The challenge of pain in chronic pancreatitis: Assessment and drug treatment - Ajith Siriwardena MD FRCS Professor of Hepatobiliary Surgery ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The challenge of pain in chronic pancreatitis:
Assessment and drug treatment.
Ajith Siriwardena MD FRCS
Professor of Hepatobiliary Surgery
University of Manchester
Consultant Hepatobiliary Surgeon
Manchester Royal Infirmary
Manchester, UK.
.
Disclosures. •Research support from Pharmanord, UK. •Research support from Lilly, Indianapolis, USA.
Outline. 1.Pathophysiology of nociception in chronic pancreatitis. 2.Practical clinical assessment of the patient with suspected chronic pancreatitis. 3.Initial medical intervention.
• Pain is the symptom that most commonly makes the patient
seek medical treatment.
• Pain is the most difficult symptom to control.
• Presentation varies from mild and intermittent to severe and
disabling leading to loss of work and frequent admission to
hospital.
• The potential for narcotic addiction is high.
Gastroenterology 1998;115:763-764.
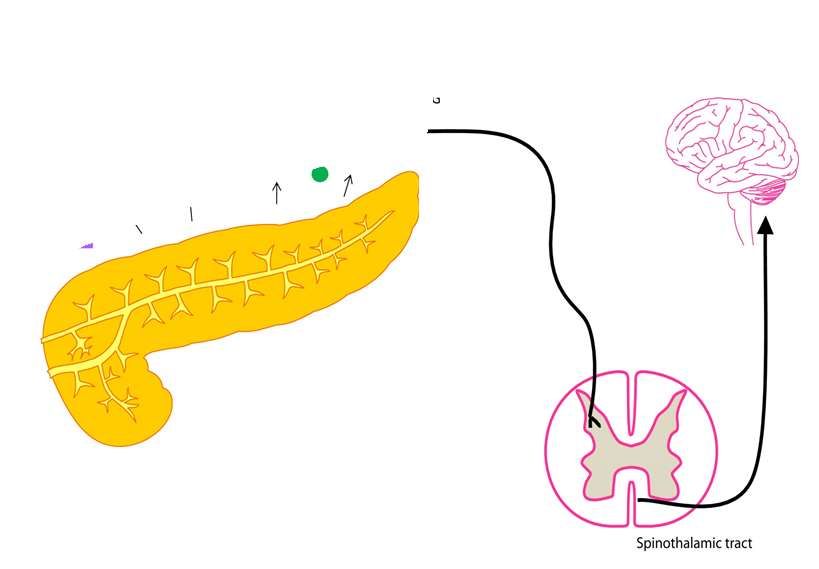
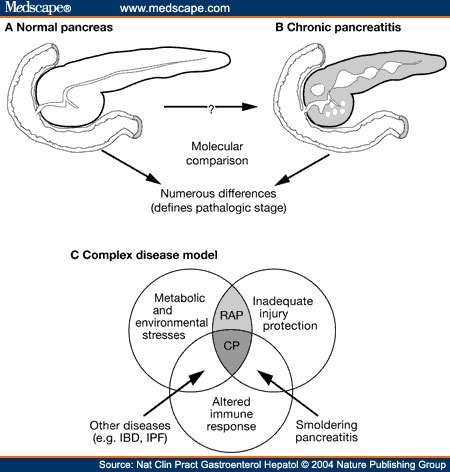
Pancreatic parenchymal causes of pain in chronic pancreatitis.
•Ductal hypertension.
•Glandular inflammation.
•Peri-glandular
inflammation/scarring.• Increased size & altered function of non-
myelinated type C nociceptive neurons.
• Aberrant interaction between nociceptive
neurons and inflammatory cells.
• Trypsin-mediated activation of neuronal sensing
mechanisms.
Altered peripheral nervous system in CP.Structural and functional changes in the brain in CP:
• Changes in EEG, cortical sensing,
• Psychological perceptions of pain
Altered central nervous system in CP.
Forsmark CE. Gastroenterology 2013;144:1282-1291.Practical clinical assessment of pain in chronic pancreatitis.
Practical pathway for care of the patient referred
with “chronic pancreatitis”.
Initial clinical assessment.
Comprehensive clinical assessment (+ lab tests)
(± pancreatic function tests)
+
nutritional assessment including alcohol history*
+
contrast-enhanced CT to pancreas protocol
±
MRCP
±
Endoscopic ultrasound + FNA
(Rosemont criteria for CP).Practical clinical treatment of pain in chronic pancreatitis.
The Recurrence of Acute Alcohol-Associated Pancreatitis Can Be
Reduced: A Randomized Controlled Trial.
Initial episode of Initial episode of
alcohol-related alcohol-related
acute pancreatitis: acute pancreatitis:
Initial intervention Repeated
only. intervention at 6
monthly intervals
number 61 59
Gender (male) 51 50
Self-reported alcohol 2880 3372
consumption in preceding two (288–15,456) (454–13,248)
months (g)
Nordback I et al. Gastroenterology 2009;136:848-855.The Recurrence of Acute Alcohol-Associated Pancreatitis Can Be
Reduced: A Randomized Controlled Trial.
Intervention
30 minute conversation (study nurse in GI OPD).
Focused on three components:
1. Information on toxic effect of alcohol.
2. Need for change and the ability to assume responsibility.
3. Social and personal problems associated with alcohol abuse.
Nordback I et al. Gastroenterology 2009;136:848-855.The Recurrence of Acute Alcohol-Associated Pancreatitis Can Be
Reduced: A Randomized Controlled Trial.
Initial intervention Repeated alcohol
only. guidance.
Re-admissions 16 pts P=0.004 7 pts
30 re-admissions in 15 re-admissions in
these 16 pts these 7 pts.
Repeated counselling at 6-month intervals at the gastrointestinal outpatient
clinic, consisting of an intervention against alcohol consumption, appears to be better
than the single standardized intervention alone during hospitalization
in reducing the development of recurrent AP during a 2-year period.
Nordback I et al. Gastroenterology 2009;136:848-855.Practical pathway for care of the patient referred
with chronic pancreatitis.
Common clinical patterns of chronic pancreatitis.
Large duct disease Small duct disease
± head mass. ± Head mass.
Surgical drainage Pancreatic resection
Or TPIAT
endoscopy
Trial of specific medical therapy.Practical pathway for care of the patient referred
with chronic pancreatitis.
Common clinical patterns of chronic pancreatitis.
Large duct disease Small duct disease
± head mass. ± Head mass.
Surgical drainage Pancreatic resection
Or TPIAT
endoscopy
Trial of specific medical therapy.Pharmacological treatments for pain in chronic pancreatitis: the position in
2015.
Category Evidence for use NICE (UK) guideline
support.
Analgesia : No RCT Yes
NSAID/opiate
Pregabalin 1 RCT Yes
Pancreatic exocrine Meta-analysis of small Yes
replacement RCTs
(none with pain as
principal end-point)
Anti-oxidant therapy Meta-analysis of 9 RCTs No.
Two conflicting RCTsPregabalin. • Binds selectively to voltage sensitive calcium channels and reduces excitability of presynaptic neurons. • Useful in post-herpetic neuralgia.
Methods.
•64 pts with painful CP received pregabalin 150-300mg bd or matched
placebo for 3 weeks as part of an RCT.
•Analgesic effect documented in a pain diary based on VAS.
•Responders were defined as showing a reduction of >30%.
•Pain thresholds to electrical and pain stimulation measured at T10
(pancreas area) and C5 (control) prior to study.
Olesen SS et al. Gastroenterology 2011;141:536-543.
Olesen SS et al. PLOS one 2013;8:e57963-Results.
•Patients with high pain thresholds in T10 and C5 were less likely to respond to
gabapentin.
•The pain responders had an abnormally low threshold to pain at T10
dermatome.
Conclusions.
•Findings need to be confirmed.
•Sustainability of analgesic effect of gabapentin for long-term control not
assessed.
Olesen SS et al. Gastroenterology 2011;141:536-543.
Olesen SS et al. PLOS one 2013;8:e57963-Antioxidant therapy for pain relief in chronic pancreatitis: A systematic
review.
• Nine RCTs of antioxidant therapy in CP including a total of 390 patients.
• Overall, antioxidant therapy was not associated with a reduction in pain in CP
• Standardised mean difference -0.55 (95% CI -1.2 to 0.12; P=0.67).
• Strong evidence that antioxidants increase adverse effects.
• BUT:
• Interventions include antox, compound antioxidant therapy, curcumin, allopurinol and SaME
• Duration of therapy, patient populations, interventions, assessment of interventions and endpoints differ.
• Only one study assessed quality of life.
..Cai G-H et al. Pain Physician 2013; 16:521-532Methods: •Double-blind, placebo-controlled RCT. •MR, ERCP or CT evidence of CP. •No prior pancreatic intervention of any form. •Narcotic addicts (defined according to Am Psych Assocn) excluded. •Study intervention: compound antioxidant therapy in the form of 600 µg selenium, ascorbic acid, β-carotene, α-tocopherol, methionine, (Betamore G Osper Pharmanaurics, India). •Pain assessment: Assessed as number of “painful days” – requirement for analgesia and/or hospitalization. •Drop-out after randomization: 7 in placebo; 0 in antioxidant group.
Patient profiles in the Bhardwaj RCT.
Placebo group Antioxidants group P
(n=56) (n=71)
Median (range) age 29.6 ± 9.3 31.3 ± 11.4 0.345
in years
Etiology: 15:41 25:46 0.206
Alcohol: Idiopathic
If alcoholic – amount 103 ± 71 102 ± 81 0.954
of alcohol (g/d)
Years of alcohol 10 ± 5 9.7 ± 5.9
Main duct dilatation 45 (81%) 55 (77%) 0.535
BMI (kg/m2) 20.2 ±3.1 19.7±3.5 0.372
Undernourished 18 (32%) 28 (39%) 0.547
(BMI < 18.5)*
*6 patients (2 antioxidant; 4 placebo) with a BMI > 25.Primary outcomes in the Bhardwaj RCT.
Placebo group Antioxidants group P
(n=56) (n=71)
n value n value
Number of
painful days 56 7.2 ± 5.3 71 9.1 ±7.6 0.11
prior to
intervention
Number of
painful days 6 53 3.3 ±4.3 66 1.6 ±2.8 0.012*
months after
intervention
Assessed by student’s t-test.Protocol overview: ANTICIPATE study.
Chronic pancreatitis:
Confirmed by CT/MR.
Fecal elastase measurement.
Pain diaries maintained in 1 month run-in.
Randomised, double-blind,
placebo-controlled allocation.
Antioxidant therapy
Antox version 1.2 Matched placebo
(Pharmanord, Morpeth, UK).
Clinic pain scores at Clinic pain scores at
baseline, 2,4,6 months. baseline, 2,4,6 months.
Diary pain scores. Diary pain scores.
QoL assessed by EORTC, QoL assessed by EORTC,
EuroQOL and EQ-VAS. EuroQOL and EQ-VAS.Protocol overview: ANTICIPATE study.
Chronic pancreatitis: Stratified by prior
Confirmed by CT/MR. intervention (1=yes; 0=no)
Fecal elastase measurement.
No formal assessment of
Pain diaries maintained in 1 month run-in. narcotic addiction
Randomised, double-blind,
placebo-controlled allocation.
Antioxidant therapy
Antox version 1.2 Matched placebo
(Pharmanord, Morpeth, UK).
Clinic pain scores at Clinic pain scores at
baseline, 2,4,6 months. baseline, 2,4,6 months.
Diary pain scores. Diary pain scores.
QoL assessed by EORTC, QoL assessed by EORTC,
EuroQOL and EQ-VAS. EuroQOL and EQ-VAS.Protocol overview: ANTICIPATE study.
Chronic pancreatitis:
Confirmed by CT/MR.
Fecal elastase measurement.
Pain diaries maintained in 1 month run-in.
Randomised, double-blind,
placebo-controlled allocation.
Antioxidant therapy
Antox version 1.2 Matched placebo
(Pharmanord, Morpeth, UK).
Clinic pain scores at Clinic pain scores at
baseline, 2,4,6 months.
Primary endpoint baseline, 2,4,6 months.
Diary pain scores. Diary pain scores.
QoL assessed by EORTC, QoL assessed by EORTC,
EuroQOL and EQ-VAS. EuroQOL and EQ-VAS.Table 1. Baseline Demographic and Clinical Parameters
Placebo (37) Antioxidant (33) p
Age at enrolment (y) 50±9 49.8±12.7 0.96
Gender male:female 27:10 23:10 0.80
Disease duration (y) 4.9±4.3 4.2±2.4 0.36
Clinic NRS (SD) 5.0±1.6 5.2±1.6 0.36
Previous intervention yes:no 20:17 18:15 1.00
Aetiology alcohol:idiopathic 27:10 24:9 1.00
ER (MR) CP* 0.19
Equivocal 0 (0%) 1 (6.3%)
Mild 4 (16.7%) 4 (25.0%)
Moderate 15 (62.5%) 9 (56.3%)
Marked 5 (20.8%) 2 (12.5%)
CT 0.13
Calcification 12 (32.4%) 18 (54.5%)
Dilated pancreatic duct 2 (5.4%) 2 (6.1%)
Calcific. & dilated pancr. Duct 23 (62.2%) 13 (39.4%)
Faecal elastase (μg/g) 192±198 221±198 0.56
Alcohol consumption: yes:no 29:8 25:8 1.00
Cigarette smoker: yes:no 28:9 28:5 0.38
Diabetes mellitus: yes:no 11:26 10:23 1.00
Morphine equivalent (mg/d) 91±105 85±114 0.84
* Data available for 24 placebo and 14 antioxidant receiving patients,
d=day, µg=micro gram, kg= kilogram, g=gram, y=years.Table 1. Baseline Demographic and Clinical Parameters
Placebo (37) Antioxidant (33) p
Age at enrolment (y) 50±9 49.8±12.7 0.96
Gender male:female 27:10 23:10 0.80
Disease duration (y) 4.9±4.3 4.2±2.4 0.36
Clinic NRS (SD) 5.0±1.6 5.2±1.6 0.36
Previous intervention yes:no 20:17 18:15 1.00
Aetiology alcohol:idiopathic 27:10 24:9 1.00
ER (MR) CP* 0.19
Equivocal 0 (0%) 1 (6.3%)
Mild 4 (16.7%) 4 (25.0%)
Moderate 15 (62.5%) 9 (56.3%)
Marked 5 (20.8%) 2 (12.5%)
CT 0.13
Calcification 12 (32.4%) 18 (54.5%)
Dilated pancreatic duct 2 (5.4%) 2 (6.1%)
Calcific. & dilated pancr. Duct 23 (62.2%) 13 (39.4%)
Faecal elastase (μg/g) 192±198 221±198 0.56
Alcohol consumption: yes:no 29:8 25:8 1.00
Cigarette smoker: yes:no 28:9 28:5 0.38
Diabetes mellitus: yes:no 11:26 10:23 1.00
Morphine equivalent (mg/d) 91±105 85±114 0.84
* Data available for 24 placebo and 14 antioxidant receiving patients,
d=day, µg=micro gram, kg= kilogram, g=gram, y=years.Table 1. Baseline Demographic and Clinical Parameters
Placebo (37) Antioxidant (33) p
Age at enrolment (y) 50±9 49.8±12.7 0.96
Gender male:female 27:10 23:10 0.80
Disease duration (y) 4.9±4.3 4.2±2.4 0.36
Clinic NRS (SD) 5.0±1.6 5.2±1.6 0.36
Previous intervention yes:no 20:17 18:15 1.00
Aetiology alcohol:idiopathic 27:10 24:9 1.00
ER (MR) CP* 0.19
Equivocal 0 (0%) 1 (6.3%)
Mild 4 (16.7%) 4 (25.0%)
Moderate 15 (62.5%) 9 (56.3%)
Marked 5 (20.8%) 2 (12.5%)
CT 0.13
Calcification 12 (32.4%) 18 (54.5%)
Dilated pancreatic duct 2 (5.4%) 2 (6.1%)
Calcific. & dilated pancr. Duct 23 (62.2%) 13 (39.4%)
Faecal elastase (μg/g) 192±198 221±198 0.56
Alcohol consumption: yes:no 29:8 25:8 1.00
Cigarette smoker: yes:no 28:9 28:5 0.38
Diabetes mellitus: yes:no 11:26 10:23 1.00
Morphine equivalent (mg/d) 91±105 85±114 0.84
* Data available for 24 placebo and 14 antioxidant receiving patients,
d=day, µg=micro gram, kg= kilogram, g=gram, y=years.Figure 2: Clinic NRS Pain Scores
10
Placebo
Antioxidants
8
Pain NRS1
6
4
2
0
0 2 4 6
Month
1 Pain score on the day of the clinic, on a visual analog scale 0-10 (bars show 95%CI)
Clinic reported pain scores were reduced in both groups (change from
baseline at 6 months, placebo: -1.97; antioxidant: -2.33), but were
similar between groups (-0.36, 95%CI: -1.44 to 0.72, p=0.509).Figure 3: Diary NRS Pain Scores
10
Placebo
Antioxidants
8
Pain NRS1
6
4
2
0
0 1 2 3 4 5 6
Month2
1 Pain scored daily on a visual analog scale 0-10 (bars show 95%CI)
2 Monthly average of daily scores
Month 0 denotes the month preceding trial treatmentConclusion In patients with painful chronic pancreatitis of predominantly alcoholic origin, antioxidant therapy does not reduce pain or improve quality of life, despite increasing blood levels of antioxidants.
Integration of the two studies • Strong placebo effect in both studies. • Antioxidant therapy is likely ineffective in alcohol-dominant disease. • Positive findings of Indian RCT do not explain their strong placebo response and may be a result of attention to nutritional detail.
Risks of selenium supplementation.
Baseline selenium status and effects of selenium and vitamin E
supplementation on prostate cancer risk.1
• SELECT: an RCT of selenium + vitamin E (alone or combined) for reduction
of prostate cancer risk.
• 35,333 participants.
• Results:
• Neither selenium nor vitamin E supplementation reduced risk.
• Selenium was associated with a 91% increase in the risk of prostate
cancer (PAnti-oxidant therapy in Chronic pancreatitis:
The position in 2015.
•Antioxidant therapy is likely ineffective in chronic pancreatitis of an
alcoholic aetiology (i.e. about 80 -90% of cases).
•Selenium supplementation is not without risk and pending the
outcome of the EUROPAC study in idiopathic CP, antioxidant therapy
should not be used.Summary: medical management of CP in 2015. •Emphasis on establishing correct diagnosis of CP and counselling on alcohol abstinence. •Consider, non-opiate and opiate analgesia + pancreatic exocrine replacement therapy as baseline. •Trial of gabapentin could be considered. •No longer any role for antioxidant therapy. •Integrate pharmacological treatment with endoscopic and surgical options in a multi- disciplinary forum.
You can also read