Premenstrual Dysphoric Disorder (PMDD) - Carlie Benson, MD, PGY4 Department of Psychiatry University of Utah Health - University of Utah ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Premenstrual Dysphoric
Disorder (PMDD)
Carlie Benson, MD, PGY4
Department of Psychiatry
University of Utah Health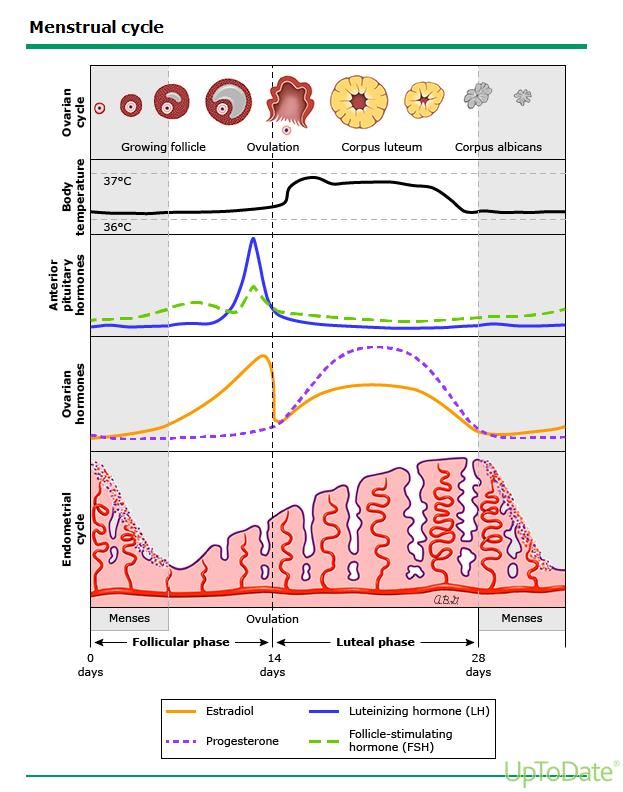
PMDD Diagnostic Criteria
A) 5+ of the following symptoms (need at least 1 from each criterion B & C)
present in the final week before onset of menses (luteal phase), start to
improve within days of menses onset, and become minimal or absent in the
week post-menses (follicular phase) during most menstrual cycles over the
past year:
C) Behavioral/Somatic
B) Affective Symptoms Sypmtoms
1. Affective lability 1. Decreased interest
2. Irritability/Anger 2. Poor concentration
3. Depressed mood 3. Low energy
4. Anxiety 4. Change in appetite
5. Change in sleep
6. Feeling overwhelmed
7. Physical Symptoms*Affective Symptoms
Need 1+ symptoms from this list
1. Affective lability – mood swings, feeling suddenly
sad, increased sensitivity to rejection.
2. Irritability* or Anger – increased interpersonal
conflicts
3. Depressed mood – feeling hopeless, self-
depreciating thoughts
4. Anxiety – tension, feeling keyed-up, restlessnessBehavioral and Somatic
Symptoms
Need 1+ symptoms from this list
1. Decreased interest – work, school, hobbies, relationships
2. Difficulty in concentration – subjective report
3. Low energy* – lethargy, fatigability
4. Change in appetite – overeating, poor appetite, specific food
cravings
5. Change in sleep – insomnia or excessive sleep
6. Overwhelmed – feeling out of control
7. Physical symptoms – breast swelling/tenderness, joint/muscle
pain, bloating*, weight gain, dizziness, hot flashes, headaches.PMDD Dx Criteria Cont. D) The symptoms cause clinically significant distress or functional impairment E) Symptoms are not due to an exacerbation of another disorder (MDD, panic disorder, dysthymia, personality disorder), though can co-occur with other disorders F) Criterion A should be confirmed by prospective ratings during 2+ cycles *prior to confirmation, can be made as a provisional dx G) Symptoms are not attributable to a substance or medical condition
Menstrual History is Key • Detailed menstrual history to confirm relationship of timing of symptoms with cycle • Ask about endogenous hormone use (infertility treatment, HRT, OCPs) • Prospective documentation is required
PMS vs PMDD • PMDD > PMS • PMS –
Disease Course • May begin anytime after menarche and typically continues throughout the reproductive life • Symptoms may worsen in the pre-menopausal period, but then resolve after menopause • Peak severity of symptoms is typically at onset of menses, resolve during follicular phase • The luteal phase is marked by increased risk for suicide • Leads to a high economic burden
Epidemiology • Clinically significant PMS occurs in 3-8% of women • PMDD occurs in 2% of women • Similar rates cross-culturally • May be slightly more prevalent in white women compared to black women
Risk Factors
• Environmental
– Stress
– History of trauma
– Smoking
– Seasonal changes
– Cultural influences
• Genetic
– Exact heritability is unknown
– Premenstrual symptoms have variable heritability, ranging from 30% - 80%
• Oral contraceptives may be protective
– Some hormonal treatments may exacerbate PMDD symptoms
• Comorbidity – history of depressive episodes
– Many other mental or medical diagnosis may have premenstrual
exacerbation of symptomsCopyrights apply
Pathogenesis
• Triggered by changes in female gonadal steroids
(sex hormones) during the luteal phase
– Gonadal steroids are a active in the CNS and interact
with neurotransmitters
– Other peripheral mechanisms
• Due to an underlying sensitivity to changes in
gonadal steroids, not due to the gonadal steroids
themselvesSpecial Populations
• Menstrual irregularities
• Women without menstruation
– Hysterectomy
– Levonorgestrel IUD (Skyla, Mirena, Kyleena,
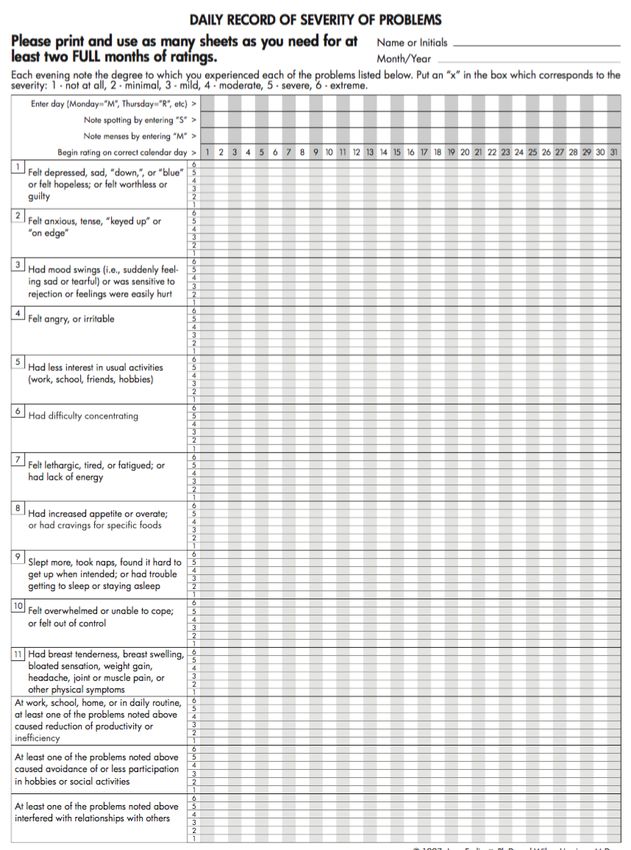
Liletta)Prospective Symptom Trackers • Daily Record of Severity of Problems (DRSP) • Prospective Record of the Impact of Severity of Menstrual symptoms (PRISM) • Premenstrual Symptoms Screening Tool (PSST) • Calendar of Premenstrual Experiences (COPE)
Tracking Apps • Me v PMDD • T2 Mood Tracker • Period Tracker • Mood Log • CLUE Ovulation • iMood Journal Tracker • Plus many more… • Period Tracker Lite
Laboratory Testing • None required • Consider TSH • Consider additional workup for menstrual irregularities (hCG, prolactin, FSH)
Differential Diagnosis • PMS • Dysthymia • Endogenous hormone use • Menopausal transition • Dysmenorrhea • Thyroid disorders • Major Depressive Disorder • Substance use disorders • Bipolar Disorder
Copyrights apply
Serotonergic Treatments
• SSRIs – recommended as first line treatment (non-bipolar
patients)
– sertraline*, citalopram, escitalopram, fluoxetine*
– Similar efficacy as that seen for Tx of MDD
– Benefit can be expected in first cycle
– May treat mood sx > somatic sx
– May respond to lower doses, often doses similr MDD
– No response with 1st SSRI try 2nd SSRI consider trial of 3rd
• SNRIs – paroxetine and venlafaxine (don’t use these)
• Clomipramine (wouldn’t recommend)
* = FDA Approval for PMDDSSRI Dosing Strategies
• Continuous Therapy
– Better for more severe sx, incomplete resolution of
symptoms between cycles, or irregular cycles
• Luteal Phase Therapy
– Starts on day 14 of the cycle and ends at onset of menses
or a few days after
• Symptom Onset Therapy
– Better for women with shorter duration and less severe
symptomsNO ----> Copyrights apply
Oral Contraceptives
• Goal is to suppress the hypothalamic-pituitary-ovarian axis
and ovulation
• Drospirenone (DRSP) containing combined oral
contraceptives (COC) are FDA approved for PMDD
– Start with 3mg DRSP/20mcg EE (4 day pill free interval) 3mg
DRSP/30mcg EE if sx persist/breakthrough bleeding after 3
cycles
– Drospirenone has increased risk of VTE
– If sx persist consider continuous COC vs adding SSRI
• 90mcg levonorgestrel/20mcg EE
• Continuous COCs have higher rates of continuous vaginal bleedingGnRH Agonists rd
– 3 Line Tx
• Only to be tried after trial of SSRI and COCs
• Leuprolide 3.75mg monthly injection
– Given with progestin-estrogen add back
– 1mg oral estradiol + 100mg micronized progesterone
• Can use other equivalent forms of hormones (transdermal)
• Long-term safety of GnRH agonists and
hormonal replacement therapy is unknownSupplements • Possibly helpful – Vitex agnus castus (chasteberry) 20-40mg daily • Maybe helpful, not risk free – Calcium 600mg BID – Vitamin B6 – up to 100mg daily • No data to support – primrose oil, vitamin E, and Mg
Complimentary Treatments • Cognitive Behavioral Therapy – Adjunctively with SSRI • Exercise • Stress reduction • Mindfulness • Diet • Sleep hygiene
Take Home Points • Diagnosis must be confirmed with 2 month prospective symptom tracking • Need symptom free follicular phase for diagnosis • SSRIs are first line treatment, good efficacy • COCs are reasonable first line alternatives to SSRIs • Don’t use alprazolam or paroxetine • Consider non-pharmacologic treatments for mild sx
References
• American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA, American Psychiatric
Association, 2013.
• https://iapmd.org – Information on apps for PMDD symptom tracking
• Pearlstein T et Steiner M. ”Premenstrual dysphoric disorder: burden of illness and treatment update.” J Psychiatry Neurosci 2008;33(4):291-301.
• Schmidt PJ, Nieman LK, Danaceau MA, Adams LF, Rubinow DR. Differential behavioral effects of gonadal steroids in women with and in those
without premenstrual syndrome. N Engl J Med. 1998;338(4):209-216. doi:10.1056/NEJM199801223380401
•
• Uptodate.com. 2020. Uptodate. [online] Available at:
[Accessed 21 October 2020].
• Uptodate.com. 2020. Uptodate. [online] Available at:
[Accessed 21 October 2020].
• Uptodate.com. 2020. Uptodate. [online] Available at:
[Accessed 21 October 2020].You can also read