Monaco Age 2019 Des essais cliniques à la vraie vie: une route sinueuse pour les patients âgés - Dr Benoit BLANCHET - Monaco Age Oncologie
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Monaco Age 2019
Des essais cliniques à la vraie vie:
une route sinueuse pour les patients âgés
Dr Benoit BLANCHET
UF de Pharmacocinétique et Pharmacochimie
Hôpital Cochin, Paris
1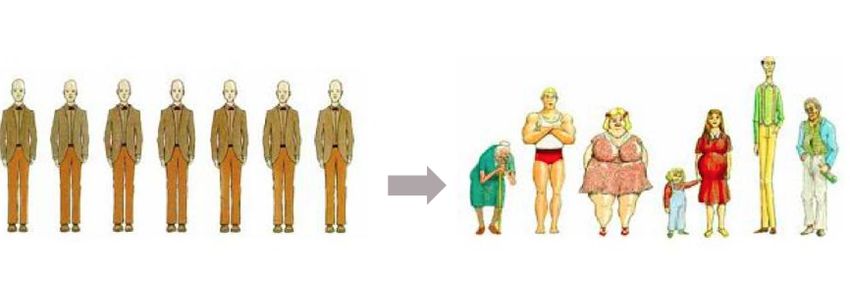
Immunothérapie et personnes âgées
Anti-PD1 Anti-PDL1
(nivolumab, pembrolizumab) (durvalumab, atezolizumab)
Variabilité
+ +
interindividuelle PK
Fonction rénale/
pas d’influence pas d’influence
hépatique et PK
Interaction
Non Non
médicamenteuse et PK
Index thérapeutique Large Large
Pas besoin d’adapter la dose
Thérapie ciblée : une question d’équilibre
Toxicité
Surdosage
Efficacité
Médicaments à faible index thérapeutique
TKI « one fit all » : pas si sûr que ça
75 years p value
Adverse events all
61 100 0.003
grade
Trough erlotinib C°
1359 2091 0.024
(ng/mL)
Treatment
3 33 0.005
discontinuation (%)
Concentration résiduelle d’erlotinib à 1 mois Profil de tolérance à 1 mois
4
Bigot et al., Invest New Drugs 2016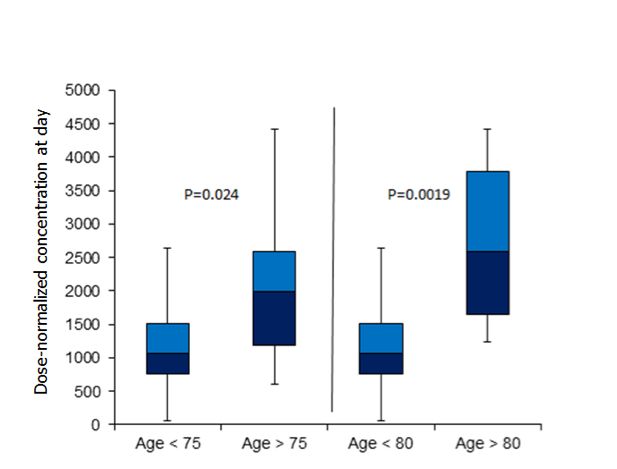
1.24)]. In LL6, PFS did not differ according to baseline BSA [HR tic analyses 1.09 (0.69–1.72)]; there was a slight trend toward improved PFS plasma concentrations with the 40 mg dose among those with BMI ≥25 versus

Complexité chez la personne âgée Comorbidités Altération de la PK (IH, IR, sarcopénie…) (absorption, métabolisme) Polymédication Observance
426 Sarcopénie et toxicité des thérapies ciblées
EUROPEAN UROLOGY FOCUS 4 (2018) 420–434
Table 3 – Studies on skeletal muscle index and treatment toxicity
First author, yr, Study population Timing of Level of Tissue Outcome Results p value Adjustment
country (ref) CT scan analysis, image comparison factors
software
used
Antoun, 2010, 55 mRCC patients Close to L3, Slice-O-Matic Low SMIa (19 M) vs DLT, % 37 vs 5.5 0.04 Univariable
France [25] treated with sorafenib treatment high SMI (18 M)
from 2003–2005 initiation Low SMI and BMI 25 kg/m2
(30 M)
Low SMI and BMI 25
kg/m2 (38 M+F)
Huillard, 2013, 61 mRCC patients "1 mo before L3, ImageJ Low SMIa and BMI 25 kg/m2
(38 M, 23 F) (n = 41)
Cushen, 2014, 55 clear cell mRCC # 1 mo of L3, Osirix SMI, Q1 (< 44.8) DLT, %c 92 vs 57 0.05 Univariable
Ireland [26] patients treated with treatment (n = 13) vs Q4 (> 63.2)
sunitinib from 2007– initiation cm2/m2 (n = 14)
2012 (43 M, 12 F) Low SMIa (n = 18) vs DLT, %c 77.7 vs 70 NS
high SMI (n = 37)d
Ishihara, 2016, 71 mRCC patients "1 mo before L3, Toshiba Low SMIe (n = 45) vs DLT, %b 51.1 vs 50.0 0.93 Univariable
Japan [27] treated with sunitinib treatment high SMI (n = 26)
from 2007–2014 initiation
(50 M, 21 F)
BMI = body mass index; DLT = dose-limiting toxicity; F = female; L3 = third lumbar vertebra; M = male; mRCC = metastatic renal cell cancer; Q = quartile;
ref = reference; SD = standard deviation; SMI = skeletal muscle index.
a
Sex-specific cut-off values for SMI were 55.4 cm2/m2 for males and 38.9 cm2/m2 for females.
b
VrielingAfter
c
one Eur
et al., cycle.
Urol Focus 2018Polymédication et cancer
Country Number of Age, years Number of Patients taking over- Patients taking complementary
patients prescribed drugs the-counter drugs (%) and alternative medicines (%)
Cashman et al3 UK 100 Median 73·5 (IQR 65–88) Median 7 (IQR 1–17) NR NR
Puts et al5 Canada 112 Mean 74·2 (SD 6, IQR 65–92) Median 5 (IQR 3–9) NR NR
Hanigan et al12 USA 52 Range 44–85 Mean 5·5 (IQR 0–13) 71%; mean 2·2 drugs 69%; mean 1·9 (IQR 0–11)
(IQR 0–20)
Sokol et al13 USA 100 Median 78 (IQR 70–90) Mean 9·1 (prescribed NR ~50%
and over the counter)
Werneke et al14 UK 318 NR NR NR >50%
NR=not reported.
Table 1: Polypharmacy reports of patients with cancer
medicines; for example, over-the-counter products such In a community-based practice in the USA, Sokol and
Risques d’interactions pharmacocinétiques:
as analgesics, cough and cold remedies, or so-called colleagues reported use of CAMs such as vitamins or
complementary and • Absorption
alternative digestive
medicines: IPP(CAMs), herbal medicines in nearly half of 100 patients aged
• voiesand
including herbal remedies métaboliques : CYP3A4+++
supplements.7,9,12 (inducteurs,
Whatever 70 inhibiteurs)
years or older. 13
One of these medicines was
the precise defi • nition,
Protéinesappropriate or rational
d’efflux : P-gp, BCRP St John’s wort (Hypericum perforatum), which is known
polypharmacy is becoming more common because of the to interact with cancer drugs such as imatinib and
numerous therapeutic options available for treatment of irinotecan, with potential adverse outcomes.6 All patients
8
medical
Lees disorders,
et al., Lancet especially in elderly patients. were taking a mean of 9·1 prescription and non-
Oncol. 2011Interactions médicamenteuses :
Published OnlineFirst February 14, 2019; DOI: 10.1158/1078-0432.CCR-18-2748
un sujet non anodin
Mir et al.
PFS duration OS duration
A Concomitant GAS therapy/pazopanib (80% treatment administration)
B Concomitant GAS therapy/pazopanib (80% treatment administration)
100 100
90 90
80 80
70 70
60 60
50 50
40 40
30 30
20 20
10 10
0 0 (Months)
0 2 4 6 8 10 12 14 16 18 0 6 12 18 24 30 36 42 48
O N Number of patients at risk: O N Number of patients at risk: Concomitant
265 274 220 145 105 85 52 39 30 26 213 274 220 137 98 53 22 8 4 No
57 59 39 23 15 11 8 4 3 3 51 59 37 20 14 4 1 1 0 Yes
PFS duration OS duration
C Concomitant GAS therapy/placebo (80% treatment administration) D Concomitant GAS therapy/placebo (80% treatment administration)
100 100
90 90
80 80
70 70
Mir et al., Clin Cancer Res 2019
60 60et les médecines complémentaires :
pas un mythe!
2
7
TIMC‐IMAG
8
Clinique de Pneumolo
Bruno Revol, Centre R
RE FE RE NC ES
1. Horneber M, Buesch
many cancer patients
tematic review and m
2. Berretta M, Della Pe
alternative medicine
survey. Oncotarget.
FIGURE 1 Evolution of serum transaminase levels and crizotinib
3. Firkins R, Eisfeld H
concentration depending on the use of ginger and crizotinib. ASAT, alternative medicine
aspartate aminotransferase; ALAT, alanine aminotransferase tions. J Cancer Res C
4. Awortwe C, Makiwa
Revol et al., Br J Clin Pharmacol 2019 Critical evaluation oMédecines complémentaires en cancérologie
■ Interactions au niveau des CYP
Ginkgo Biloba
■ inhibition CYP3A4 et CYP2C19
Ginseng
■ inhibition CYP3A4
Echinacea
■ induction CYP3A4
Kava Kava
■ induction CYP3A4
■ toxicité hépatique ++
Millepertuis
■ induction nombreux CYP
■ Principaux sites pour informations
■ OCCAM (Office of Cancer Complementary and Alternative Medicine) http://cam.cancer.gov/cam/
■ NCCAM (National Center for Complementary and Alternative Medicine): http://nccam.nih.gov/
■ NCI (National Cancer institute) http://www.cancer.gov/cancertopics/cam 11
■ MSKCC (Memorial Sloan Kettering Cancer Center) http://www.mskcc.org/cancer-care/integrative-medicine
Slide from Dr A. Thomas SchoemannEvaluation pluridisciplinaire des risques
• RCP dédiée d’individualisation thérapeutique
Evaluation gériatrique Infirmière Comorbidités
Gériatre coordinatrice Cardiologue
Diabétologue
Risque iatrogénique
Pharmacien
Diététicienne
Psychologue
Assistante sociale
Oncologue
Venue spécifique en HDJ
Prescription sécurisée et individualisée
Médecine intégrée > médecine personnaliséeSuivi Thérapeutique Pharmacologique
• Adapta&on posologique
• Tolérance acceptable
• Réponse clinique
13Take home messages thérapies ciblées
Recommandations pratiques
Altération rénale ou Si polymédication
Sarcopénie
hépatique importante
Médicaments à privilégier
Inhibiteurs de PARP ou CDK Médicaments à privilégier
IR IH
• Initiation à dose réduite • Inhibiteurs de PARP
Inhibiteurs de PARP • Niraparib
• Augmenter la dose ou pas • Niraparib Niraparib • Talazoparib
• en fonction de la toxicité • Olaparib Talazoparib • Veliparib
• Ribociclib Veliparib
• STP si possible pour vérifier • Inhibiteurs de CDK
exposition plasmatique Inhibiteurs de CDK • Abemaciclib
• Abemaciclib • Palbociclib (sauf si inducteur)
• Palbociclib
1415
You can also read