PEDIATRIC ANXIETY DISORDERS: TIPS AND TECHNIQUES FROM A CHILD PSYCHIATRIST
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
“Anxiety disorders are the most common mental health diagnoses in youth,
and carry risks for ongoing impairments and subsequent development of
other psychiatric [and medical] comorbidities into adulthood. ”
PEDIATRIC ANXIETY DISORDERS: TIPS AND
TECHNIQUES FROM A CHILD PSYCHIATRIST
Karen Seroussi DO
Vibrant Minds Child and Adolescent Psychiatry
Austin, TX
DISCLOSURES • I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME activity. • I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

OBJECTIVES Review the clinical presentation of anxiety in children and adolescents Discuss evidence-based treatment modalities, therapies medication Identify environmental supports for the anxious child parent-mediated interventions community and educational resources.

NEED FOR INTERVENTION IN PRIMARY
CARE
• ~20% of children experience mental health issues
• >50% of mental health issues start before age 14
• Delay of onset of treatment for youth is 8-10 yr
• Increased risk for co-morbid disorders that affect behavior and learning
• Access to mental health services; only 20% receive treatment
• Pediatricians are considered the “first resource” for parents
• In many areas, there are no other options
5); ); NIMH (2005).
EPIDEMIOLOGY • Prevalence: • Any anxiety disorder 6-20% (often comorbid) • Separation Anxiety disorder ; children 4.1-12.% and adolescents 1.3% school refusal • Social Anxiety disorder; 3.9 – 6.9% • GAD; 2.9-4.6% • Gender distribution is equal in children and female > male in adolescents • Risk factors • 2-3x risk of depression as an adult • Increased risk of underachieving as young adults • Increased rate of substance use disorders

INFANCY OF PEDIATRIC ANXIETY • Predisposition to sensitive temperament • Can be seen as rigidity or reactivity • Environmental component • Traumatic event(s) • Change(s) in care • Childcare/parenting interaction • Repetitive behavior pattern, often with identifiable trigger: • Separation • Social interaction • Trying new things • Theory = genetic variant (ie SNP or receptor predisposition) +/- neuronal circuitry changes

ROLE OF PARENTAL MATCH/MISMATCH • Match/mismatch coined by Temperament research in the 1960’s (Chess and Thomas) – “goodness of fit” • Mental Health psychopathology in the parent • Higher risk for co-morbidities and lifelong mental health issues • Higher risk for lifelong health issues (ACES study) • Decreased ability to make changes to their behavior • Recommendations • Stronger need for Family Therapy • Monitor for comorbid disorders • More likely to need medication treatment • High functioning parents • Decreases the level of treatment needed • Parents can rapidly improve the environment

PRESENTATION • Internalizers • Fear without recognizing it is unreasonable or out of proportion • Refusal to do age-appropriate behavior • Somatic complaints • Self-critical statements • Seek excessive reassurance • Often perfectionistic • Misinterpret social interaction and their own performance or behavior • Externalizers • Irritable • Angry outbursts • Phobic behavior • Risk of substance use

SCREENING
• Considered a minimum standard in pediatric mental health treatment
• Initial evaluation
• Tracking progress
• Question is who to screen??
• Parents
• Often poor identifiers of the child’s inner experience
• Good assessment of impact on family and school fxn
• Children -- Risk to results if the child wants to please or not worry the interviewer or is not cooperative
• Validated Tools
• SCARED – general screen and also subscales available
• SPIN – Social Phobia inventory
• GAD-7 – only 7 questions, not for young children
Screen for Child Anxiety Related Disorders (SCARED)
PARENT Version—Page 1 of 2 (to be filled out by the PARENT)
Developed by Boris Birmaher, M.D., Suneeta Khetarpal, M.D., Marlane Cully, M.Ed., David Brent, M.D., and Sandra McKenzie, Ph.D.,
Western Psychiatric Institute and Clinic, University of Pittsburgh (October, 1995). E-mail: birmaherb@upmc.edu
See: Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999). Psychometric properties of the Screen for Child
Anxiety Related Emotional Disorders (SCARED): a replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10),
1230–6.
Name: __________________________________________ Date: __________________________________
Directions:
Below is a list of sentences that describe how people feel. Read each phrase and decide if it is “Not True or Hardly Ever True” or
“Somewhat True or Sometimes True” or “Very True or Often True” for your child. Then, for each statement, fill in one circle that
corresponds to the response that seems to describe your child for the last 3 months. Please respond to all statements as well as you
can, even if some do not seem to concern your child.
0 1 2
Somewhat
Not True True or Very True
or Hardly Sometimes or Often
Ever True True True
1. When my child feels frightened, it is hard for him/her to breathe O O O PN
2. My child gets headaches when he/she am at school. O O O SH
3. My child doesn’t like to be with people he/she does't know well. O O O SC
4. My child gets scared if he/she sleeps away from home. O O O SP
5. My child worries about other people liking him/her. O O O GD
6. When my child gets frightened, he/she fells like passing out. O O O PN
7. My child is nervous. O O O GD
8. My child follows me wherever I go. O O O SP
9. People tell me that my child looks nervous. O O O PN
10. My child feels nervous with people he/she doesn’t know well. O O O SC
11. My child gets stomachaches at school. O O O SH
12. When my child gets frightened, he/she feels like he/she is going crazy. O O O PN
13. My child worries about sleeping alone. O O O SP
14. My child worries about being as good as other kids. O O O GD
15. When my child gets frightened, he/she feels like things are not real. O O O PN
16. My child has nightmares about something bad happening to his/her parents. O O O SP
17. My child worries about going to school. O O O SH
18. When my child gets frightened, his/her heart beats fast. O O O PN
19. He/she child gets shaky. O O O PN
20. My child has nightmares about something bad happening to him/her. O O O SPD/DX
• Medical comorbidities or primary disorders
• Pulmonary (allg, asthma) • Medication SE
• Endocrine (DM, thyroid) • ASD/ ADHD/learning disorders
• CNS issues • Abuse
• Cardiac (ie conduction defect) • Caffeinism
• Anxiety disorders
• Separation Anxiety Disorder • Panic Attack Specifier
• Social Anxiety Disorder • Agoraphobia
• Generalized Anxiety Disorder • Substance/Medication-Induced
• Selective Mutism • Secondary to Medical Condition
• Specific Phobia (animal, nature, • Other Specified Anxiety Disorder
med, situation, other) • Unspecified Anxiety Disorder
• Panic DisorderTREATMENT
• Multi-modal is standard of care
• Environmental support [CATEG [CATEG
ORY ORY
• Home NAME] NAME]
• School
• Community programs
• Therapeutic modalities
• Medication [CATEG
ORY
NAME]
• When is medication necessary?TREATMENT CONSIDERATIONS
• Acuity
• Severity of sx
• Duration of sx
• Parent psychopathology
• Parenting interaction pattern = match/mismatch
• Educational Setting
• Family’s ability or desire to participate in treatment
• Child’s ability and willingness to actively engage in treatment
• CAMS = Child and Adolescent Anxiety Multimodal Study
• RCT – 448 patientsC AMS: CHILD AND ADOLESCENT
MULTIMODAL STUDY
• Study type and participants: RCT for 488 children ages 7 years to 17 years, all had moderate to severe
separation anxiety disorder, generalized anxiety disorder or social phobia. Many also had coexisting disorders,
including other anxiety disorders, attention deficit hyperactivity disorder, and behavior problems.
• Study Location: six regionally dispersed sites throughout the United States
• Length of study: treatment length of 12 weeks and then continued follow-up through 9 months
• Methods:
• Cognitive behavioral therapy (CBT)
• Sertraline (Zoloft), a selective serotonin reuptake inhibitor (SSRI)
• CBT combined with sertraline
• Placebo pill (sugar pill).
• Results: Combination treatment, 81 percent improved. Sixty percent in the CBT-only group improved, and 55
percent in the sertraline-only group improved. Among those on placebo, 24 percent improved. A second
phase of the study monitored the children for an additional six months and found that the treatment
outcomes were not lost.CAMS OUTCOMES Piacentini J, Bennett S, et al. 24- and 36-Week Outcomes for the Child/Adolescent Anxiety Multimodal Study (CAMS). J Am Acad Child Adolesc Psychiatry. 2014 Mar; 53(3): 297–310.
MEDIC ATION
SELECTIVE SEROTONIN REUPTAKE
INHIBITORS
Medication Min Indications Dose range Side effects Pearls Studies
age (start, effective, and risks
max)
Fluoxetine 5/6 MDD, 5-10 mg Headache, Always dose in Birmaher 2003
(Prozac) OCD, PTSD 10-40 mg activation AM, long T1/2, Bridge 2007
80 mg weekly
available
Sertraline 6 OCD, MDD 12.5 –25 mg GI sx, daytime Best EBM for Walkup 2008
(Zoloft) 25-150 mg sleepiness, anxiety (CAMS),
200 mg emotional Wagner 2003
blunting
Escitalopram/ 6 MDD, Social 2.5 – 5 mg Sedation, Narrow dose Isolan 2008
(Lexapro) anxiety d/o 5-15 mg headache range
20 mgBLACK BOX WARNING
• Suicidal thoughts, no completed suicides
• Risk of increased SI more prevalent in the depressed child
• (NNH = 143-150)
• Positive outcome favored use of SSRI (NNT = 10)
• Increased risk of 0.7% for anxiety disorders
• Take Home Important points
• Discuss treatment response – it takes awhile to work
• Alleviated with co-occurring therapy
Bridge, 2007 and Compton 2010MEDICATION PRNS
• Anxiolytic
• Hydroxyzine (Atarax) – antihistamine – 12.5 – 25 mg bid or tid, can be sedating
• Buspirone (Buspar) – partial 5HT agonist – 5-10 mg bid or tid with meals, not at bedtime, short
half-life
• Guanfacine (Intuniv,Tenex), Clonidine (Catapres, Kapvay) – alpha-2 agonist - can be sedating
• Gabapentin (Neurontin) – GABA agnoist – 100 – 300 mg bid/tid with meals
• Propranolol (Inderal) - Beta blocker - 20-40 mg bid
• Melatonin 0.3-0.5 mg bid (Cochrane review)
• Benzodiazapines – use with caution
• Risk of disinhibition, decreased memory consolidation, sleep architecture changes,
tolerance/dependence
• AVOID XANAX – highest risk of dependence, street value
• Lorazepam has dual benefit to GI upsetMEDICATION PRNS (CONT) • Insomnia – often the fastest route for improvement • Melatonin 1-5 mg + Magnesium 100-200 mg • Mirtazapine (Remeron) – risk of weight gain , decreases nightmares – 3.75 – 7.5 mg • Trazodone – risk of priapism – 25-100 mg • Doxepin – danger with OD - 3-10 mg • Clonidine – risk of hypotension – 0.1 mg; Guanfacine 1-2 mg • Prazosin - 1-2 mg for nightmares • Hydroxyzine/Benadryl – risk of cognitive dulling – 25 – 50 mg • Supplement • NAC – n-acetylcysteine – anxiety, OCD and repetitive grooming behaviors
GUIDING PARENTS • What not to do • Expecting a child to grow out of it • Teasing or criticizing the fear • Force the child to do the thing they are afraid of • Allow the child to avoid fears entirely • Punishment for behavior • Change their interaction pattern – may need family therapy for guidance • Improve Communication skills • Stay calm; not get pulled into the fears and worries • Be supportive; not punish the behavior • Increase recognition of the desired behavior = operant conditioning
PARENT-DIRECTED INTERVENTIONS
• Improve sleep
• Bedtime routine
• Sleep hygiene
• Parental supervision of electronics
• Parent-guided behavior interventions for younger kids
• Use of self-help books
• Bravery Book /Cheer Chart – parent-guided intervention
• Tangible security object – parent-guided intervention
• Parent-assisted interventions for tweens and teens
• Work on self-help books together
• Skill-building activities (yoga, exercise, gardening, art, etc.)
• Review the day technique - best done during an activity, builds parent-child communication and parent has to use good communication
skillsTHERAPY • Play therapy • Talk Therapy • CBT = cognitive behavioral therapy thoughts • DBT = dialectical behavioral therapy • ACT = acceptance and commitment therapy • Trauma-based therapies • TF-CBT • TBRI feelings behavior • What to teach parents to ask for • How to find a few referrals in your community
EDUCATIONAL ASSISTANCE • In-school resources • Embedded mental health clinic • Social Skills classes • Communities in schools • School-based IDEA resources • Special education vs 504 • How to request services
COMMUNITY RESOURCES • Community organizations • Child therapy centers – ex. Lifeworks • Grief Programs - Wonders and Worries • Community mental health - Austin Child Guidance Center • Support groups for parents and patients • NAMI • Other special populations (ie. LGBT) • Group therapy
RESOURCES FOR PARENTS • Nurtured Heart Approach – book, parent workbook and online seminar http://childrenssuccessfoundation.com/ • TBRI; Trust-based Relational Intervention – http://child.tcu.edu/about-us/tbri/ • Theraplay: http://www.theraplay.org/ • Trauma focused CBT - https://tfcbt.org/ • ACT therapy - https://contextualscience.org/act • DBT therapy - http://www.linehaninstitute.org/certification.php • NAMI; National Alliance on Mental Illness - http://www.nami.org/
BOOK RESOURCES FOR PARENTS
• General parenting skills:
• Dan Siegel books, especially No Drama Discipline and Brainstorm
• Raising Human Beings (Greene)
• Parenting books to deal with challenging behaviors
• Raising Your Spirited Child (Kurcinka)
• Transforming the Difficult Child (Glasser)
• Anxiety Workbooks to do with Children
• Therapeutic exercises for Children http://tinyurl.com/zcutmyr
• What to do guides: http://www.dawnhuebnerphd.com/Books.aspx
• Anxiety Workbooks for Teens
• The Panic Workbook for Teens: Breaking the Cycle of Fear, Worry, and Panic Attacks, (Kissen)
• Mindfulness for Teen Anxiety: A Workbook for Overcoming Anxiety at Home, at School, and Everywhere
Else (Willard)RESOURCES FOR PEDIATRICIANS
• Educational resources for Pediatricians and information sheets for Parents
• AACAP Behavioral Health fact sheets:
http://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/FFF-
Guide-Home.aspx
• Bright Futures https://brightfutures.org/mentalhealth/
• Screening tools
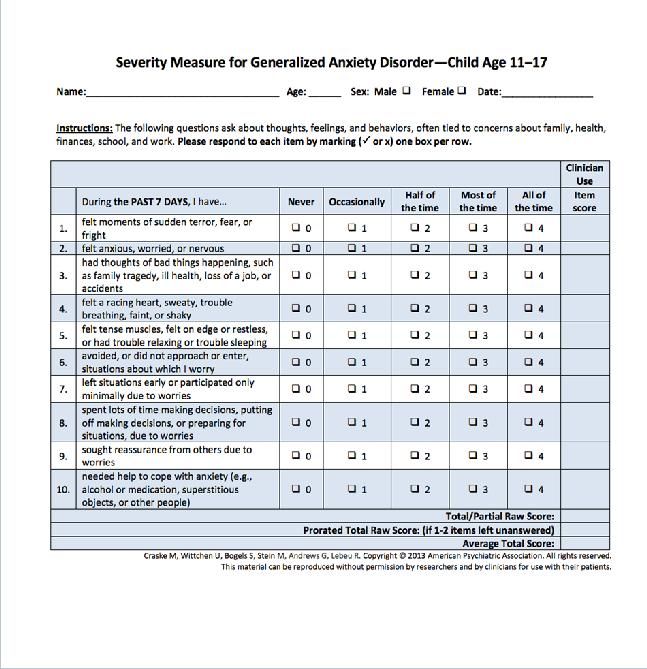
• GAD-7 for adolescents, free tool:
https://www.psychiatry.org/File%20Library/Psychiatrists/Practice/DSM/APA_DSM5_Severity
-Measure-For-Generalized-Anxiety-Disorder-Child-Age-11-to-17.pdf
• SCARED for children, free tool: http://www.midss.org/content/screen-child-anxiety-related-
disorders-scaredREFERENCES
• The Future of Pediatrics: Mental Health Competencies for Pediatric Primary Care. Committee on Psychosocial
Aspects of Child and Family Health and Task Force on Mental Health, J. Pediatrics, July 2009,VOLUME 124 / ISSUE 1.
http://pediatrics.aappublications.org/content/124/1/410.full
• NIMH (Press Release 2005); NRC & IOM (2009); USDHHS (1999); NIMH (2005). Foy et al (2010);
• Spitzer RL, Kroenke K, Williams JBW, Lowe B. A brief measure for assessing generalized anxiety disorder. Arch Inern
Med. 2006;166:1092-1097.
• Hirshfeld-Becker D., Biederman J. Psychopathology in adolescent offspring of parents with panic disorder, major
depression, or both: a 10-year follow-up. Am J Psychiatry. 2012 Nov;169(11):1175-84.
• Compton SN, Walkup JT, Child/Adolescent Anxiety Multimodal Study (CAMS): rationale, design, and methods. Child
Adolesc Psychiatry Ment Health. 2010 Jan.
• Piacentini J, Bennett S, et al. 24- and 36-Week Outcomes for the Child/Adolescent Anxiety Multimodal Study
(CAMS). J Am Acad Child Adolesc Psychiatry. 2014 Mar; 53(3): 297–310.
• Sokolowska E and Hovatta I. Anxiety genetics – findings from cross-species genome-wide approaches. Biology of
Mood & Anxiety Disorders 2013
• Dean O, Giorlando F, Berk M. N-acetylcysteine in psychiatry: current therapeutic evidence and potential mechanisms
of action J Psychiatry Neurosci. 2011 Mar; 36(2): 78–86.REFERENCES
• Beato A, Pereira A, Barros L. Parenting Strategies to Deal with Children's Anxiety: Do Parents Do What They Say
They Do? Child Psychiatry Hum Dev. 2016 Aug
• Kodish I, Rockhill C, Varley C. Pharmacotherapy for anxiety disorders in children and adolescents. Dialogues Clin
Neurosci. 2011 Dec; 13(4): 439–452
• Birmaher B, et al. Fluoxetine for the Treatment of Childhood Anxiety Disorders. Journal of the American Academy
of Child & Adolescent Psychiatry, Volume 42, Issue 4, April 2003, Pages 415–423
• Bridge J, et al. Clinical Response and Risk for Reported Suicidal Ideation and Suicide Attempts in Pediatric
Antidepressant Treatment; A Meta-analysis of Randomized Controlled Trials. JAMA. 2007;297(15):1683-1696.
• Walkup J. et al. Cognitive Behavioral Therapy, Sertraline, or a Combination in Childhood Anxiety. N Engl J Med
2008; 359:2753-2766 December 25, 2008
• Wagner KD, et al. Efficacy of Sertraline in the Treatment of Children and Adolescents With Major Depressive
Disorder; Two Randomized Controlled Trials . JAMA. 2003;290(8):1033-1041.
• Isolan, L, et al An Open-Label Trial of Escitalopram in Children and Adolescents with Social Anxiety Disorder.
Journal of Child and Adolescent Psychopharmacology. January 2008, 17(6): 751-760.
• Hansen MV, et al. Melatonin for pre- and postoperative anxiety in adults. Cochrane review. Pub online
http://www.cochrane.org/CD009861/ANAESTH_melatonin-pre-and-postoperative-anxiety-adults. April 2015You can also read