Voice Characteristics in Patients with Thyroid Disorders
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Eurasian J Med 2019; 51(2): 101-5 Original Article
Voice Characteristics in Patients with Thyroid Disorders
Lejla Junuzović-Žunić1 , Amela Ibrahimagić1 , Selma Altumbabić2
ABSTRACT
Objective: This study investigated acoustic and perceptual characteristics of the voice of patients with thy-
roid gland disorders such as hypothyroidism and hyperthyroidism immediately after the diagnosis was made
and six months later, after using drug therapy.
Materials and Methods: The study includes 20 female outpatients with hypothyroidism and 27 female out-
patients with hyperthyroidism. The criterion for the selection of the patients was a thyroid gland disorder
medical diagnosis, no history of voice disorders and absence of other possible causes of voice changes.
Acoustic, perceptual and aerodynamic parameters were assessed. Acoustic analysis was performed by spe-
cific software. Experienced speech and language pathologists made perceptual voice assessment by using
grade, roughness, breathiness, asthenia, and strain (GRBAS) scale.
Results: Significant differences in patients with hypothyroidism were established on parameter amplitude
perturbation, jitter and noise-to-harmonics ratio between pretreatment and posttreatment period, in which
patients took drug therapy. In group of patients with hyperthyroidism significant difference was noted only
on aerodynamic parameter maximum phonation time. There were a significant differences in all perceptual
parameters in both groups of patients (p
102 • Junuzović-Žunić et al. Voice Changes in Patients with Thyroid Disorders Eurasian J Med 2019; 51(2): 101-5
Patients with untreated thyroid gland diseases tients (mean age, 50 years) with hyperthyroid- deviance, and 3 is severe deviance. The five char-
experience a wide range of symptoms that have ism (age range, 26-74 years). acteristics are grade (G), a description of the de-
a very high impact on the quality of life [10]. gree of hoarseness, which relates to the overall
Currently, few studies are available regarding the Research Tools and Data Collection voice quality, integrating all deviant components;
impact of thyroid diseases on voice production, The study was conducted at the ENT clinic of roughness (R), the perceptual irregularity of vo-
and thyroid gland dysfunction is mainly reported the university clinical center. A speech and lan- cal fold vibrations, abnormal fluctuations in F0
after surgery with regard to the paralysis of the guage pathologist performed an acoustic and or amplitude of vibration; breathiness (B), an au-
recurrent laryngeal nerve or the superior laryn- perceptual evaluation of the patients’ voice. The ditive impression of air leakage through the in-
geal nerve and its impact on patients’ voice [11]. first evaluation was conducted after diagnosing sufficient glottic closure; asthenia (A), the voice
the condition and an examination by an ENT denotes weakness and lack of power; and strain
The aim of this study was to determine the specialist (pretreatment), and the second evalu- (S), reflects a perception of vocal hyperfunction.
acoustic and perceptual characteristics of the ation was done after 6 months (posttreatment). The parameters of aerodynamic measurements
voice of patients with thyroid gland disorders, During this period, patients received drug ther- were also evaluated: maximum phonation time
such as hypothyroidism and hyperthyroidism, apy coordinated by a specialist in nuclear medi- (MPT) of vowel sound “a.”
immediately after the diagnosis was made and 6 cine.
months after drug therapy. The present study was approved by the ethics
The patient’s voice was recorded using the AKG committee of university clinical center. All the
Materials and Methods 190 ES microphone. It was placed at a distance participants provided signed informed consent
of 30 cm and at 45° according to the recom- before they were subjected to the research pro-
Patients mendations of Union of European Phoniatri- cedures.
The participants included female patients with cians [12]. The recording was conducted in a
thyroid gland disorders, such as hypothyroidism sound isolation booth with noise level less than Statistical Analysis
and hyperthyroidism, who were treated at the 40 dB. An average of three trials of prolongation Statistical analysis was performed using the
clinic center. The patient selection criteria were of vowel “a” was used for the acoustic analysis, Statistical Package for Social Sciences (SPSS®)
medical diagnosis of a thyroid gland disorder, i.e., its middle part of the acoustic waveforms software package version 24.0 (IBM Corp., Ar
no history of voice disorders, absence of other for at least 2 seconds. Acoustic voice analysis monk, NY, USA). Descriptive statistics param-
known causes of voice changes, and patients was performed using the computer software eters were calculated. The normality of data
with no history of a previous surgery or trauma Speech Training for Windows, Version 4.00 - Dr. distribution was tested using the Shapiro–Wilk
in the head and neck. The diagnosis was made by Speech and EZ Voice Plus™ Version 2.0. The test. Paired-samples t-test was used to deter-
a specialist in nuclear medicine based on a typi- acoustic vocal parameters assessed were aver- mine differences in the acoustic parameters of
cal clinical examination, determination of hor- age F0, frequency perturbations (jitter), ampli- voice in two related samples of patients in the
mones in serum (thyroid-stimulating hormone tude perturbations (shimmer), and harmonics- pre- and post-treatment phases. The Wilcoxon
[TSH], tri-iodothyronine, thyroxine), and ultra- to-noise ratio (HNR). signed rank test was used to calculate the differ-
sound and palpatory examinations. After the ences of repeated measurements for perceptual
medical diagnosis of a thyroid disease, the pa- The perceptual voice quality assessment was parameters of two related samples. A statistical
tients underwent an ear, nose, and throat (ENT) conducted using the Grade, Roughness, Breathi- level of 95% (pEurasian J Med 2019; 51(2): 101-5 Junuzović-Žunić et al. Voice Changes in Patients with Thyroid Disorders • 103
and post-treatment phases was not changed.
Also, no change in the percentage of the pa-
tients with hypothyroidism and abnormal F0 was
observed, but the percentage of patients with
abnormal values of the other acoustic and aero-
dynamic parameters measured had decreased in
the post-treatment period, wherein the patients
received drug therapy.
Furthermore, tests were conducted to deter-
mine whether there are significant differences
in acoustic and aerodynamic parameters, in gen-
eral, between the pretreatment and posttreat-
ment periods.
Table 1 shows that a significant difference was
found in the variable describing the amplitude
perturbations (shimmer) in patients with hypo-
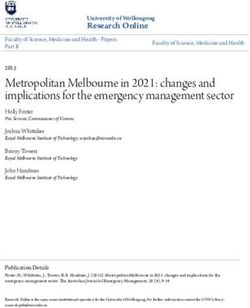
Figure 1. F0-average fundamental frequency; shimmer-amplitude perturbations; HNR-harmonics-to- thyroidism (p=0.032), wherein it was clear that
noise ratio; MPT-maximum phonation time of the vowel sound “a” this parameter had significantly decreased after
treatment. In addition, there was a significant
difference in the variable describing the HNR
(p=0.017); the mean value improved in this
voice parameter posttreatment. Although the
values of the jitter parameter were in the nor-
mal range in patients with hypothyroidism in the
pretreatment phase, there was a significant dif-
ference between pretreatment and posttreat-
ment phases (p=0.03). There were no signifi-
cant changes in pre- and post-treatment periods
on variables describing the voice frequency. F0
was even lower posttreatment. Although insig-
nificant, the mean value of the MPT improved in
the posttreatment period.
When the acoustic voice parameters in patients
with hyperthyroidism in the pre and post-
treatment phases were compared, significant
differences were observed only in the MPT
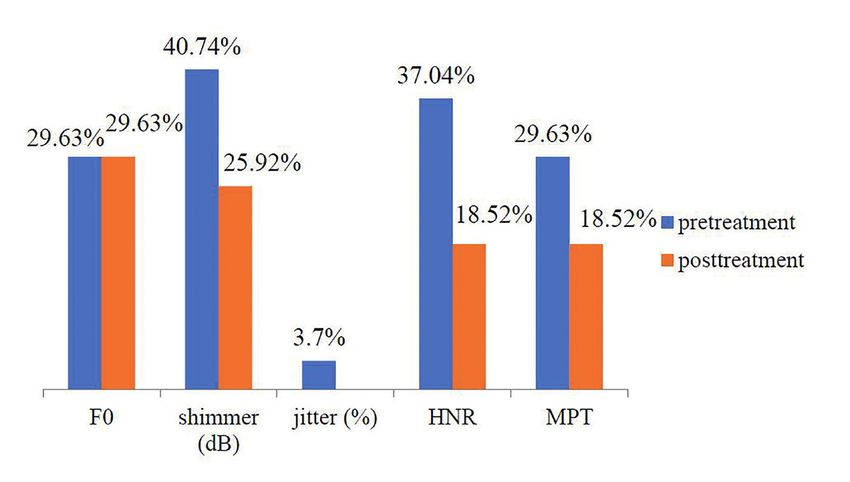
Figure 2. F0-average fundamental frequency; shimmer-amplitude perturbations; jitter-frequency (p=0.004). As in the patients with hypothyroid-
perturbations; HNR-harmonics-to-noise ratio; MPT-maximum phonation time of the vowel sound “a”
ism, the F0 showed a slight decrease in the voice
pitch. Although insignificant, the patients with
Table 2. Results of the Wilcoxon signed rank test on the differences in perceptual voice parameters
in patients with hypo and hyperthyroidism in the pretreatment and post treatment periods hyperthyroidism did have better results for jitter,
shimmer, and HNR in the posttreatment period.
Hypothyroidism Hyperthyroidism
Variable Z p Z p The perceptual voice assessments were also
Grade −1.823 0.068 −1.897 0.058 compared before and after treatment in pa-
Roughness −2.373 0.018 −2.956 0.003
tients with hypo and hyperthyroidism (Table
2). Significant differences were found in all the
Breathiness −1.89 0.059 −2.06 0.039
parameters in patients with hyperthyroidism,
Asthenia −1.298 0.194 −2.913 0.004 except for the grade parameter, but only in the
Strain −2.058 0.040 −2.98 0.003 parameters roughness, breathiness, and strain in
* Wilcoxon signed rank test; Z: standardized test statistic; p104 • Junuzović-Žunić et al. Voice Changes in Patients with Thyroid Disorders Eurasian J Med 2019; 51(2): 101-5
changes in patients with thyroid gland disorders ter, shimmer, and HNR seem to determine the tion widely used in the studies involving patients
[14]. The results of this study showed that the basic perceptual elements of the voice quality: with voice problems [21] including those with a
values of the parameters describing the voice grade, roughness, and breathiness [21]. This breathy and weak voice [25]. In contrast, the re-
frequency ranged within the normal values, and data support results of the perceptual analy- sults of the perceptual evaluation showed signifi-
there was no change in the voice frequency sis performed in the present study, except for cant differences in all observed variables, except
between pretreatment period and the post- the parameter grade that was borderline in- in grade, before and after treatment. Hyper-
treatment period, wherein the patients received significant. Voice hoarseness and loss of voice thyroidism is mainly the cause of hoarseness or
thyroid replacement therapy. Colton [15] stated range are the major features of hypothyroidism. roughness, which is often overlooked [8]. Voice
that women usually produce a basic frequency Hoarseness has a gradual onset and a slow pro- hoarseness is one of the problems that patients
of voice between 180 HZ and 220 Hz, and at gression, thus limiting the patient to notice any often complain about when they undergo vocal
the age of 40–49 years, F0 is 214 Hz [15]. voice changes [22]. Therefore, the voice qual- therapy, although it can often be associated with
ity may be affected by the thyroid gland disease, infection or injuries [4]. Apart from hoarseness,
Although jitter was within the normal values, and some of the symptoms that are referred a number of patients with a high degree of hy-
patients with hypothyroidism showed significant to in literature regarding hypothyroidism are perthyroidism complained of vocal disruption
improvement posttreatment for this parameter. loss of vocal range; reduced voice frequency, [24]. Although some symptoms are very specific
The minor glottic pulse irregularities were even especially in women; vocal fatigue; hoarseness; in hyperthyroidism, the sensitivity in these pa-
less noticeable after the treatment period. Most low voice; and decreased voice intensity [23]. tients when it comes to certain symptoms is low
researchers consider that the normal value of In some cases, mild dysphonia may occur as a (2.9%–28.3%). In addition to hoarseness, a fre-
jitter in adults ranged between 0.5% and 1% result of mild thyroid deficiency. Hoarseness is quent symptom of hyperthyroidism is reported
[16]. a common symptom in patients with hypothy- to be a deep voice. However, the absence of
roidism. Kadakia, Carlson, and Sataloff [1] stat- symptoms does not indicate the absence of thy-
The results also showed that the patients with ed that according to Ritter, the mechanism of roid gland disorders [26].
hypothyroidism had the biggest deviation in the action of the thyroid hormone to the voice is
variables describing shimmer and HNR, and unknown in patients with hypothyroidism, but it During a study conducted on 96 patients with
significant differences before and after treat- is believed to be related to the increased levels thyroid gland disorders, a high prevalence of
ment were established in these parameters. of polysaccharides and the fluid accumulation in deviant perceptual voice features was observed.
The overall average shimmer value for females the lamina propria in the vocal folds, paresis of Most of these abnormalities were mild to mod-
was 0.25 dB and the critical value was 0.48 dB the cords due to the thyroid gland enlargement, erate deviations, and only 8% of the patients
[17]. In the pretreatment period, 40% of pa- myxedema of the cricothyroid muscle, and neu- had clinically significant perceptual abnormalities
tients with hypothyroidism had abnormal shim- ral edema of the vagus nerve [6]. The thicken- [23]. The results of another study showed that
mer, but in the posttreatment period, only 10% ing leads to a decrease in the vibratory capac- there are voice changes in patients with thyroid
had abnormal shimmer. The signal-to-noise ratio ity. Singers with hypothyroidism may complain gland disorders, which was especially evident in
also improved after the treatment. The higher about the limitations associated with the higher the perceptual evaluation. The voice changes in
HNR indicates better voice quality [18]. The vocal range and vocal fatigue. In a number of these patients were not negligible, considering
value of the aerodynamic variable before treat- patients who are singers and experienced voice that the presence of voice change symptoms in
ment was slightly below the normal values, and problems and hypothyroidism, there was an in- patients with thyroid pathology has been report-
it was on the lower limit of normal values after crease in the voice clarity after small doses of ed to range from 9% to 38% [14]. Patients with
treatment. The MPT was approximately 15–20 thyroid hormone replacement [24]. Speech dis- thyroid pathology, apart from other symptoms,
seconds for adults [4]. orders in most patients with thyroid hypofunc- may also complain about voice changes [27], the
tion and voice changes correlate with serum most common being hoarseness, breathiness,
Regarding hypothyroidism, Birkent et al. [19] TSH levels [21]. Birkent et al. [19] stated that strain, and uncertainty about how the voice will
established that after thyroidectomy was per- dysphonia associated with hypothyroidism may sound [28]. Cases of low voice, rough voice,
formed and an appropriate substitution therapy vary in relation to the amount and duration of reduced vocal range, and vocal fatigue were
was applied, a statistically significant increase in hormone deficiency. Certain degree of changes also reported [7]. Although the present study
the F0 parameter was observed, although this in the patient’s thyroid status will affect the voice found significant differences in the posttreat-
parameter was abnormal even prior to the regardless of the absolute value of TSH level at ment period (wherein the patients were under
therapy. The MPT was reduced after therapy, the start of hormone replacement. It is believed drug therapy) in only a small number of acoustic
although not statistically significant, while the that the supplements of thyroid hormones are parameters, which do not include parameters
other objective parameters (jitter, shimmer, usually sufficient to control the symptoms of hy- describing the F0, and not the same parameters
amplitude perturbation quotient, pitch pertur- pothyroidism [1]. in hypo and hyperthyroidism, Birkent et al. [19]
bation quotient, and NHR) showed no signifi- stated that it is possible, with the exemption of
cant changes after hormone replacement. This The assessment results of the acoustic voice the F0 parameter, that other acoustic estimation
was not the case in this study: the patients were parameters in patients with hyperthyroidism parameters cannot detect the subtle changes in
treated only with drugs. In cases of primary hy- showed that the parameters describing the fre- the mass of the vocal fold, and it is unlikely to
pothyroidism, before the substitution therapy quency characteristics were within normal in detect any change without a significant vibra-
was applied, F0, voice turbulence index, and soft most patients, but 29.63% of patients had ab- tory or epithelial disease. In any case, a patient
phonation index differed significantly from the normal F0 in pre- and posttreatment periods. experiences voice changes caused by the thy-
control values of the patients without hypothy- There was significant improvement before and roid gland disorders, and these changes may
roidism [20]. However, only a certain number after treatment only in the variable MPT. MPT disappear completely within 3–6 months after
of patients in this study had voice deviations. Jit- is an indirect measure of the laryngeal func- achieving euthyroidism [22].Eurasian J Med 2019; 51(2): 101-5 Junuzović-Žunić et al. Voice Changes in Patients with Thyroid Disorders • 105
The limitation of this study is the small num- S.A.; Analysis and/or Interpretation - L.J.Ž, A.I., S.A.; 14. de Morais Costa EB, de Araújo Pernambuco L.
ber of patients. Moreover, even though we re- Literature Search – L.J.Ž.; Writing Manuscript – L.J.Ž.; Vocal self-assessment and auditory-perceptual as-
corded all patients’ voices in the morning after Critical Review - L.J.Ž, A.I., S.A. sessment of voice in women with thyroid disease.
Revista Cefac 2014; 16: 967-72. [CrossRef]
the morning routine to diminish fluctuations of
Conflict of Interest: The authors have no conflicts of 15. Roth FP, Worthington CK. Treatment resource
acoustic voice parameters during the day and
interest to declare. manual for speech language pathology. Thomson
enforced the controlled use of voice prior to re- Delmar Learning; 2005.
cording, these factors could still affect the voice Financial Disclosure: The authors declared that this 16. Teixeira JP, Oliviera C, Lopes C. Vocal acoustic
parameters. Further studies should focus on the study has received no financial support. analysis-jitter, shimmer and HNR parameters.
correlation of changes in the patient’s thyroid Proc Technol 2013; 9: 1112-22. [CrossRef]
status and voice with regard to the thyroid hor- References 17. Sorensen D, Horii Z. Frequency and amplitude
mones. 1. Kadakia S, Carlson D, Sataloff RT. The effect of perturbation in voice of female speakers. J Com-
hormones on the voice. J Sing 2013; 69: 571-4. mun Disord 1983; 16: 57-61. [CrossRef]
2. Petrovic-Lazic M. Fonopedija. Belgrade: Naucna 18. Finger LS, Cielo CA, Schwartz K. Acoustic vocal
Thyroid gland disorders cause changes in the
knjiga; 2001. measures in women without voice complaints
voice. Changes in the perceptual character-
3. Dodig K, Kusic Z. Klinicka nuklearna medicina. and with normal larynxes. Braz J Otorhinolaryn-
istics of the voice of patients are particularly Zagreb: Medicinska naklada; 2012. gol 2009; 75: 432-40. [CrossRef]
evident, while the acoustic characteristics are 4. Andrews ML. Manual of voice treatment. Pedi- 19. Birkent H, Karacalioglu O, Merati AL, Akcam T,
less affected by the changes, particularly vari- atrics through geriatrics. Canada: Thomson Del- Gerek M. Prospective study of the impact of thy-
ables describing the voice frequency. The high- mar Learning; 2006. roid hormone replacement on objective voice
est deviations in the voice of these patients are 5. Garber JR, Cobin RH, Gharib H, et al. for the parameters. Ann Otol Rhinol Laryngol 2008;
seen in the acoustic parameters of shimmer and American Association of Clinical Endocrinolo- 117: 523-27. [CrossRef]
HNR. There was an improvement in the voice gists and American Thyroid Association Task- 20. Mohammadzadeh A, Heydari E, Azizi F. Speech
of patients with thyroid gland disorders after force on Hypothyroidism in Adults. Clinical impairment in primary hypothyroidism. J Endo-
practice guidelines for hypothyroidism in Adults: crinol Invest 2011; 34: 431-33. [CrossRef]
the treatment period, as they received therapy.
Thyroid 2012; 22: 1200-35. [CrossRef] 21. Dejonckere PH. Assessment of Voice and Respi-
The results indicate the importance of assess- 6. Altman KW, Haines GK, Vakkalanka SK, Keni SP, ratory Function. In: Remacle M, Eckel HE, eds.
ing and treating the symptoms of changes in the Kopp PA, Radosevich JA. Identification of thyroid Surgery of larynx and trachea. Berlin Heidelberg:
voice of patients with thyroid gland disorders hormone receptors in the human larynx. Laryn- Springer-Verlag; 2010; 11-26. [CrossRef]
and possible the effect of hormone replace- goscope 2003; 113: 1931-4. [CrossRef] 22. Hari Kumar KVS, Garg A, Asjai Chandra NS,
ment therapy, especially on the perceptual voice 7. Melnick LA. Perceptual evaluation of voice in Singh SP, Datta R. Voice and endocrinology.
features. Since there are fewer studies on the patients with thyroid disease. The school of Indian J Endocrinol Metab 2016; 20: 590-4.
effect of thyroid hormone supplements and graduate studies and research department of [CrossRef ]
the long-term follow-up of voice discrepancies education and educational technology: Indiana 23. Bone SL, Vertigan AE, Eisenberg RL. Auditory-
University of Pennsylvania, Master Thesis. 2011. perceptual voice characteristics in pre-operative
after the application of therapy, further studies
8. Kim JE, Rasgon B. The hoarse patient: Asking the patients undergoing thyroid or parathyroid surgery.
should aim at monitoring the effects of thyroid right questions. Perm J 2010; 14: 51-3. [CrossRef] Folia Phoniatr Logop 2012; 64: 87-93. [CrossRef]
hormone replacement therapy on the voice of 9. Solter M. Bolesti stitnjace. Klinicka tireoidologija. 24. Brodnitz FS. Hormones and the human voice.
patients with hypo- and hyperthyroidism. Zagreb: Medicinska naklada; 2007. Bull N Y Acad Med 1971; 47: 183-91.
10. Watt T, Groenvold M, Rasmussen AK, et al. 25. Van Riper C. Speech correction: principles and
Ethics Committee Approval: Ethics committee ap- Quality of life in patients with benign thyroid methods. Englewood Cliffs, N J: Prentice-Hall;
proval was received for this study from the ethics disorders. A review. Eur J Endocrinol 2006; 154: 1954; 469-71.
committee of University Clinical Center Tuzla (02- 501-10. [CrossRef] 26. Canaris GJ, Steiner JF, Ridgway EC. Do traditional
09/2-44/14). 11. McIvor NP, Flint DJ, Gillibrand J, Morton RP. Thy- symptoms of hypothyroidism correlate with bio-
roid surgery and voice-related outcomes. The chemical disease? J Gen Intern Med 1997; 12:
Informed Consent: Written informed consent was Aust N Z J Surg 2000; 70: 179-83. [CrossRef] 544-50. [CrossRef]
obtained from patients who participated in this study. 12. Schutte HK, Seidner W. Recommendation by the 27. Banks CA, Ayers CM, Hornig JD, et al. Thyroid
Union of European Phoniatricians (UEP): Standard- disease and compressive symptoms. Laryngo-
Peer-review: Externally peer-reviewed. izing voice area measurement/phonetography. Folia scope 2011; 122: 13-6. [CrossRef]
Phoniatr (Basel) 1983; 35: 286-8. [CrossRef] 28. Lombardi CP, Raffaelli M, D'Alatri L, et al. Voice
Author Contributions: Concept – L.J.Ž, A.I., S.A.; 13. Hirano M. Psycho-Acoustic Evaluation of Voice. and swallowing changes after thyroidectomy in
Design - L.J.Ž, A.I., S.A.; Supervision – L.J.Ž.; Materials In: Hirano M, editor. Clinical examination of the patients without inferior laryngeal nerve injuries.
– S.A.; Data Collection and/or Processing - L.J.Ž, A.I., voice. New York: Springer-Verlag; 1981: 81-4. Surgery 2006; 140: 1026-32. [CrossRef]You can also read