To boldly go? Place, metaphor, and the marketing of Auckland's Starship Hospital
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Environment and Planning D: Society and Space 1999, volume 17, pages 201 226
To boldly go? Place, metaphor, and the marketing
of Auckland's Starship Hospital
Robin A Kcarns
Department of Geography, The University of Auckland, Private Bag 92019. Auckland, New Zealand;
e-maii: r,kearns@auckland.ac.n7,
J Ross Barnett
Department of Geography, University of Canterbury Private Bag 4800, Christchurch, New
Zealand; e-mail: r.barnctt@gcog.cantcrbury.ac.nz
Received 28 April 1997; in revised form 3 June 1998
Abstract. In this paper, we place the naming of the Starship Children's Hospital in Auckland, New
Zealand, within the context of increasingly consumer-oriented health care provision. This use of
metaphor alludes to the hospital's distinctive design features and represents an attempt to de-emphasise
connotations associated with institutionalised medicine, thus normalising the place for children.
However, those naming the hospital had more than children in mind. Rather, there was a dual intent:
to market the hospital as a distinctive place for monetary donors, as well as promoting a more therapeutic
environment for youthful users. Through the vehicle of our case study, we raise questions concerning the
competition by health care services for public and private funds. We conclude that there is a need to move
beyond viewing hospitals as service entities and equating health care consumption with utilisation
behaviour. Rather, a merging of insights from the political economy of health care and new cultural
geography literatures can aid the development of morefinelytextured understandings of the meaning
of contemporary health care, and the role of metaphor and marketing in selling places of health care
consumption.
1 Introduction: Sketching the enterprise
"... the new children's hospital in Auckland is going where no other NZ public
hospital has gone before. It is casting off its dull old title and going for something
a little more space-age with its new name 'The Starship'. The enterprising strategy
is part of marketing designed to attract millions of dollars of sponsorship for child
health. Hospital managers believe they can capitalise on the unique design and
colour scheme...and give the centre a new science-fiction-like identity"
(New Zealand Herald 1992a).
In 1992 the recently completed national children's hospital located in Auckland was
officially named 'Starship', a metaphor de-emphasising the institution's medical purposes
and invoking ideas of otherworldliness. This naming, we argue, incorporates a 'nooning'
(Berg and Kearns, 1996) that involves a calculated elision of images ordinarily associated
with medical environments (Shore, 1984). In choosing this name, symbols were being
(re)placed both tangibly and linguistically in an attempt to reorient children's health care
in an era of branding and marketing.
Elsewhere, we have explored the links between culture, place, and health through
examining recent developments in primary health care, a competitive domain in which
distinctive architecture and signs have become widespread in New Zealand (Kearns
and Barnett, 1997). In the present paper we focus on a singular higher-order health
care facility. There is precedent for such specificity of focus in health geography
(Chiotti and Joseph, 1995) as well as local justification as the Starship is the only
tertiary-level facility for children in New Zealand. Previous geographical work on the
hospital sector in New Zealand has been firmly rooted in the welfare tradition and has
focused on issues of distribution and resource allocation (see, for example, Barnett,
1984; Barnett et al, 1980). We specifically focus on the deployment of metaphor in the202 R A Kearns, J R Barnett
design and promotion of the Starship Hospital. It is our contention that clinical
settings which have provided such fertile ground for exploring the power-dynamics of
professional practice (see, for example, Foucault, 1973) are now being materially and
symbolically transformed into arenas of broader consumption practices.
Our decision to consider a children's hospital is both strategic and personal. First,
throughout the developed world there is increasing pressure on hospitals to market
themselves as distinct commodities. Cutbacks in government support, together with
the rise of the for-profit sector and the growth of managed care, have seen the emer-
gence of considerable competition for funds and patients within both the public and
private sectors. With the exception of writers such as James Bohland and Paul Knox
(1989) such trends have received little attention from geographers. We feel this is
unfortunate as there are strong parallels between the 'selling cities' literature (Hall
and Hubbard, 1996; Kearns and Philo, 1993) and trends within the health care sector.
Just as various metaphors, such as the 'urban frontier' (Reid and Smith, 1993), have
been used to facilitate and legitimate gentrification in many US cities, so too have
similar trends appeared in the marketing of health care and hospital services (Kearns
and Barnett, 1997). In this discourse hospitals, just as other parts of the urban realm,
have become commodified and have been rendered attractive to patients and investors
through the conscious manipulation of images and the deliberate creation of cultural-
historical packages. As Briavell Holcomb (1993) notes, the selling of an urban lifestyle
becomes an integral part of an increasingly sophisticated commodification of everyday
life, in which images and myths are relentlessly packaged and presented until they
become 'hyperreaP (that is, elevated from the metaphoric into the everyday and
taken-for-granted). These observations derived from international trends and geograph-
ical literatures relate to the local specificity of our case example.
Second, from a personal perspective, the packaging and myth-making referred to by
Holcomb (1993) became apparent to the first author in mid-1996. With a history of two
previous hospitalisations, Robin's preschool son came running to him after sustaining
a minor injury, saying "I think my leg is broken. I need to go to the Starship where the
robot is." Four year old Liam's exhortation contained no mention of doctors, medicine,
or hospitals. For him, sudden pain implied a need to visit the Starship, and this
perceived need triggered memories of 'placial icons' (Hopkins, 1990) which at the
hospital include a robot effigy in the Radiology Department. It thus appeared that
the Starship was a metaphor at work, inviting consumption and effectively linking
health and place.
Third, our decision to focus on a children's hospital stems from a claim by John Short
(1989) that our cities are generally unresponsive to the needs of children. The recent
opening of the Starship presents an opportunity to initially assess the extent to which the
hospital, in a tight fiscal environment, has been able to respond effectively to children's
needs. In New Zealand, child health has become an important political issue especially
as there has been growing concern that the gains in child health through the middle years
of the century are not being sustained (Barnett and Ford, 1991). To a large extent
increased poverty and a legacy of inadequate resourcing of child health services has
contributed to a picture of child health in New Zealand which compares unfavourably
with the rest of the developed world (AAHB, 1990). Children have received less than their
'fair share' of health expenditure and have frequently received care in quite unsuitable old
and rundown facilities (Board of Health, 1982). Indeed, until the opening of the Starship,
even in metropolitan areas with large paediatric departments, children continued to be
admitted to adult wards in spite of the fact that authoritative statements on the care of
children in hospital considered this practice undesirable (Central Health Services
Council, 1962; Committee on Child Health Services, 1976). Thus, in considering aTo boldly go? 203
new health care setting for children, wc contribute to redressing the limited place for
children in geography (James, 1990), a gap thai has only recently been addressed in
a sustained manner by Gill Valentine (1996; 1997). Although other recent work has
addressed public health implications for urban children (Davis and Jones, 1996;
Hcrtzman and Wicns, 1996), the relations between children's health and experience
of place have yet to be considered from a service provision and cultural landscape
perspective.
In light of the foregoing discussion, in our paper we have two aims: (1) to examine
changes in the provision and marketing of hospital services, and to discuss why such
marketing has been necessary; and (2) to examine the use of symbols and metaphor
in the marketing process and to gauge how these have been important in affecting both
the financial viability of the Starship Hospital and the qualities of its therapeutic
environment. To this end the paper is organised into five substantive sections. In order
to provide a political-economy context for the study, we begin by reviewing the
increasingly consumption-oriented nature of health care services. We consider how
this situation has resulted in competition and changes in the organisation and market-
ing of hospital care within the private and public sectors. Wc then focus on the qualities
of symbol and metaphor in the marketing process and their contribution to the con-
struction of particular therapeutic landscapes which are used to attract sponsorship
and patients. In the third substantive part of the paper we examine the world into
which the Starship was launched and how continuing fiscal problems in the New
Zealand hospital sector have shaped the corporate strategies of the hospital and the
character of the therapeutic environment which has developed. In the final two sections
wc reflect on our findings and consider further research directions.
2 Competition in the provision and marketing of hospital services
A common feature of health reforms in Western nations has been an introduction of
market-based ideologies advanced by 'new right' politics and resulting in an infusion of
competitive practices and greater levels of advertising (Robinson and Le Grand, 1993).
Whereas most commentators have been preoccupied with analysing explicit policies
and their outcomes at regional and national scales, our present interest lies in the more
subtle ways in which the means and styles of health care provision have changed under
the 'market-led' transformation of the health sector and of society at large. One outcome
of this transformation has been the (reconstruction of health and health care as,
respectively, a commodity and product, in tandem with more conventional constructions
as a quality and service (Hay, 1989). In the course of this transformation, users of health
care services have been refashioned as 'consumers'and, we might argue, the health system
itself has become part of what Robert Sack (1992) describes as "the consumer's world"
(Kearns and Barnett, 1997).
Within the hospital sector this market-led transformation became evident in the
1980s and has accelerated in the 1990s. Hospital systems have been increasingly
privatised. This observation is evident in such trends as the increased rationing of public
care and the downsizing and closure of public hospitals (Succi et al, 1997), the growth of
for-profit involvement in health care (Montague Brown, 1996a; Salmon, 1985; 1995) and,
more recently, the emergence of large-scale managed care organisations which have
resulted from a raft of mergers and consolidations of existing providers (Montague
Brown, 1996b; Corrigan et al, 1997).
To a large extent, changes in the organisation and financial viability of hospitals
can be attributed to changing sources of capital. Historically, capital financing of
hospitals came from a variety of sources including philanthropy, debt financing (loans),
government grants, or equity financing (that is, sale of stocks). The main factor204 R A Kearns, J R Barnett
determining access to these different finance sources has been the type of ownership, but
increasingly this is less true as the boundary between private and public sectors has
become blurred. Nevertheless, traditionally public and nonprofit hospitals have tended to
rely on capital from philanthropic and government sources, whereas equity financing has
usually only been an option available to for-profit institutions (Bohland and Knox, 1989).
During the 1970s and 1980s national economic and political restructuring fundamen-
tally altered the availability of low-cost capital for hospitals. In New Zealand, for
instance, state fiscal crises during the 1980s saw the end of state subsidies for patient
care in the private (nonprofit) sector (Barnett and Barnett, 1989). Similarly, in the United
States, the advent of diagnosis-related groups (DRGs) had the effect of constraining the
fiscal capacity of nonprofit hospitals and hastened rates of closure (Williams et al, 1992).
In some respects DRGs also opened the way for the emergence of the for-profit sector,
which is now the fastest growing source of care in many states (Needleman et al, 1997).
Ready access to external capital provides for-profit companies with the resources to
acquire hospital assets outright and where the boards of financially struggling nonprofit
hospitals have been reluctant to walk away from such community institutions by selling
all assets, compromise joint ventures have often resulted (Hollis, 1997). In contrast to the
ready availability of capital fuelling private-sector growth, most public institutions have
been faced with a legacy of state fiscal crises and declines in expenditure.
As public hospitals have come to face increasing difficulty in receiving large enough
government grants, or as proprietary and nonprofit hospitals have had difficulty in
generating sufficient cash flows from patient care revenues to support their current level
of operations, they have had to develop new organisational strategies in search of
potential sources of financing (Naidu, 1992; Parry and Parry, 1992). Many hospitals
have sought to boost cash flow by changing or improving the focus of their patient care
activities, by marketing themselves more aggressively, or by attempting to bolster their
cash flow by diversifying into other lines of business (Eastaugh, 1992; Smith et al, 1995a),
a theme we will explore with reference to Auckland's Starship.
These trends have been particularly evident among for-profit hospitals, but are also
increasingly characteristic of public-sector institutions, particularly where, as in New
Zealand, they have been corporatised (that is, restructured into commercial profit-
seeking entities) (Kelsey, 1995). In the United States, for example, for-profit hospitals
have engaged in aggressive marketing campaigns to attract patients (Kuttner, 1996a;
1996b). Sue Greer and Paul Greenbaum (1992), attribute the rise of adolescent psy-
chiatric hospital admissions to the use of fear-based advertising by private psychiatric
hospitals intent on increasing their market share. Such trends have resulted from an
overabundance of hospital beds as well as continued pressure on hospital executives to
maintain and increase profit levels for shareholders. Not surprisingly, competitive
health care policies which have propelled corporatisation in the US health care sector
have had little impact on prices given that hospital competition was driven by the
provider rather than the patients (Salmon, 1995). Indeed, as providers engaged in
expensive 'technology wars' (designed to attract doctors and patients) and pursued
higher bottom-line returns, no improved efficiency in the market resulted as the
rhetoric had promised. Numerous studies in the 1980s revealed that costs per inpatient
day for for-profit hospitals were higher than for other hospital types and that these
costs peaked in more competitive environments where the density of hospitals was greatest
(Robinson and Luft, 1987; 1988; White, 1987). It has only been with the advent of managed
care that circumstances have changed. Purchasers are now increasingly bypassing
insurance companies to contract directly with preselected large-scale managed care
organisations and such trends at last appear to be placing downward pressure on costs
(Zwanziger et al, 1994).To boldly go? 205
Nonprofit hospitals, too, have developed their own coping strategies with respect to
fiscal stress and increased financial risk. In some respects fiscal cuts have meant that
nonprofit hospitals have forced emulation of their for-profit counterparts in marketing,
patient selection, and labour relations tactics. As Montague Brown (1996a* page 13) has
commented, "the voluntary not-for-profit enterprise we think of as Main Street and
Community Values has changed to one that is Wall Street and Commercial Values"
Nonprofit hospitals have responded to increased financial risk by increasing prices for
privately insured patients (Friedman and Farley, 1995), by being more selective about
patient admission (Mann et al, 1995), and by ensuring increased internal efficiencies.
They have also increasingly turned to nonoperating sources of finance, such as income
from investments and marketing themselves to increase their income from philanthropic
donations (Smith et al, 1995a). For instance, the Royal Alexandra Hospital for Children
in Westmead, a suburb of Sydney, has actively courted corporate sponsors for dona-
tions. In return, it has raised the sponsors'community profiles by using their names (for
example, Woolworths, Shell Oil) to identify a landscaped courtyard and operating
theatre respectively (L Brown, personal communication), thus contributing to new
geographies of corporate philanthropy (Hurd et al, 1998), In what seems to be a
return to the nineteenth century, philanthropy is again becoming an important source
of capital (Beatrice, 1993; Glaser, 1992).
Within the public sector similar trends are apparent. Faced with serious fiscal
cutbacks or, at worst, closure, many public institutions arc now seriously marketing
themselves to attract paying patients as a way of generating additional income. In
Canada, for instance, Johnston (1992) reports that the St Boniface Hospital in Winnipeg
has opened an in-house pizza franchise. Other Canadian hospitals, such as the small
(twenty-five bed) Cardston Municipal Hospital in Alberta have attempted to resist
closure by marketing themselves in the United States. Despite opposition from the
Alberta Provincial Government, Cardston was successful in attracting overweight
Americans into its gastroplasty (surgical weight reduction) programme (Williams,
1995). Philanthropy is also becoming a more important source of capital for public
hospitals either to help with day-to-day operating expenses or, more commonly, in
response to fundraising efforts associated with particular developments (Smith et al,
1995b). Children's hospitals, in particular, have been host to such developments and, as
Robert Evans has commented, "the most compelling reason for building and main-
taining children's hospitals is their ability to attract donations" (Morgan and Cohen,
1993, page 1775). This view has relevance to the case study in question. Although a
nation's sole teaching and tertiary care paediatric hospital is certainly in no need of
competing for patients, it nevertheless needs to compete for the donated dollar. Given
an era in which 'core services' are defined and provided(1) (NACCHDSS, 1996), addi-
tional health care developments must be funded from philanthropic sources. Many
worthy health care causes regularly seek donations, so it is arguably important that
an organisation regards its potential benefactors as consumers of a branded image.
Thus the strategic choice by a hospital administration of a catchy logo and name, and
the development of a building with high imageability (Lynch, 1960) hypothetically
encourages potential benefactors to become actual patrons and consumers of the
charity in question.
(1)
In sketching this brief account of the health reforms in New Zealand, we recognise that we are
using language o/the reforms to speak about the reforms. In so doing, our use of terms such as
'consumer' and 'core services' risks reproducing rather than interrogating such metaphors. How-
ever, for the sake of maintaining a focus on the chosen metaphor in the paper, a fuller discussion
of these metaphors will be reserved for another occasion.206 R A Kearns, J R Barnett
In attracting corporate funding, nonprofit and public institutions must increasingly
sell themselves not only to their sponsors, but also to the patients who will use the
facilities in question. Therefore, it is important to understand how public and private
agencies strive to 'sell' the image of a particular place so as to make it attractive. Making
places attractive involves the conscious manipulation of images, that is adapting the
'product' to be more desirable to the 'market'. Conventionally, geographers have viewed
the consumption of health care services largely in terms of utilisation behaviour (see, for
example, Joseph and Phillips, 1984). Alternatively, the emphasis in the geography of
health care consumption can be shifted from behaviour to culture. In the remainder of
the paper, we build on Wilbert Gesler's exhortation that we "read or decode healing
environments for their symbolic meaning" (1991, page 182). Although geographers are
increasingly interested in the relations between place and consumption, health care is an
area neglected by recent surveys (for example, Jackson and Thrift, 1995). Incorporating
health care contexts into the intersection of urban geography and cultural studies is
overdue as new styles of service provision have taken highly visible and symbol-laden
forms in the built environment (Kearns and Barnett, 1992).
3 Symbol and metaphor in marketing therapeutic landscapes
An incorporation of health care into the meeting of urban and cultural studies requires
that we advance our understanding of the deployment of symbol and metaphor in
places of health care provision. Symbols are structures of meaning imbued with power
which can be used to control environments (Cosgrove, 1987) such as in the case of
security cameras or 'no entry' signs. Symbols can also be employed in the interests of
healing (Hagey, 1984) with the red cross, for instance, being widely regarded as
representing the availability of nonpartisan medical care. However, symbols can be
ambiguous. The traditional white coat of the physician, for instance, might convey
confidence, hope, and professionalism; yet this symbol can also connote oppressive
patriarchal characteristics (Blumhagen, 1979). The buildings that house medical activ-
ities can be equally ambivalent elements of the symbolic landscape. A private medical
clinic may represent a place of accessible, friendly, and effective health care for those
with health insurance, but to members of an uninsured family, the same clinic might
symbolise something foreign and inaccessible (Kearns and Barnett, 1997). The symbolic
content of a landscape is thus paradoxically both fixed (by means of the ideology that
shaped its tangible form) and varied (according to the 'ways of seeing' adopted by
different people) (Berger, 1972).
Linguistic symbols can take the form of metaphors which involve the application of
a word or idea to something to which it is imaginatively, but not literally, applicable
(Kearns, 1997). In health studies, the word or idea has frequently been disease itself,
with much orthodox western (bio)medicine founded on metaphors such as the body as
machine (Kirmayer, 1988). As Susan Sontag's (1978) classic study indicated, cancer has
at various times stood for corruption, catastrophe, and evil.(2) More recently, we see
AIDS as metaphor, with associations popularly made between this disease and societal
breakdown (Michael Brown, 1995; Gilman, 1988). The use of metaphor thus represents
a discursive coping strategy deployed strategically by communities to construct under-
standing of their changing places and changing place-in-the-world (Kearns, 1997). Such
strategic deployment can occur informally within a community (see Kearns, 1998), or
through a more explicit marketing plan in which the place, as well as the services,
becomes the commodity 'sold' to professionals, patients, and benefactors.
(2)por instance, groups oppositional to the ruling military dictatorship were labelled 'Chile's
cancer' (Frazier and Scarpaci, 1998).To boldly go? 207
Perhaps the most pervasive metaphor currently deployed in public policy discourses
in contemporary New Zealand is 'the market' itself. This metaphor connotes an image of
knowledgeable actors negotiating prices of goods and services (Le Heron and Pawson,
1996a), The market metaphor has now permeated a number of state service sectors
including public housing (Murphy and Kearns, 1994), education (Berg and Roche, 1997),
and health care (Barnett and Kearns, 1996). With respect to health care, the use of the
market metaphor has prompted people to experience "one kind of thing [caring, curing]
in terms of another [a commodified exchange]" (Lakoffand Johnson, 1980, page 5).
Metaphor has long been applied informally to particular places associated with
health care activities. In New Zealand, for instance, children frequently refer to the
school dental clinic as 'the murder house'. Such clinics are not literally sites of homicidal
activity, but rather their description as such within juvenile vernacular powerfully
conveys commonly understood (mis)perceptions and distressing experiences. So too,
contrived names such as the 'Starship' suggest imaginary rather than literal expectations.
Both usages are examples of what George LakofT and Mark Johnson (1980, page 29)
describe as "container metaphors", which are applied to bounded areas in which certain
properties are to be found here but not there. Within bounded areas such as clinics and
spas, metaphors mediate between the biophysical and sociocultural worlds and, in the
words of Klcinman (1973, page 207), "healing occurs along a symbolic pathway of words,
feelings, values, expectations, beliefs... which connect events and forms with affective
and physiological processes". Thus, whether through popular reputation (Gesler, 1998) or
explicit marketing (Geores, 1998), potentially health-promoting sites become concep-
tualised as containers. These sites represent focal centres for healing experiences and
reputations found in, but not out of, place (Kearns, 1997).
Within the consumer's world of health, metaphor is increasingly being deployed
through explicit marketing to represent health as a quality, when in fact it is being
commociified through the pricing and 'packaging' of health care. In New Zealand, for
example, many general practitioners are rebranding themselves as family doctors, a label
resonant with ideas of attentiveness to relationships, and caring as well as curing.
Similarly, commercially oriented yet publicly owned Crown Health Enterprises (CHEs)
have given themselves names that are less descriptive of locality and jurisdiction (as was the
case with Area Health Boards) and more euphemistically indicative of quality. *A+ Health'
and 'Good Health Wanganui', for instance, are simultaneously administrative names and
corporate brands that metaphorically accentuate the positively therapeutic, and seek to
mask less desirable associations with illness and commerce.(3) Thus, when linked to the
marketing of health, metaphors are potentially no more than semantic veneers, provid-
ing a linguistic layer covering the reality of commercial transactions.
Our concern with links between marketing and metaphor is situated within a growing
interest in therapeutic landscapes. This idea brought into health geography by Wilbert
Gesler applies perspectives from cultural geography to explore "environmental, individ-
ual and societal factors that come together in the healing process in both traditional and
non-traditional landscapes" (1992, page 735). These 'nontraditional' landscapes are
identified as including "situations in which healing might take place, such as a physician's
modern office... or a hospital ward" (1992, page 735). This catholic application of
'landscape', a term widely associated with expansive and naturalistic settings, self-
consciously draws upon a melange of humanist, materialist, and poststructuralist ideas
that reconstitute places as, respectively, sites of shared symbolic meaning (Relph, 1976),
(3)
'Good Health' seems an ironic descriptor that allies itself with the positive health model of the
Ottawa Charter for Health Promotion, while also suggesting an utterance ordinarily reserved for
social drinking occasions.208 R A Kearns, J R Barnett
arenas of social control (Cosgrove, 1987), or texts to be cocreated by the reader (Duncan
and Duncan, 1988). Although Gesler has focused his research on places with established
reputations for healing (1993; 1996a; 1998), Martha Geores has usefully extended the
concept by arguing that entrepreneurs can self-consciously engage in "steering placemak-
ing activities towards the (therapeutic landscape) metaphor" (1998, page 36). We build on
her concern for placemaking and the selling of a health care site in considering how an
otherwise prosaically named hospital has been branded, marketed, and metaphorically
deinstitutionalised through the process of naming.
However, it is not just naming that can metaphorically invoke therapeutic or non-
therapeutic properties in a built environment. As Gesler (forthcoming) has pointed
out, the place-specific language used is central to the construction of health and
healing contexts. In hospitals, for instance, the 'words in wards' can create senses of
place(lessness) no less powerfully than the sterile disinfected smellscapes (Porteous,
1985) and soundscapes (Smith, 1994) of echoing corridors (see also Rodaway, 1994).
Indeed, the very design of a health care facility can convey powerful messages such as
what type of patient is welcome, and how relaxed they are intended to feel. These
statements that might be implicit in the interior design and furniture can be made explicit
in the hands of entrepreneurs seeking to promote the hospital to a wider audience.
Hospitals are conventionally places of medicalised care that tend to be highly
functional elements in the urban landscape. They have generally only advertised them-
selves inadvertently through location (for example, elevated, or central city, sites),
or through their form (for example, large size relative to surrounding buildings).(4)
Consonant with the box-like form of the modernist skyscraper, the built form of
many hospitals is austere and angular, their interiors potentially generating feelings
of placelessness (Relph, 1987). However, influenced by the postmodern turn in archi-
tecture and a concern for branding, some private clinics now proclaim their presence
through "architectural imagineering" (Mills, 1993, page 152). In New Zealand, such
'imagineering' has been much less evident in hospitals, few of which have been built
within the era of postmodern architecture. Indeed, many hospitals were dedicated as
war memorials or in homage to distant members of British royalty. In the case of the
Starship, however, such an orientation to the past is replaced by a naming that aims to
be novel, marketable, and suggestive of a journey beyond the particularities of time
and place.(5)
In summary, the therapeutic landscape idea reminds us that the urban environment
comprises more than composite elements of tangible built form. Rather it is an inter-
pretable text which contributes to meaning and well-being in the broader canvas of
urban life. As Caroline Mills puts it, "places encapsulate and communicate identity"
(1993, page 150). Metaphor can be a linguistic vector for this transmission of identity
and can be materialised in the naming of buildings and places. Although smell and
sound contribute to place, the main cues for this transmission of identity are visual
and are to be found both tangibly in the built environment and reproduced in printed
representations of products and services. In the following section we consider the case
of the Starship and how this particular children's hospital has marketed itself as a
'therapeutic place' within an increasingly hostile fiscal environment. We begin, first, by
(4)
Auckland Hospital, adjacent to the Starship, inadvertently (and obscurely) advertises itself
through the leasing of rooftop advertising space to the Sharp electronics corporation. This has
led some to nickname the hospital the Sharp Factory.
(5)
In the wake of the September 1997 death of Diana, Princess of Wales, there was a short-lived
campaign led by prominent Auckland journalist Pat Booth to have the Starship renamed 'Princess
Diana Memorial Hospital'. Subsequent letters to the press strongly indicated that Starship was
now the recognisable name for the children's hospital.To boldly go? 2(W
outlining briefly the political and economic context of hospital funding in New Zealand
before turning to a more detailed examination of the characteristics and marketing
strategies of the Starship itself.
4 Into hostile fiscal space: The world of the Stnrship
4.1 Building the Stnrship
"This building marks a major shift in thinking about how this nation hospitalises
our children." (Land, 1992)
The (yet unnamed) Starship was conceived as a facility to replace the ageing Princess
Mary Hospital in central Auckland, built in 1942 as an annex for an expected influx of
war-wounded. In the post-war era, children were moved into Princess Mary Hospital
and remained as patients amid deteriorating conditions. A new facility for children was
first planned by the Auckland Hospital Board in I960 (AAHB, 1991). However, early
plans were regarded as too grand and the project stalled. Inaction led staff at Princess
Mary to form the New Children's Hospital Trust in 1981 with the purpose of lobbying for
the facility. A petition was organised the same year by Dr Paul White, a paediatrician, and
50000 signatures were presented to Parliament, establishing a precedent for a high
level of public mobilisation in the cause of the hospital and child health. This pressure
propelled the planning process (NZCD, 1992). Development of the hospital spanned
the transition from the medically oriented Auckland Hospital Board to the more
health-focused Area Health Board in 1989 and, more latterly, to the more market-
driven and consumer-driven CHE, A+ Auckland Healthcare Limited, in 1993. During
the intervening years there was considerable debate concerning the merits of this 958
room, 185 bed hospital, described by architects Stephenson and Turner Ltd as the most
complex building planned in New Zealand. At a cost of NZ$79 million, it was also
one of the most expensive. An editorial in the major New Zealand daily newspaper at
the time of its naming proclaimed that
"the new Auckland children's hospital is a most expensive, overcapitalised institu-
tion ... for all its modern styling [it] is a relic of a time when pressure, not prudence,
ruled public spending and new construction was always more easily promoted than
better use of facilities" (New Zealand Herald 1992b).
The hospital was built amid much controversy and was maligned by key spokes-
people. It was labelled in 1989 by the Commissioners of the Area Health Board as a
"bad decision" (New Zealand Herald 1989). Notwithstanding such feeling arising from
the fiscal and political history of Auckland's hospital sector, the Starship was completed
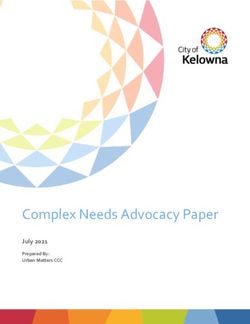
in November 1991 (see figure 1, over). It was built adjacent to the main acute Auckland
Hospital and former Princess Mary site, covers 22000 square metres, and is eight
storeys high. In 1996, the hospital had 494 staff supported by 200 volunteers who dealt
with 16 480 admissions, 35 838 outpatients visits, and over 26 000 visits to the Emergency
Department (Starship Childrens' Health, 1996). In contrast to the minimalist and
functional designs typical of other modernist New Zealand hospitals, an effort was
made by the designers to create a distinctive postmodern structure as well as a space-
efficient, yet child-friendly, building (Vernon, 1988). According to the architect, "the
bending of an otherwise rectangular plan into a curve successfully avoids the typically
long, straight corridors of an institutional building" (Land, 1992). This move repre-
sented a break from the customary use of efficiency-driven calculations based on bed
numbers, a practice that had prevailed at the time when the adjacent box-like Auckland
Hospital was designed by the same architectural firm. The award-winning design of the
Starship is characterised by pastel colours, the use of all-wool carpets throughout the
ward and waiting areas, and children's art work on the walls. In addition to its curved210 R A Kearns, J R Barnett
Figure 1. Starship Hospital viewed from the adjacent Auckland General Hospital (photography
by R Kearns).
lines, other distinctive architectural features include a large entrance atrium, a glassed
roof to admit natural light and, reflecting its eventual name, "rocket-like lifts in various
colours taking off and landing" (New Zealand Herald 1991).
4.2 A hostile fiscal environment
The Starship was launched into a hostile fiscal environment. Two years before the
hospital was opened the elected representatives of the Auckland Area Health Board
(AAHB) had been sacked by the Minister of Health, the Honourable Helen Clark,
and replaced by a government-appointed commissioner, prominent businessman
Harold Titter. By the end of the 1989-90 financial year, the AAHB had overspent
its budget by $47 million, a figure that was later revised to $70 million once cumula-
tive overspending to March 1990 had been taken into account (Drage, 1993). Auckland
was by no means unique in this respect as its precarious financial position was typical
of other large metropolitan area health boards in New Zealand at the end of the
1980s.
To a large extent the pattern of hospital funding in the latter 1980s reflected the
cumulative result of a long period of underfunding of hospital services in the larger
cities. Indeed the pattern could be traced back to the initial system of local funding of
hospital care which persisted in various forms until 1957. Given New Zealand's trends
of economic development at the end of the nineteenth century, the system of local
funding inevitably meant that more affluent rural areas ended up spending more per
capita on hospital care than was the case in the larger cities (Barnett et al, 1980).
Despite the advent of central government funding in 1938 and the final phasing out
of local funding in 1957, the incremental allocation system which followed simply
served to reinforce historical fiscal inequalities. Attempts to rationalise the administrationlb boldly go? 2tt
of hospital care by reducing the number of hospital boards and the implementation of
population-based funding in 1983 provided the opportunity to reduce geographic dis-
parities in hospital financing in favour of areas of urban disadvantage. However, progress
towards greater equity remained slow. Unlike the situation in Britain at the time of the
implementation of the Resource Allocation Working Party's (RAWP) recommendations
(DHSS, 1976; Eyles and Woods, 1983), in New Zealand there was no commitment for
the provision of extra money to underfunded boards and the expectation was that
funds for bringing underfunded boards, such as Auckland, to equity would be derived
from reduced allocations to overfunded boards (Burnett, 1984). However, such a recipe
was inevitably one that would lead to intense political conflict with the result that the
closure of rural hospitals in favour of the upgrading of urban ones has been painfully
slow (Prosser et al, 1996).
Although the reforms of the 1980s produced certain gains, lack of service integra-
tion, continued long waiting lists, and the drive for greater efficiency resulted in further
pressures for reform. These pressures initially began under the Labour government
which introduced elements of the *new public management* into the public sector
(Boston ct al, 1996), but widespread hospital restructuring did not occur until 1993,
after the new right National government was well established in office. The changes
introduced in 1993 largely reflected the new right's adoption of economic rationalist
propositions that markets must be promoted not only to advance economic efficiency
but also to maximise the economic and political freedom of individuals to pursue their
own goals (Malcolm Brown, 1996). This contention took the form of the introduction of
internal markets in the hospital system which was now characterised by a separation of
funders [Regional Health Authorities (RHAs)] and providers, both public and private.
Public hospitals were renamed Crown Health Enterprises and were, in essence, publicly
owned companies registered under the 1993 Companies Act. To some commentators
these initial moves to corporatisc hospitals were just the first step in a political agenda
which would eventually involve full privatisation as had happened in the case of many
other former state activities (see, for example, Kelsey, 1995).
Whatever the main aim of the 1993 reforms, their effect was to introduce more
competitive processes into the hospital system, to foster further integration of services
(as primary care was now included under the purchasing orbit of RHAs) and to foster
greater accountability by devolving 'control' from the centre to the regions. In reality,
however, central control remained given that locally elected area health boards had
been abolished and replaced by nonelected government-appointed chief executive
officers (CEOs), many of whom were appointed from outside the health sector and
who were directly responsible to the newly established Minister of Crown Health
Enterprise (Barnett and Malcolm, 1997). One of the key assumptions underlying this
change in governance was that it would avoid the perverse incentives which had
prevented the attainment of greater efficiency among area health boards. As Fougere
(1997) has noted, successive governments had argued that the problem was not one of
inadequate resources, but an inability of the hospital sector to rationalise the use of its
existing resources. Crucial to this analysis was the argument that area health boards,
and hospital boards before them, had been 'captured' by community and provider
interests. The new RHAs were designed to avoid such capture by holding communities
and providers at arm's length, dealing with both by means of the formal contracting
process. By cutting direct ties, central government policymakers hoped to ensure that
purchasers would be preeminently their agents and would achieve a more rational and
efficient allocation of resources at the regional level.212 R A Kearns, J R Barnett
4.2.1 CHE financial strategies
An important part of the reforms was the reconstitution of public hospitals into CHEs
which were to be run along commercial lines. This philosophy was reflected in the first
reading of the Health and Disability Services Bill 1992 which stated that one of the
principal objectives of CHEs was to be as "profitable and efficient as comparative
businesses that are not owned by the Crown" (Health and Disability Services Bill, first
reading, 1992). Although the word 'profit' was eventually removed with the passing of
the bill, this philosophy nevertheless still pervades CHE boards and other corporatised
parts of the public sector (Murphy and Kearns, 1994).^
The basis for the establishment of CHEs is that they will be service providers
responding to purchaser initiatives. However, in the absence of other purchasers of
health services, CHEs have been forced to negotiate only with RHAs, which essentially
are monopoly purchasers. Conversely, given the limited involvement of private providers
in the contracting process, RHAs, in turn, have been forced to negotiate contracts with
monopoly providers. In some respects the lack of competition, accentuated by New
Zealand's small population (Barnett and Barnett, 1997), has compromised the ability of
the reforms to satisfy their original objectives. The lack of competition has also led to a
situation in which perverse incentives continue, given the continuing pattern of CHE
deficits and the state continuing to underwrite CHE financial losses.
In the financial year ending March 31, 1996, despite improvements in management,
information systems, contracting arrangements, and performance monitoring, and also
despite the additional injection of $200 million into the hospital sector since 1993 - 94,
21 of the 23 CHEs were in financial deficit (Office of the Controller and Auditor-
General, 1997). To a large extent these trends reflect the gap between the pricing
structure of RHA contracts and the actual cost of delivering services. Although an
extra $200 million has been paid to CHEs since 1993-94, CHE costs increased by
$267 million (CCMAU, 1996). Clearly, a full coverage of their costs represents a
significant challenge to CHEs which, for the most part, have few options. These
options include: identifying and capturing other efficiency gains; renegotiating the
prices in contracts with RHAs; developing other sources of revenue; or negotiating
to withdraw from providing services altogether (services which, in the long term, will
cost more to provide than what the RHA or other purchasers are willing to pay).
All of the above are difficult options. Improving efficiency, for example, may not
always be possible given the improvements which had already occurred under the area
health board structure. Renegotiating contracts will also be difficult. Although RHAs
are required to pay CHEs a price which is financially sustainable over the medium
term, CHEs have generally been unable to reduce the cost of providing services to the
level specified in RHA contracts. Given their difficult position in managing capped
budgets and balancing the demands of the now 'seamless' primary and secondary
sectors for contracts, RHAs, however, have not been accommodating of CHE wishes.
The fact that RHAs have been relatively successful in managing these divergent
pressures is reflected in the fact that at the end of the 1995 - 96 financial year although
three of the four RHAs themselves were in deficit, their total (accumulated) deficit
amounted to only $1.19 million versus $560 million for the 23 CHEs (Office of the
Controller and Auditor-General, 1997; Ministry of Health, 1997). CHEs have also
sought to reduce their deficits by closing or downgrading peripheral rural hospitals.
Such strategies have led to considerable political unrest. However, such unrest has not
(6)
As a reflection on the removal of their statutory obligation to return dividends to their
shareholding Ministers, CHEs were renamed Hospital and Health Services (HHSs) in 1998.l b boldly go? 213
stopped the trend. In 1997, Healthcare Otago, for example, sought to completely withdraw
from the provision of rural hospital services (GOHDC, 1997).
Last, CMEs have the option of securing other sources of funding, In the "Statement
of Shareholders* expectations of Crown Health Enterprises" of the Crown Company
Monitoring Advisory Unit (CCMAU) report to the incoming Minister of Health
(1996) it is stated that
"We expect CHEs to exhaust other sources of finance before approaching the share-
holder (that is, the state and taxpayers) for additional equity" (CCMAU, 1996,
section 3.2.1.1).
In section 3.2.4 it is further stated that
"We wish CHEs to access private sector capital where possible. This includes
considering proposals to lease facilities or equipment as well as borrowing from
the private sector. Such proposals should be assessed on a commercial basis...
Accordingly the Crown will not provide guarantees of any sort for CHE borrowings."
In practice the latter statement is not strictly true as the Crown owns the CHEs.
Persistent losses require that the Crown assist CHEs financially for they can hardly
be allowed to go bankrupt. As a result the Crown has made frequent capital contribu-
tions to restore the financial base of CHEs, but such infusions of capital have not been
sufficient to prevent financial deficits. Currently CHEs have the option of borrowing
from the private sector to cover deficits or, more commonly, arc funding deficits by
borrowing from the state-owned Residual Health Management Unit (RHMU). How-
ever, both forms of borrowing carry interest costs. Nevertheless the state is still financing
such deficits and to the extent that there is 'poor performance* by a CHE, deficit support
has a perverse effect as it is inevitably rewarding poorer performers with more money.
This has caused resentment among some CHEs. For instance, in Auckland, 'good
performers' included Counties Manakau Health Ltd (South Auckland Health), the
only Auckland CHE to make a small 'profit' in 1995-96, and this company feels
that they have not been adequately rewarded for their improved performance.
To date, in addition to borrowing from public and private sources, accessing extra
capital has taken various forms. Some CHEs have increasingly tendered out non-
clinical services in order to make financial savings. However, such moves are hardly
new and are part of a long-term trend (Stubbs and Barnett, 1992). Other CHEs, such as
Capital Coast Health (Wellington) and Good Health Wanganui, have made plans to
tender out clinical services, whereas others, such as Healthcare Otago (Dunedin) have
aligned themselves with private providers in a bid to win RHA contracts. Healthcare
Otago, for instance, joined forces with the Southern Cardiothoracic Institute, a private
surgical company, in an unsuccessful bid for a major contract to provide cardiac
surgery in the South Island (Christchurch Press 1997a). Last, other CHEs, such as A+
Auckland Healthcare, have increasingly attempted to court private capital in the form
of encouraging corporate donations from major banks and companies and have, in
the case of the Starship, offered an in-hospital concession to the major restaurant
chain, McDonald's (see Kearns and Barnett, 1998).
Considerable geographic variation exists in the economic health of CHEs. The fact
that CHEs began life with varying degrees of financial hardship has its origins in
historical patterns of funding and the constraints imposed on former area health
boards. Broadly speaking the pressures faced by area health boards and how these
pressures were managed have led to three broad groups of CHEs: the inadequately
resourced, the adequately resourced, and the overresourced (CCMAU, 1996). A+
Auckland Healthcare Ltd—the CHE which includes four major acute care hospitals,
including the Starship—belongs to the first category. In 1995-96 the CHE's net
operating deficit was $28.9 million or 7.72% revenue for that year (Office of the214 R A Kearns, J R Barnett
Controller and Auditor-General, 1996). This represented an increase of 0.29% on that of
the previous year which was in contrast to an average decline of 6.06% for all CHEs.
Most significant was the fact that the Auckland CHE had the largest absolute operating
deficit and its debt-equity ratio was the third largest in the country. Most other
metropolitan CHEs had above-average debt-equity ratios. It would appear that despite
almost two decades of reform, not much has changed. Historical inequities continue. In
the meantime, in the words of the 1996 CCMAU profile of the Auckland CHE,
"solvency is maintained via a mix of shareholder equity and debit financing from the
government... and the business continues to operate on the basis of a commitment of
future support from the shareholders" (CCMAU, 1996, appendix 4.8). It is in the context
of such trends that the marketing strategies of the Starship hospital must be interpreted.
4.3 Launching the Starship
"Forgive the loopy title...and hope that, whatever heavenly horrors 'The Starship'
may hold for children admitted with life-threatening conditions, the tag might
excite corporate sponsorship". (New Zealand Herald 1992b)
The full name 'Starship Children's Hospital of the South Pacific' which was officially
given to the hospital in April 1992 astutely captured a combination of connotations:
familiarity and otherworldliness. The name was formulated by Bob Harvey, currently
mayor of Waitakere City in western Auckland, but then regarded as a "marketing guru
employed by neighbouring Auckland Hospital as a consultant" (New Zealand Herald
1992a). In his words, "Having children of my own, I was aware of the trepidation many
kids felt towards entering hospital. The name was a way to ease that fear by presenting
the hospital as something I believed kids were interested in/excited by" (B Harvey,
personal communication). This quest to normalise the hospital was, at the outset, laced
with a strong concern for selling the place. According to Harvey,
"I approached the Starship project like any other marketing/advertising assignment.
The trick is to come up with a catchy phrase or name that will endear the product
to the customer. In this case the 'customers' were the kids...It was when I was
going up in a lift that I got into conversation with a young... patient. I said to him:
'This is a pretty good place isn't it?' He was looking out of the lift at the time and
replied: 'Its like being inside a spaceship'. For me that was the trigger to go outside
the traditional for a name. The next day, mulling over the spaceship idea while on a
run, I developed 'The Starship'" (B Harvey, personal communication).
In the years since, the normalising potential of the fantasy-laden name continues to be
recognised. According to the Starship's current General Manager:
"The metaphor is a distraction for kids who are the real target. We're keen to normalise
the hospital experience. That's one reason we got McDonald's in here. Psychologists
tell us the biggest fear of children under six is separation, being left alone. By making
the hospital seem familiar to children, we have aimed to reduce children's anxiety"
(G Close, personal communication).
From the outset, there was excitement at the name in terms of its 'sell-ability' and
ultimate potential to be a highly popular and visible part of Auckland's therapeutic
landscape. It was optimistically reported that "the Starship image could put the
hospital on the tourist trail...overseas visitors could soon visit Kelly Tarlton's Under-
water World, the Aotea Centre and the Starship"(7) (New Zealand Herald 1992a).
Indeed, the hospital's business and marketing manager of the time, Roger Bannister,
"confirmed that groups of tourists were already being shown through the hospital,
(7)
These attractions are, respectively, a walk-through aquarium, and the city's recently completed
performing arts centre.To boldly go? 213
although the tours were confined to the atrium area" (New Zealand Herald 1992a).
Such media reports clearly added to inventing* the Starship as a place (Anderson and
Gale, 1992), and cementing its attractiveness to potential sponsors.
The name was confidently applied in signs and advertising without the subtitle
'Children's Hospital' in expectation that there would be rapid public assimilation of
the chosen metaphor. Cultural sensitivity was one rationale behind the name. The
Herald reported on its abbreviation to simply 'Starship', stating that
"Mr Harvey said the word 'hospital' was a definite no-no in the new name because it
had connotations, particularly for Maori and Pacific Islands people, of sickness
and death."
Reference to Auckland was also avoided as the hospital serves a larger area than the
city. The name was chosen "after consultation with staff, the Maori community, and
clinicians", and in avoiding a prosaic name,
"the hospital was following in the footsteps of many overseas children's hospitals
which marketed their product to attract sponsorship... the Starship image and logo
would give sponsors something to which they could relate... most importantly, every
child in the country would come to know the Starship as an exciting place rather than
something of which to be scared" (New Zealand Herald 1992a, emphasis added).
The naming was thus concerned with setting norms for the hospital: the metaphor
potentially had euphemistic content for users, and also connoted a catchy optimism for
sponsors. The allusion to science fiction involved links between the Starship name and
the television (and later film) scries "Star Trek". However, as if to appeal to a younger
generation of popular culture consumers, the lettering and image included in the
original promotional logo for the hospital alludes more to the Star Wars scries of films
(seefigure2). Perhaps significantly, Star Trek is a better-known icon of popular culture to
parents and (now middle-aged) potential donors than to current children, although more
recent representations of 'starships' have saturated youth culture with movies such as 'ET'
and Independence Day'. In all such representations, the emotions evoked by youthful
hospital users are likely to vary from excitement to anxiety, an almost unavoidable
ambivalence given the intrinsically polysemic qualities of metaphor itself (Kearns, 1997).
As a newspaper headline proclaimed at the time of naming "Not Everyone is
Starstruck by the Starship Image" (New Zealand Herald 1992c). Cartoonists (seefigure3,
over) as well as columnists took delight in poking fun at the name:
"A hospital without sickness and death—well not that you talk about, anyway....
Did I say death? Well, feed me to the Daleks. The 'D' word must be banned. No
one will die. They'll be beamed up to the Big Burger King in the sky instead"
(Rudman, 1992).
Figure 2. Allusion to "Star Trek"; the early hospital logo (courtesy of Starship Hospital).You can also read