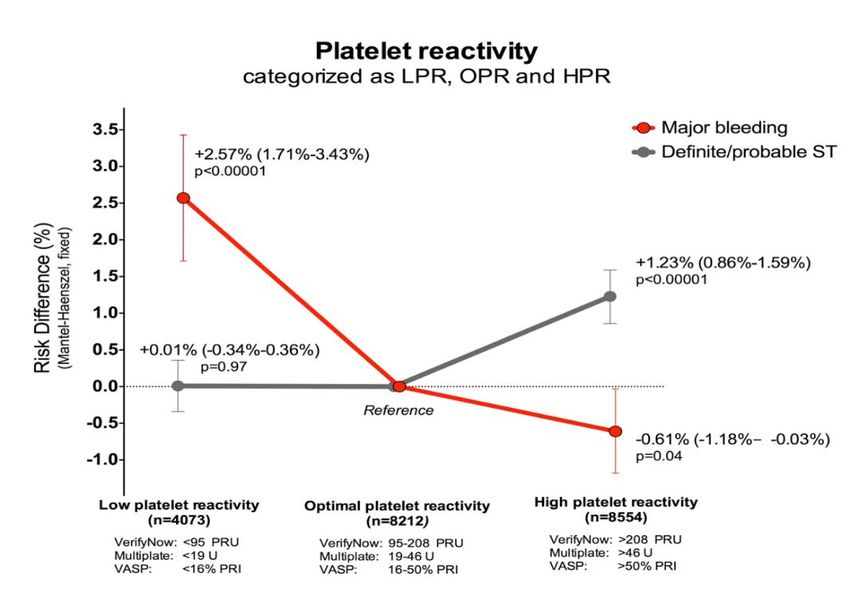
Agenda 1) Was sind die aktuellen Empfehlungen zur dualen Plättchenhemmung bei ACS Patienten ? 2) Strategien zur Individualisierung der Plättchenhemmung in 2018: Länger? Kürzer? De-Eskalation?
Agenda 1) Was sind die aktuellen Empfehlungen zur dualen Plättchenhemmung bei ACS Patienten ? 2) Strategien zur Individualisierung der Plättchenhemmung in 2018: Länger? Kürzer? De-Eskalation?
2018 ESC Guidelines
2018 ESC/EACTS Guidelines on
myocardial revascularization
The Task Force on myocardial revascularization of the European Society of Cardiology (ESC)
and European Association for Cardio-Thoracic Surgery (EACTS).
Developed with the special contribution of the European Association for Percutaneous
Cardiovascular Interventions (EAPCI).
Authors/Task Force Members: Franz-Josef Neumann (ESC Chairperson) (Germany),
Miguel Sousa-Uva (EACTS Chairperson) (Portugal), Anders Ahlsson (Sweden),
Fernando Alfonso (Spain), Adrian P. Banning (UK), Umberto Benedetto (UK),
Robert A. Byrne (Germany), Jean-Philippe Collet (France), Volkmar Falk (Germany),
Stuart J. Head (The Netherlands), Peter Jüni (Canada), Adnan Kastrati (Germany),
Akos Koller (Hungary), Steen D. Kristensen (Denmark), Josef Niebauer (Austria),
Dimitrios J. Richter (Greece), Petar M. Seferovic (Serbia), Dirk Sibbing (Germany),
Giulio G. Stefanini (Italy), Stephan Windecker (Switzerland), Rashmi Yadav (UK),
Michael O. Zembala (Poland).
2
www.escardio.org/guidelines 2018 ESC/EACTS Guidelines on myocardial revascularisation
European Heart Journal (2018) 00, 1-96 - doi:10.1093/eurheartj/ehy394
Aktuelle ESC 2018 Leitlinie
Recommendations Class Level
Pre-treatment and antiplatelet therapy
Aspirin is recommended for all patients without contraindications at an
initial oral loading dose of 150-300 mg (or 75-250 mg i.v.), and at a I A
maintenance dose of 75-100 mg daily long-term.
A P2Y12 inhibitor is recommended in addition to aspirin, maintained over
12 months unless there are contraindications such as an excessive risk I A
of bleeding. Options are:
• Prasugrel in P2Y12-inhibitor naïve patients who proceed to PCI
I B
(60 mg loading dose, 10 mg daily dose).
• Ticagrelor irrespective of the preceding P2Y12 inhibitor regimen
I B
(180 mg loading dose, 90 mg b.i.d.).
• Clopidogrel (600 mg loading dose, 75 mg daily dose) only
when prasugrel or ticagrelor are not available or are I B
contraindicated.
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018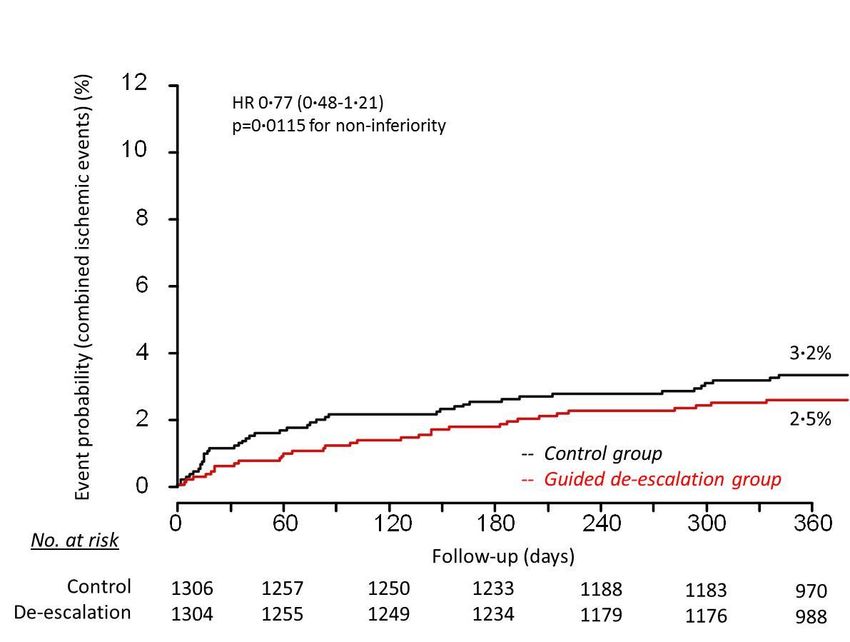
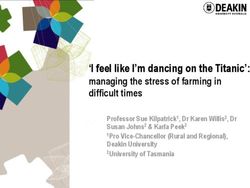
DAPT Dauer: NSTEMI
Antithrombotic Treatment in Patients Undergoing Percutaneous Coronary Intervention
Treatment Indication NSTE-ACS
(Pre-) Treatment DAPT A T C
High Bleeding Risk
Time
No Yes
1 month A P A T
or or
3 months A T A C Antiplatelet drugs :
DAPT Duration
or
A C
6 months DAPT A Aspirin
6 months
12 months DAPT C Clopidogrel
12 months
A T or P Prasugrel
30 months A P A C
T Ticagrelor
DAPT >12 months
36 months
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018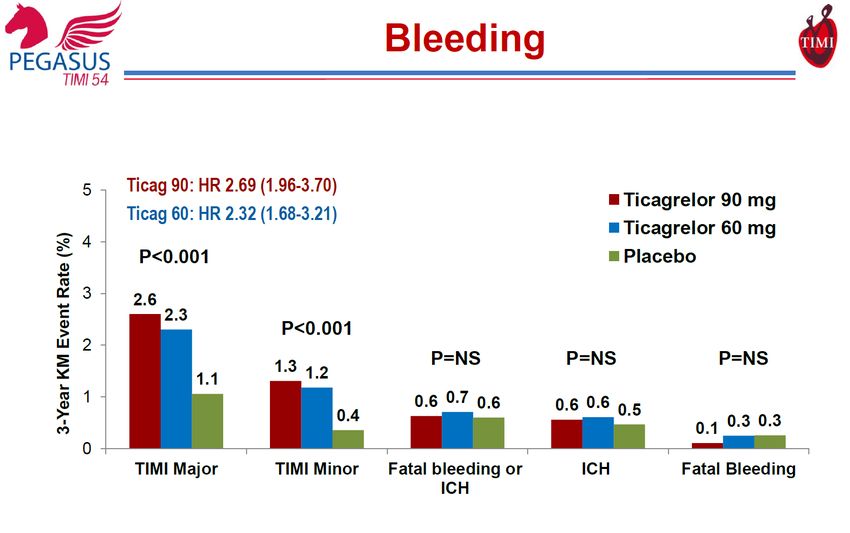
DAPT Dauer: STEMI
Antithrombotic Treatment in Patients Undergoing Percutaneous Coronary Intervention
Treatment Indication STEMI
(Pre-) Treatment DAPT A T P C
High Bleeding Risk
Time
No Yes
1 month A P A T
or or
A T A C Antiplatelet drugs :
3 months
DAPT Duration
or
A C
6 months DAPT A Aspirin
6 months
12 months DAPT C Clopidogrel
12 months
A T or P Prasugrel
30 months A P A C
T Ticagrelor
DAPT >12 months
36 months
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018Triple: Was? Wielange?
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018NOACs & Triple
Dual antiplatelet therapy duration in patients
with indication for oral anticoagulation
Recommendations Class Level
Dual therapy with clopidogrel 75 mg/day and an OAC should be
considered as an alternative to 1-month triple antithrombotic
therapy in patients in whom the bleeding risk outweighs the IIa A
ischaemic risk.
NEW:
In patients with non-valvular AF requiring anticoagulation and
IIa A PIONNER
antiplatelet treatment, a NOAC should be preferred over VKAs. RE-DUAL
In patients with an indication for a VKA in combination with aspirin
and/or clopidogrel, the dose intensity of the VKA should be care-
IIa B
fully regulated with a target INR in the lower part of the re-
commended target range and time in the therapeutic range >65%.
Discontinuation of antiplatelet treatment in patients treated with
IIa B
OAC should be considered at 12 months.
20
www.escardio.org/guidelines 2018 ESC/EACTS Guidelines on myocardial revascularisation
European Heart Journal (2018) 00, 1-96 - doi:10.1093/eurheartj/ehy394Agenda 1) Was sind die aktuellen Empfehlungen zur dualen Plättchenhemmung bei ACS Patienten ? 2) Strategien zur Individualisierung der Plättchenhemmung in 2018: Länger? Kürzer? De-Eskalation?
Scores
2017 ESC/EACTS DAPT Guidelines, EHJ 2017DAPT Eskalation
• GRAVITAS
• TRIGGER-PCI Kein Benefit einer „Guided* Eskalation“
• ARCTIC
*Guided = gesteuert durch Plättchenfunktionstestung
Price et al., JAMA 2011, Trenk et al., JACC 2012, Collet et al., NEJM 2012Prasugrel: Ischämien vs.
Blutungen
Akute Phase Chronische Phase
Antman et al., JACC 2009, Wiviott et al., NEJM 2007Ticagrelor: Ischämien vs.
Blutungen
PLATO
Definite ST
Becker et al., EHJ 2011; Velders et al., Heart 2016Real-World Daten zu DAPT De-
Eskalation (Switching)
DAPT De-Eskalation 15 % 28 %
Zettler et al., AHJ 2017TOPIC Studie
PRO
Cuisset et al., EHJ 2017SCOPE Register
CONTRA
De Luca et al., Eurointervention 2017Clopidogrel: Wirkung &
Outcome
20,839 Patienten
Plattchenfunktionstestung (PFT) als “Tool” um eine DAPT De-Eskalation
sicherer zu machen
Gurbel et al., Circulation 2003 Aradi, …, Sibbing, EHJ 2015Patienten & Studienarme
Control
(n=1306)
@ 2 weeks after discharge
Adherence to treatment:
unchanged
PFT (Multiplate analyser)
11 ½ months
14 days prasugrel
>94% in both groups
prasugrel
therapy
Biomarker
Hospital discharge
positive ACS
patients R*
(n=2610) with 1:1 Guided de-escalation
Low
successful (n=1304)
PCI Responders 11 ½ months
prasugrel
(40%)
7 days 7 days
Good
prasugrel clopidogrel
Responders 11 ½ months
(60%) clopidogrel
Dec 2013 – 98% 96%
May 2016
Follow-up:
@ 2 weeks @ 12 months
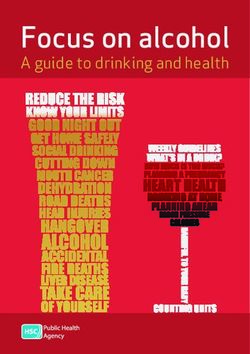
Sibbing et al., Lancet 2017Primärer
Studienendpunkt
10
(CVD, MI, stroke, BARC ≥2) 9·0%
Event probability (%)
8
7·3%
6
HR 0·81 (0·62-1·06)
4 p=0·0004 for non-inferiority
(p=0·1202 for superiority)
2
-- Control group
-- Guided de-escalation group
0
No. at risk
0 60 120 180 240 300 360 (days)
Control 1306 1238 1220 1190 1132 1124 924
De-escalation 1304 1234 1213 1189 1129 1124 942
Sibbing et al., Lancet 2017Sekundäre
Studienendpunkt
Blutungen (BARC 1-5) Ischämien
(CVD, MI, stroke)
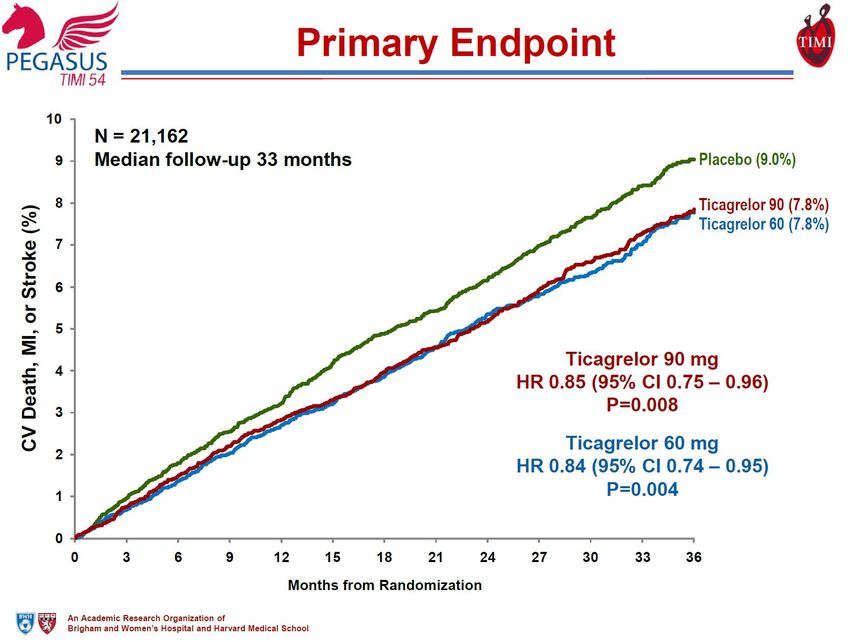
Sibbing et al., Lancet 2017PEGASUS: Primärer
Endpunkt
ARR: 1.2%
RRR: 15%
NNT: 84
Bonaca et al., NEJM 2015PEGASUS: Blutungen
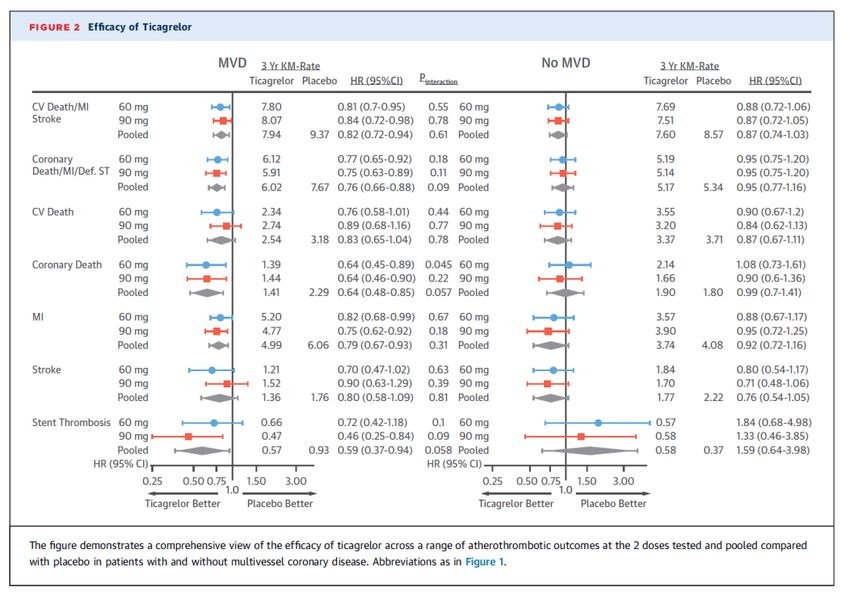
Bonaca et al., NEJM 2015PEGASUS: Mehrgefäß-KHK Bansilal et al., JACC 2018
DAPT Alternativen in 2018
Recommendations Clas Leve
s l
De-escalation of P2Y12 inhibitor treatment (e.g. with a
switch from prasugrel or ticagrelor to clopidogrel) guided TROPICAL-ACS
by platelet function testing may be considered as an IIb B TOPIC
alternative DAPT strategy, especially for ACS patients
deemed unsuitable for 12-month potent platelet inhibition.
In patients with ACS who have tolerated DAPT without a
bleeding complication, continuation of DAPT for longer IIb A PEGASUS
than 12 months may be considered. DAPT
∑: Alternative DAPT Strategien zur DAPT Eskalation und De-eskalation
2018 ESC/EACTS guidelines on myocardial revascularization, EHJ 2018Zusammenfassung
• Standards zur Plättchenhemmung nach ESC Leitlinie sind eine 12
monatige DAPT Dauer mit ASS + Prasugrel oder Ticagrelor und
eine 6 monatige DAPT Dauer bei hohem Blutungsrisiko
• Alternative Strategien und DAPT Optionen sind
a) eine verlängerte DAPT Dauer mit potenten
Plättchenhemmern wenn das Ischämierisiko überwiegt
b) sowie eine verkürzte DAPT Dauer oder eine DAPT De-
Eskalation bei hohem Blutungsrisiko oder aus sozio-
ökonomischer Indikation
• Aktuelle Leitlinien unterstützen eine individualisierte Therapie in
ausgewählten Fällen und insb. i.R. einer DAPT De-EskalationVielen Dank für die Aufmerksamkeit!
You can also read