Tobacco Cessation at CHI St. Alexius Health Bismarck - North ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tobacco Cessation at
CHI St. Alexius Health Bismarck
Development & Impact of a Tobacco
Treatment Program 2012 – 2020
Photo from chistalexiushealth.org
May 2020
Prepared for: Prepared by:
Neil Charvat, Director Sara Richter, MS
Kara Backer, Tobacco Cessation Coordinator Melissa Chapman Haynes, PhD
North Dakota Department of Health, Renée Kidney, PhD, MPH
Tobacco Prevention and Control Program Audrey Hanson, MPH
Professional Data Analysts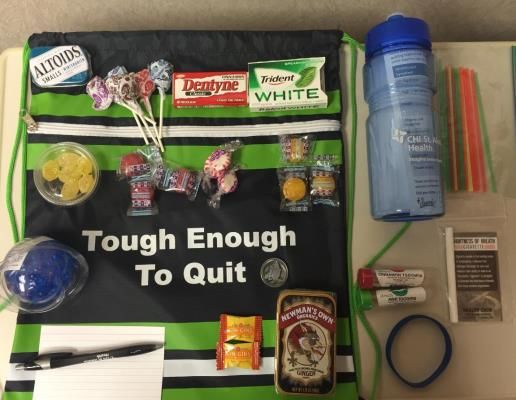
About this Report
Since 2012, the North Dakota Department of Health
(NDDoH) Tobacco Prevention and Control Program (TPCP) Initialisms
has awarded grant funding to aid tobacco cessation AAR: Ask – Advise – Refer
efforts in health systems via the NDQuits Cessation CDC: Centers for Disease Control and
(NDQC) Grant Program. This program was previously Prevention
known as Million Hearts® “S” (Smoking Cessation) Grant.
CMS: Centers for Medicare and Medicaid
Professional Data Analysts (PDA) has evaluated this
Services
program since 2014.
CHI: CHI St. Alexius Health, formerly known
The focus of this program is to advance tobacco treatment as St. Alexius Medical Center
efforts in North Dakota’s health care systems and to
CTTS: Certified Tobacco Treatment
support Comprehensive Tobacco Prevention and Control
Specialists
State Plan goals of promoting quitting among adults and
youth. EHR: Electronic Health Record
ENDS: Electronic Nicotine Delivery System
One health system, CHI St. Alexius Health in Bismarck, has
EVALI: E-cigarette or Vaping Product
been a grant recipient since 2012 and has established a
strong Tobacco Treatment Program (TTP). An in-depth, Use-Associated Lung Injury
exemplar case study into CHI St. Alexius Health’s progress FY: Fiscal Year
with the NDQC Grant Program was conducted to IT: Information Technology
document their extensive history with the grant and to
help identify successes to date. NCTTP: National Certificate of Tobacco
Treatment Practice
Goals of this report NDDoH: North Dakota Department of Health
• Document the activities of one, exemplar NDQC NDC: Nicotine Dependence Conference
grantee - CHI St. Alexius Health
NDQC: NDQuits Cessation Grant Program
• Analyze the reach and impact of CHI St. Alexius NRT: Nicotine Replacement Therapy
Health’s TTP
PDA: Professional Data Analysts
• Assess sustainability successes and opportunities SAMSHA: Substance Abuse and Mental
• Identify future opportunities, particularly for Health Services Administration
expanded cessation coverage with Medicaid TPCP: Tobacco Prevention and Control
Methods Program
TTP: Tobacco Treatment Program
The overall approach to this case study is a modified TTS: Tobacco Treatment Specialists
timeline mapping method. This involves a retrospective
US: United States
examination of the NDQC Program for one grantee,
where their documentation is reviewed to ensure the
resulting timeline and analysis is credible and accurate.
Materials from July 2012 – March 2020 were reviewed
and included in this review. Full details about methods
are in Appendix A.
Professional Data Analysts | May 2020 2
Report Summary
Introduction (p.4)
The NDDoH started funding health systems to do tobacco cessation work in 2012 under the
NDQC Grant. This grant was inspired by the Million Hearts® initiative, which focused on
cardiovascular health through preventive measures like smoking cessation. CHI St. Alexius
Health in Bismarck was one of the first NDQC grantees, building on smoking cessation work
that was already going in their organization.
Timeline (p.7)
The extensive history of CHI St. Alexius Health’s work with the NDQC Grant is described in three
eras:
2012-2014: Starting the NDQC Program. In this era, CHI successfully launched their TTP.
2015-2017: CHI achieved many TTP expansions while facing electronic health record (EHR)
changes and organization contractions.
2018-2020: With an established TTP, CHI increased its focus on education and outreach
while responding to two nation-wide public health crises.
Four significant factors emerged as contributing to their success: considering and treating
tobacco use as a chronic disease, having a dedicated TTP team with a strong leader, forging
strong collaborations, and being persistent and adaptable to organizational changes.
Program Approach (p.14)
The collaborative approach taken by CHI St. Alexius Health’s TTP team is covered in further
detail on page 14, highlighting their grantee partnerships and community engagement
activities.
Reach & Impact (p.15)
In the past five years, the CHI St. Alexius Health TTP team has counseled over 7,500 patients. In
FY19 alone, four Tobacco Treatment Specialists (TTS) counseled 1,500 patients, provided quit
kits and bridge nicotine replacement therapy (NRT) to nearly 550 patients, and referred at least
40 patients to NDQuits, the North Dakota quitline. CHI is one of the larger grantees by patient
volumes. Together in FY19, the 17 NDQC grantees counseled over 13,000 patients in eight
frontier counties, two additional rural counties, five micropolitan counties, and all four
metropolitan counties. As generalizable outcomes data are not available, impact is relayed
through provider testimonies and patient success stories on page 16.
Sustainability (p.17)
Sustainability of the CHI St. Alexius Health TTP was assessed in nine domains. While some
aspects of this grantee’s TTP are quite strong, such as maximizing billing opportunities and
having passionate, trained staff, opportunities exist to further enhance sustainability, most
notably through engaging higher-level leadership.
Future Opportunities (p.18)
One area of future opportunity is the potential reimbursement of cessation services by
Medicaid, as outlined in the North Dakota 6|18 Initiative. CHI St. Alexius Health provided
commentary of the value they provide and how reimbursement would benefit their program.
This commentary is put into the context of smoking rates and health care costs for Medicaid
enrollees.
Professional Data Analysts | May 2020 3
The NDDoH and Tobacco Cessation
North Dakota was one of the first states in the
United States to develop a statewide plan, a US DEPARTMENT OF HEALTH AND
strategic document to guide tobacco control HUMAN SERVICES 2008 CLINICAL
activities in the state. The framing of and PRACTICE GUIDELINE
RECOMMENDATIONS
alignment with national guidance and specific
state-level strategy is essential for program success
and sustainability. 1. Tobacco use is a chronic disease that
requires repeated intervention and multiple
The Comprehensive Tobacco Prevention and
attempts to quit.
Control State Plan (State Plan) is evaluated each
biennium and reported to the North Dakota 2. It is essential that clinicians identify and
Legislature. The State Plan outlines specific document tobacco use status and treat every
objectives and strategies to accomplish four goals. tobacco user.
Under the cessation goal, “Promoting quitting
among adults and youth”, one objective from the 3. Tobacco dependence treatments are
2019-2021 State Plan is to “Increase the number effective across a broad range of populations.
of health care settings that use the systems
approach for tobacco dependence treatment” 4. Brief tobacco dependence treatment is
as recommended in the United States (US) Public effective.
Health Service Treating Tobacco Use and
Dependence, Clinical Practice Guideline-2008 5. Individual, group, and telephone counseling
Update. A listing of the ten major are effective, and their effectiveness increases
recommendations can be found in the box to the with treatment intensity.
right.
6. Seven first-line medications (5 nicotine and 2
The strategies to meet this State Plan objective non-nicotine) increase long-term smoking
align with the Clinical Practice Guidance and abstinence rates. Combinations of certain
include engaging with health care systems to medications should be considered.
implement and deliver the Ask-Advise-Refer (AAR)
intervention: 7. The combination of counseling and
medication is more effective than either one
Ask patients about tobacco use, alone.
Advise them to quit,
Refer them to evidence-based cessation services 8. Clinicians should ensure access to and
like NDQuits. promote quitline use.
9. Clinicians should use motivational
Additional activities in the State Plan that involve
interviewing techniques to increase likelihood of
cessation and health systems include
future quit attempts.
implementing protocols to assess all patients at
each visit for tobacco use, promote and maintain 10. Insurers should ensure that all insurance
tobacco treatment protocols, promote cessation plans include the counseling and medications
education events, and determine reportable discussed here as covered benefits.
variables from the EHR.
Professional Data Analysts | May 2020 4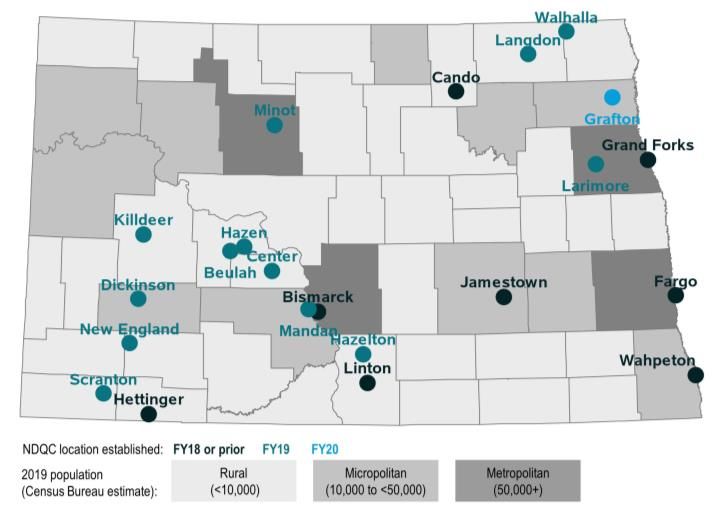
Development of Cessation
Programming in Health Systems:
The North Dakota Million Hearts®
’S’ Program
In 2011, the Centers for Disease Control and Prevention (CDC) partnered with the Centers for
Medicare & Medicaid Services (CMS) to launch the Million Hearts® initiative. The initiative’s goal
was to prevent one million heart attacks and strokes in the US over five years by focusing on the
ABCS of heart health (below).
ABCS of Heart Health
Aspirin use when appropriate,
Blood pressure control,
Cholesterol management, and
Smoking cessation.
To achieve the goal, Million Hearts® solicited regional, state, and local partners to increase focus
on the ABCS, fostering clinical innovations (including billing reform), expanding the use of health
information technology, expanding community initiatives to support healthier behaviors, and
identifying and sharing successes. By 2012, over 12,000 individuals and organizations had
championed Million Hearts®, including federal agencies, physicians, nurses, pharmacists, private
insurers, community health workers, employers, health advocacy groups, and community
organizations.
In 2012, inspired by the Million Hearts® initiative, the NDDoH created the NDQuits
Cessation (NDQC) Grant Program, coining the North Dakota Million Hearts® ‘S’ Program.
This program was focused on the advancement of tobacco treatment efforts in health care systems.
Systems were asked to start Tobacco Treatment Programs (TTP), primarily in the inpatient setting,
and later expanding to outpatient settings. As part of the TTP, systems were asked to train and
certify staff as Tobacco Treatment Specialists (TTS), implement and follow an ask-advise-refer (AAR)
process, to make changes to their EHR for easier reporting and referrals to NDQuits, and to track
outcomes data. Later, an education component was added. In the first year of the NDQC Grant,
there were four grantees - CHI St. Alexius Health Bismarck, Sanford Health Bismarck, Sanford
Medical Center Fargo, and First District Health Unit.
Professional Data Analysts | May 2020 5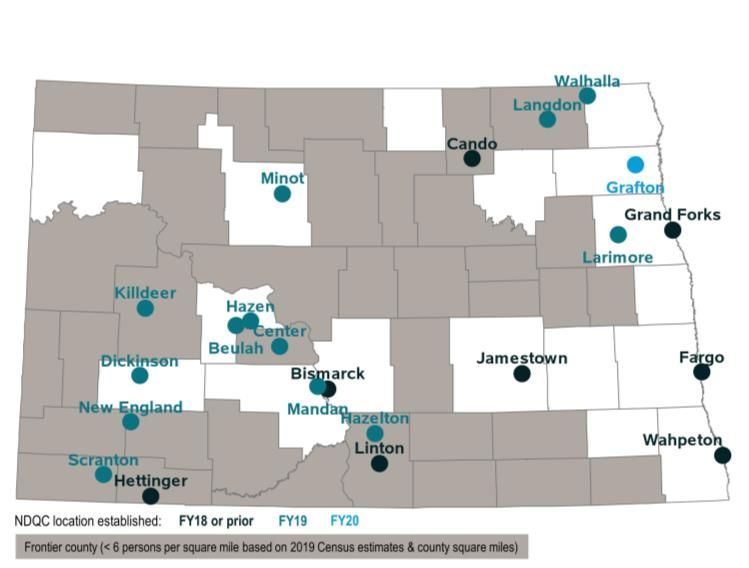
CHI St. Alexius Health Bismarck
CHI St. Alexius Health Bismarck was founded in 1885 by Benedictine Sisters. It was the first
HISTORY
hospital in the Dakota Territory and eventually became known as St. Alexius Medical Center. In
2014, St. Alexius Medical Center joined Catholic Health Initiatives (CHI), a non-profit, Roman
Catholic faith-based care system and was renamed CHI St. Alexius Health. In 2016, several North
Dakota CHI health care facilities joined to form a regional health care network, including CHI St.
Alexius Health Bismarck. CHI St. Alexius Health is sponsored by the Benedictine Sisters of
Annunciation Monastery in Bismarck and abides by the Ethical and Religious Directives for
Catholic Health Care Services as promulgated by the United States Conference of Catholic
Bishops. In 2019, CHI merged with Dignity Health to form CommonSpirit Health. The regional
system serves residents of central and western North Dakota, northern South Dakota, and eastern
Montana.
CHI St. Alexius Health Bismarck is a 286-bed acute care medical center providing tertiary care
ABOUT
inpatient services and a wide range of primary and specialty outpatient services. The site also
offers home health and hospice services, durable medical equipment, and a fitness and human
performance center. Throughout this report, references to CHI St. Alexius will indicate the CHI St.
Alexius Health Bismarck facility.
“Smoking and tobacco use cause so many health issues for our
patients and community, and we knew we needed to do something
about it.” – Rajean Backman, “The Journey Newsletter,” 2018
The beginning of the NDQC Program at CHI St. Alexius Health
In 2010, CHI St. Alexius Health Bismarck partnered with the
University of Mary to conduct a Community Health Needs
Assessment to address strategies for the future health
needs of the counties served by St. Alexius Medical Center.
The report identified six prevalent disease groups,
including cardiovascular disease, Alzheimer’s disease,
cancer, respiratory disease, diabetes, and obesity.
Smoking and tobacco use was called out as a major risk
factor for at least four of these conditions. While tobacco
cessation was not directly addressed as one of the health
Rajean Backman, RRT, AE-C, TTS initiatives following the needs assessment, it was on the
Backman is a Respiratory Therapist
radar. CHI started offering the American Lung Association’s
Freedom From Smoking® classes, and in 2011, CHI
Care Manager and Tobacco Treatment became a smoke-free facility.
Specialist at CHI St. Alexius Health. She
initiated the Tobacco Treatment Working together, Andrea (Lennick) Smetana, Rajean
Program at CHI in 2012 and has worked Backman, and Angie (Anderson) Basaraba launched the
diligently to continue and expand the NDQC work at CHI St. Alexius Health by applying for and
program today. Photo from chistalexiushealth.org. being awarded NDQC Grant funding at the start of the
fiscal year (FY) 2013.
Professional Data Analysts | May 2020 6
The Keys to CHI St. Alexius Health’s
NDQC Success
CHI St. Alexius Health has been developing a successful Tobacco Treatment Program (TTP) since 2012. Through
all of the expansions, challenges, progress gained, and setbacks encountered, there are four aspects of CHI St.
Alexius Health’s program that set them up for success. Each aspect is introduced below and then detailed in other
sections of the report.
Chronic disease point-of-view
CHI St. Alexius Health’s approach is that they consider tobacco use a chronic
disease and treat it as such. This means they provide tobacco cessation
counseling for all hospital inpatients that report using tobacco or nicotine,
regardless of the patient’s readiness to quit. Backman explains their approach
saying, “We don't ask people if they want their diabetes treated or their heart
failure, or their hypertension, or whatever. It's a chronic disease, and when you're
here, you manage it.”
Dedicated TTP team with a strong leader
Championing the program for CHI St. Alexius Health is a core team of four
individuals with a passionate leader. This team provides tobacco cessation
counseling services, provider education, pursues EHR revisions, gathers data,
works on program expansions, develops a rapport with providers, reviews and
revises protocols, organizes an annual two-day conference, and keeps the
program running. This team goes above and beyond for their patients, and
their program is stronger for that commitment.
Strong collaborations
The CHI St. Alexius Health TTP team has built strong collaborations with the
NDDoH and the other grantees. The collaboration between CHI and the
NDDoH was strong from the beginning – the NDDoH knew they needed to
partner with health systems, but at the time there was no template to follow.
The NDDoH let CHI figure out what was going to work for them, and CHI kept
open lines of communication with the NDDoH when they needed help or had
problems. Together, the two organizations built a solid foundation for
tobacco cessation work in the hospital.
Persistence & Adaptability
Throughout the duration of CHI St. Alexius Health’s work through the NDQC
Grant, the team’s persistence in not only pursuing and achieving grant
deliverables but also adapting to changing contexts for their work is readily
apparent. CHI’s work plans and quarterly progress reports showcase their
commitment to achieving deliverables and streamlining their work. Their
progress also demonstrates how they can adapt, re-focus and continue their
work, and work together or with different partners when facing contextual
barriers (EHR change, e-referrals, and nicotine replacement therapy (NRT)
standing orders). This persistence and adaptability is another key to their
success.
Professional Data Analysts | May 2020 7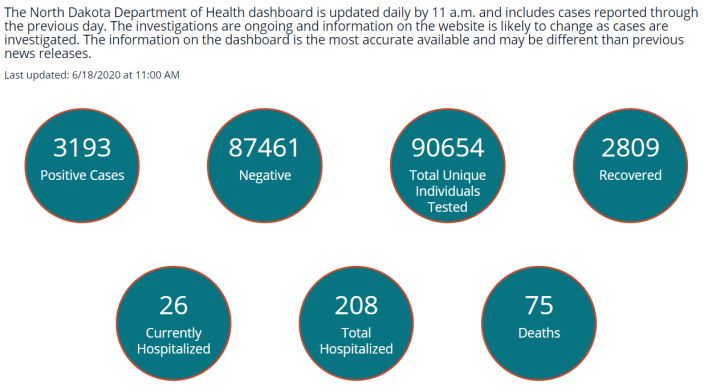
Starting the NDQC Program at
CHI St. Alexius Health, 2012–2014
Starting with a solid foundation
When the NDQC Grant was awarded to CHI St. Alexius Health in 2012 (along with three other
grantees), Freedom From Smoking® classes were already being offered and two staff had attended
TTS training, but there was no formal tobacco counseling protocol in the hospital. The main focus
of the NDQC Grant for CHI St. Alexius Health was to develop an inpatient tobacco cessation
program; a secondary focus was to implement parts of the TTP to other areas of the health care
system.
Building the Program
When asked about launching the TTP, Ms. Backman recalls,
“I've met with everybody from the medical director to every physician group, every
nursing group. I've had a conversation with I think just about everybody that is in this
building.”
In the first years of the grant, the CHI TTP team, led by Ms. Backman, started building a program
from the ground up. Using the Mayo Clinic Nicotine Dependency Model as a guide, they:
✓ Developed and implemented inpatient tobacco use assessment and cessation
counseling guidelines, taking a chronic disease approach to see all patients
✓ Created an NRT voucher system and implemented NRT standing orders
✓ Started billing for services
✓ Worked with Information Technology (IT) to create an EHR report for
identifying tobacco users needing counseling
✓ Presented the protocols and received approval from the Medical Executive
Committee, the Nursing Leadership Counsel, Health Information
Management, the Pharmacy and Therapeutics Committee, the Clinical
Integration Network, and the outpatient family practice physicians
✓ Increased the number of staff with TTS training from two to six
✓ Started counseling outpatients, when requested
✓ Started offering the BABY & ME – Tobacco Free Program to support cessation
with pregnant and postpartum women
During this time, the TTP team was approached by the CHI St. Alexius Health Quality department to
help implement the Joint Commission Tobacco Measure Set for behavioral health patients.
The TTP team established a collaboration with the behavioral health unit, ultimately meeting the
Joint Commission’s requirements.
In the fall of 2014, St. Alexius Medical Center joined with Catholic Health Initiatives (CHI) to become
CHI St. Alexius Health, signaling larger organizational changes to come, including being recognized
as an Accountable Care Organization for Medicare services.
Professional Data Analysts | May 2020 8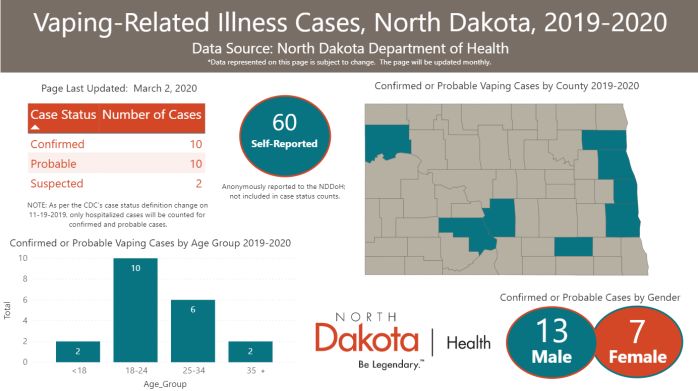
Expanding CHI St. Alexius Health’s TTP
Amid Setbacks, 2015–2017
Expanding TTP: Challenges
Despite early success establishing and growing a TTP, the next years brought organizational
challenges.
EHR Conversion E-Referrals Organizational Contraction
In fall 2015, the EHR was Prior to the EHR change, CHI The last major change was an
converted from McKesson to St. Alexius was exploring organizational contraction,
EPIC. This impacted the bidirectional electronic including budget cuts,
team’s processes, (i.e., report
identifying newly admitted referrals (e-referrals) with the layoffs, and a hiring freeze
patients reporting tobacco NDQuits quitline vendor. implemented in 2016. This
use needed to be rebuilt), After much discussion, CHI freeze meant the TTP team
patient care (i.e., NRT St. Alexius Health leadership could not grow and when
standing orders did not decided e-referrals posed too members of the team left,
transfer so TTS needed great a risk to patient privacy they could not be replaced.
physician sign-off to order and decided not to pursue. Eventually, this led to a
NRT for each patient), and Instead, CHI St. Alexius staffing shortage where TTP
grant reporting (i.e., NDQC Health first added a members were having to
data reports were not
transferred). The effects of checkbox to the EHR that prioritize patient care and
this change were prolonged would generate an NDQuits tobacco cessation counseling
due to new organizational fax referral form that could for admitted patients over
processes where IT requests be printed and faxed, and conducting follow-up calls
were triaged using a system- later set up automatically with patients that had been
wide prioritized ticketing generated e-faxes. discharged.
system.
Expanding TTP: Introducing Quit Kits
In 2016, the TTP team introduced Quit Kits,
personalized packets with tools to support patients in
their quit journey. The kits included: stress balls, pen
and paper to write goals, hard candies and gum,
“tough enough to quit” cessation bracelets, and
prayer coins for mediation. These tools were given to
patients to encourage them to use the quit strategies
discussed during cessation counseling.
Ms. Backman described how Quit Kits fit into their treatment protocols in an interview in CHI’s “The
Journey Newsletter” (2018): ”We initially meet with patients to provide cessation counseling services.
We find out what will make their cessation journeys successful, and we provide them with customized
‘Quit Kits’ filled with all sorts of items tailored to their specific needs. From there we enroll them into
NDQuits, and we also follow-up with them on the dates they ask us to.”
Professional Data Analysts | May 2020 9
Expanding CHI St. Alexius Health’s TTP
Amid Setbacks, 2015–2017
Expanding TTP: Building internal rapport and collaborations
Even with these organizational setbacks, the CHI TTP team continued to expand their program.
Once the inpatient protocols were in place and outpatient referrals were set-up, Ms. Backman led
the TTP team in establishing collaborations with CHI specialty areas, including: cardiology,
pulmonology (through the Heart and Lung Clinic), endocrinology (specifically patients with
diabetes), behavioral health, and the surgery center.
The 2015 CHI TTP Team “We have had a lot of success gaining clinician
buy-in when we approach one provider at a
time. Sometimes it's a brief encounter in the
hallway, sometimes it is a discussion when
asking for nicotine replacement therapy for a
particular patient, and sometimes we send
e-mails with literature attached highlighting the
evidence that supports our cause.”
Rajean Backman, Alison Harrington, Traci
Hutslar, Missy Lutman, Jordan Buchholz – Rajean Backman, NDQC FY20 Progress Report, Jan 2020
As the TTP grew, Ms. Backman reflected on how more and more providers started trusting their
cessation counseling and becoming interested in tobacco cessation. She recalls,
“When we first started doing this, you'd walk into a room, and if a nurse came in, they were irritated.
‘Oh, she's here to talk about smoking,’ roll their eyes and kind of point towards the door. And then you
found more that they were wanting to hang out in that room to see what you had to say and realizing
that this just wasn't telling people that they had to quit.”
Expanding TTP: Building external collaborations & sharing successes
In addition to internal collaborations, the TTP team also started collaborations with the
CHI Mandan Clinic and Mid Dakota Clinic. CHI Mandan first began referring patients to CHI
Bismarck for services, but eventually, CHI Bismarck staffed TTS outpatient services at the CHI
Mandan Clinic. Mid Dakota also collaborated with CHI St. Alexius, implementing an e-referral for
their patients who use tobacco to receive outpatient counseling at CHI.
This was also when CHI ramped up their education and outreach efforts. Most notably, they started
the Nicotine Dependence Conference (NDC) in Bismarck, ND. This conference has grown to be
a two-day annual event co-sponsored by three grantees. The event is highly attended,
offers continuing education credits, and is well received by attendees as motivating and applicable
to their work.
In 2016, the CHI St. Alexius Respiratory Therapy Managers were invited to meet with
the NDDoH and CDC representatives to discuss the health systems changes and TTP workflows
implemented with NDQC Grant funding. The CDC found their experiences and feedback very
valuable. In 2017, CHI St. Alexius Health was invited to attend the North Dakota Quarterly Partners
Meeting, providing valuable insight regarding tobacco cessation in health care systems.
Professional Data Analysts | May 2020 10Tobacco Cessation at CHI St. Alexius Health
During Public Health Crises, 2018–2020
Refining the Tobacco Treatment Program
In the last few years, CHI St. Alexius Health has continued to refine its program and make changes
to their EHR (e.g., adding the advisory statement to after visit summaries, adding SmartPhrases to
help with documentation, adding electronic nicotine delivery systems (ENDS) screening questions).
They continue to explore re-establishing their standing orders for counseling (approved) and NRT
(still in progress) and exploring new collaborations (emergency department and occupational
health).
Their focus on continued learning was intensified in the last couple of years:
- Co-sponsoring the annual Nicotine Dependence Conference with Sanford and Mid Dakota Clinic
- Participating in community events like the Family Fun Day with the Bismarck Larks
- Speaking at colleges, attending the TPCP Quarterly Partners Meetings
- Authoring and providing interviews for newspapers, newsletters, and magazines
ENDS epidemic and vaping-related lung injury investigation (EVALI)
In 2017, JUUL was introduced as a new electronic nicotine device system (ENDS). With ENDS use
rates on the rise, especially in youth and young adults, CHI St. Alexius Health implemented ENDS
screening questions in their EHR, participating in a system-wide CHI national initiative. The NDDoH
released a position statement in 2018 saying ENDS were not considered cessation devices. Later in
2018, the US Surgeon General announced the growing rate of ENDS use by youth and young
adults was an epidemic that needed to be addressed.
In 2019, the vaping epidemic turned deadly when a
national outbreak of e-cigarette, or vaping, caused
product use-associated lung injury (EVALI). Patients
with EVALI tended to be younger, otherwise healthy
individuals that presented with severe, sometimes
fatal lung infections. Both CHI St. Alexius Health and
the NDDoH responded by quickly submitting data
to the CDC and highlighting the dangers of ENDS
products in public communications.
Novel Coronavirus (COVID-19) Cases Screenshot from https://www.health.nd.gov/vaping; Accessed June 18, 2020
In March 2020, the novel coronavirus (COVID-
19), an infectious disease that primarily affects
the lungs, spread across the nation. In North
Dakota, businesses and schools closed to help
stop the spread of the disease. CHI St. Alexius
Health TTP responded to this public health crisis
by modifying their workflow to wait for COVID-
19 test results before counseling. As a result of
the pandemic, there were more inpatients
Screenshot from https://www.health.nd.gov/diseases-conditions/coronavirus; needing counseling and fewer outpatients.
Accessed June 18, 2020
Professional Data Analysts | May 2020 11CHI St. Alexius Timeline in Context
The contextual internal and
external factors were right for CHI
2009 – 2011 The
CDC & St. Alexius Health (CHI) to partner
NDDoH
Internal and external CMS engages with the NDDoH on NDQC. The
factors align for more launch health timeline below shows how the CHI
Million systems TTP evolved alongside the NDQC
focused tobacco Program more generally. Key
Hearts CHI
cessation work within events below are designated as
conducts successes and challenges.
North Dakota health needs
care systems. assessment
2012-2014 NDQuits Cessation
The NDDoH launches Grant Program begins
the NDQC Grant
Program & CHI
becomes one of the The NDDoH makes progress CHI launches their Tobacco Treatment
four first grantees. on the TPCP plan; meanwhile Program (TTP) by creating inpatient
JUUL is introduced, starting treatment protocols, training TTS, and
the vaping epidemic. establishing NRT and billing practices.
2015-2017 CHI undergoes system-wide changes
Both the NDDoH and including converting their EHR to EPIC,
CHI experience NDQC In 2017, the North Dakota forming a regional care system, and
Program growth amid legislature cuts TPCP funding; implementing a hiring freeze.
NDDoH assumes administration Meanwhile, the TTP expands tobacco
budget cuts.
of all tobacco prevention and cessation counseling to hospital specialty
control efforts in North Dakota. departments and outpatients, starts
collaborations with CHI Mandan Clinic
and Mid Dakota Clinic, and sponsors the
2018-2020 The NDDoH releases position 1st Nicotine Dependence Conference.
The NDDoH and CHI statement on ENDS, indicating This conference becomes a successful
respond to the vaping is not a cessation tool; annual event in partnership with other
escalating vaping the NDQC Grant Program NDQC grantees.
expands to include 17
epidemic.
grantees.
CHI refines and makes improvements
to their TTP by making EHR changes,
The vaping epidemic escalates; adding ENDS screening questions, getting
the NDDoH contributes data to standing orders for counseling, and
the national vaping-related lung contributing data to EVALI.
injury investigation (EVALI);
COVID-19 emerges as public
health crisis. COVID-19 disrupts typical patient care.
Professional Data Analysts | May 2020 12CHI St. Alexius TTP Detailed Timeline
Over the course of their NDQC Grant participation, CHI St. Alexius Health has had many successes, forging the
way in developing inpatient and billing protocols, establishing rapport with other clinical areas, and creating a
culture of continued learning. They have also had set-backs and put effort into ideas that did not materialize. The
detailed timeline below provides some specific examples of these activities.
CHI St. Alexius Health Successes CHI St. Alexius Health Work In-progress &
New activity Challenges
New challenge/barrier
2012 • Inpatient protocols developed following Mayo • Working to develop a system to provide NRT
model • Working on follow-up plan: possibly using
• Continued Freedom from Smoking® classes technology to call patients three times after
• Met with physicians, introduced them to program discharge
2013 • EHR report created • Working with informatics team to develop detailed
• NRT voucher process with pharmacy created tobacco cessation documentation
• Developed patient handouts • Working on patient education handouts
• TTS counsel first patient • Working on setting up billing system
• Refined inpatient protocol
2014 • Started counseling outpatients as requested • Working on ability for TTS to order NRT through
• Started to bill for services EHR standing orders
• Started BABY & ME – Tobacco Free Program
• Created report to identify tobacco users
2015 • Expands to hospital specialty areas • EHR system converted to EPIC, reports and
• Collaborated with CHI Mandan Clinic and Mid documentation need to be re-created
Dakota Clinic • NRT standing orders did not transfer, TTS
unable to order without physician contact
• Working through how to collect follow-up data
(limited staff capacity)
2016 • Started the Nicotine Dependence Conference • Hiring freeze begins
(NDC) • Working with IT to rebuild reports, data collection
• Added NDQuits referral form to EHR still manual
• Started exploring e-referrals
2017 • Added new questions to EHR tobacco history • Unsuccessful implementation of the EHR e-
section locally and throughout CHI National referral into NDQuits
• Added e-fax referrals from EHR to NDQuits • Difficult to make changes in EPIC
• Hosted 2nd annual NDC • Working on expanding to Occupational Health
2018 • Added advisory statement as part of the after • Change in priority funding for follow-up calls
visit summary in EHR • Working on billing for carbon monoxide tests and
• ENDS screening added to EHR cotinine tests, which screen for tobacco abstinence
• Hosted 3rd annual NDC with Sanford
2019 • Helped sponsor local TTS training • Working on protocol for Emergency Department
• Hosted 4th annual NDC with Sanford • Working to receive referrals from CHI Mandan
Clinic (Lung cancer pre-screen)
• Working to re-implement standing orders for
inpatient counseling and NRT
2020 • Presented at United Tribes Technical College • COVID-19 emerges as public health crisis and
• Hosted 5th annual NDC with Sanford and Mid disrupts patient care
Dakota Clinic
Professional Data Analysts | May 2020 13CHI St. Alexius’s Collaborative Approach
CHI St. Alexius Health’s collaborative approach and culture of continued learning have contributed to successes
with the implementation and expansion of a TTP over the past eight years. Specifically, CHI St. Alexius Health has
seen working with other health systems and other NDQC grantees as a great asset to their work. Throughout the
duration of the NDQC Grant, CHI St. Alexius Health has found creative and engaging ways of educating their
community and spreading awareness about the importance of tobacco cessation.
“If you're hoarders of information, things don't grow. And that
doesn't help anyone. You have to share what works and you have
to share what doesn't work.” – Rajean Backman, Interview with PDA, April 3, 2020
4th annual Nicotine Dependence Conference Grantee Partnerships
sponsors (2019) One significant collaboration with other NDQC grantees is
hosting the annual Nicotine Dependence Conference. CHI
founded the conference in 2016. Since then, they have
engaged other grantees in planning, hosting, and offering
continuing education credits for the conference, helping
to set the tone for shared learning across health systems.
CHI St. Alexius Health has also been open and
enthusiastic about exchanging information and best
practices with other health systems.
Photo: Rajean Backman (CHI St. Alexius Health); Teresa Kershaw (Sanford Bismarck); Therese Shumaker (Mayo); Missy Lutman, Traci Hutslar, and
Angie Basaraba (CHI St. Alexius Health). Photo provided by Kara Backer, NDDoH TPCP.
Community Engagement
CHI St. Alexius Health has engaged and educated the public through the following activities:
➢ Broader community-wide events: Innovative events, like
the Family Fun Day with the Bismarck Larks (pictured right),
Summer Fun and Safety Day, and participating in the North
Dakota Safety Conference help increase awareness about
the harms of smoking and vaping.
Photo: On June 23, 2019, CHI St. Alexius Health sponsored a Family Fun Day with the Bismarck Larks
baseball team, including a “knocking tobacco out of the park” activity station. Photo from Bismarck Larks
baseball page.
➢ Education for the general public and CHI employees:
Offering Freedom from Smoking® classes to the general
public and staff at CHI St. Alexius Health, especially at the
beginning of the grant, solidified CHI’s TTP role and
commitment to tobacco cessation. CHI TTS also author
content and contribute interviews to many newspaper,
magazine, and newsletter articles each year.
➢ Training the next generation of tobacco cessation specialists: Allowing respiratory therapy
students to do rotations or shadow at CHI St. Alexius Health, having staff teach at local
colleges, and sponsoring local TTS training courses contribute to the culture of continued
learning through real-world experiences for those entering the field.
Professional Data Analysts | May 2020 14CHI St. Alexius Health Reach in Context
NDQC Reach
In FY20, the NDQC Program has 17 grantees providing face-to-face visits in 22 cities across the
state and telehealth visits in many more. NDQC grantees are providing tobacco cessation
counseling in eight frontier counties. When looking at county population designation, NDQC is
reaching 10 rural counties, five micropolitan counties, and all four metropolitan counties.
Established grantees tend to be larger health systems serving more major metropolitan areas with
newer grantees serving more rural areas.
NDQC locations overlaid on frontier counties (left) and county population designations (right)
NDQC grantees include hospitals, clinics, and specialty care centers (college campus health
clinics, addiction treatment facilities, Federally Qualified Health Centers, and cancer centers),
meeting the activity goals outlined in the TPCP State Plan regarding NDQC grantee diversity.
In FY19 alone, NDQC grantees’ 101 Tobacco Treatment Specialists
provided cessation counseling to over 13,000 patients.
NDQC Reach within CHI St. Alexius Health Bismarck
Priority populations reached by CHI TTP:
• Pregnant women • Patients with diabetes
The TTP at CHI has continually expanded the
• Psychiatry & • Cardiology
patient populations it serves. In 2013, the
Behavioral Health • Pulmonology
Tobacco Treatment Protocols were established
for hospital inpatients. From there, the TTS team In the last five years, the CHI TTP
expanded to counseling outpatients, other
hospital areas, the CHI Mandan Clinic, the Mid
has counseled almost 7,500 patients
Dakota Clinic, and, in FY19, started developing with only four TTS.
protocols with the Emergency Department.
In FY19, CHI TTS counseled 1,490 patients,
provided quit kits and bridge NRT to 546
patients, and referred 41 patients to NDQuits.
Professional Data Analysts | May 2020 15NDQC Impact at CHI St. Alexius Health
Due to staffing shortages, quantitative data related to quit outcomes is not available. Instead, impact is
highlighted through provider testimonials regarding importance of the program and a number of case studies
showing how CHI St. Alexius Health’s tailored, patient-centered approach to tobacco cessation has made
improvements in patient lives.
“It's more than just telling people that they should quit. It's quality of life,
it's longevity of life... I think it's giving every person that opportunity to
have that lifestyle change.” – Rajean Backman, Interview with PDA, April 3, 2020
Provider Testimonials
“Tobacco usage is rampant in North “Having these professionals available to
Dakota, is difficult to discontinue, speak with patients in our clinic has been
and a significant risk for coronary extremely helpful and often successful in
artery disease as well as other smoking cessation. Our ability to treat
serious pathologies. …The services patients is often hindered by smoking.
that these individuals supply should Guidance from this group is
not be underestimated.” -Nicholas immeasurable to the patient as well as
Mahr, MD, Letter of support, 2017 ourselves.” -Debra Fueller, FNPc, Letter of
support, 2017
Patient Success Stories
Providing cessation counseling to all tobacco users Creating individualized treatment plans:
following a chronic disease approach: “A 31-year-old female outpatient was counseled. She routinely
“A 74-year-old male was admitted to the hospital for chest pain. smoked up to two packs of cigarettes per day. She had a rolling
He has a history of smoking a pipe daily for 59 years. He "had machine and bought bags of tobacco. She was trying to reduce
tried everything" to quit smoking. During his overnight the number of cigarettes she was smoking. She did not want to
hospitalization he had a heart catherization and had 1 stent use a nicotine patch or gum (used in the past and didn't like
placed. When he was approached about tobacco cessation, he either of them) and was afraid she would chew the nicotine
was dressed and ready to be discharged. He was definitely in lozenges. We reviewed the other cessation pharmacotherapy;
the ‘precontemplative’ stage of change. His wife and daughter she had never seen the nicotine inhaler before. She used a
were at his bedside. Nine days later, this patient called the TTS pharmacy voucher for 42 nicotine cartridges and mouthpiece.
and stated he has not smoked since he was discharged from She called on the way home and stated she would be giving
the hospital but is having some pretty intense cravings and was her rolling machine to a friend that day. She has been tobacco
calling for help. We have had weekly phone contact for three free since 9/10/19.”
weeks now and he has not smoked for 23 days (which is the
longest he has ever been abstinent). The moral of this story is: Helping patients through times of crisis:
if we only counsel those that are already motivated to quit, this “A 19-year-old male was admitted to the hospital for e-cigarette
gentleman would still be smoking.” or vaping product use-associated lung injury (EVALI). He was
vaping with CBD cartridges he bought "on the streets." There
Going above and beyond to coordinate cessation were multiple hours spent counseling this patient (by both the
resources: TTS staff and the hospitalist). No nicotine replacement therapy
“A 75-year-old male was using one can of smokeless tobacco was used. The TTS staff made a follow-up phone call two
per week. He tried the herbal chew from our quit kits while in weeks after hospital discharge. The patient states that he has
the hospital and really liked it. We called the gas station in his not vaped/smoked/JUULed since discharge. This patient is a
hometown and asked if they would special order the herbal college hockey player and notices that his breathing is getting
chew and they were happy to help us. One-month post much better and feels that he is able to skate more
hospitalization, the patient states that he is still using the herbal aggressively, and his endurance is much better.”
chew saying, ‘I think I love you for showing me this.’”
Professional Data Analysts | May 2020 16Assessing Sustainability of
CHI St. Alexius Health’s TTP
The goals of establishing a TTP under the NDQC Grant Program are to become part of the hospital’s standard
operations, to be self-sustaining, and to expand current cessation efforts within the health care system or target
priority patient populations. To assess CHI St. Alexius Health TTP’s sustainability strengths and opportunities, the
following areas were reviewed using a modified Substance Abuse and Mental Health Services Administration
(SAMHSA) sustainability checklist. See Appendix B for the full checklist.
Sustainability Assessment
Skills Structure
TTS training & Job responsibilities &
staff education descriptions include
Environment TTP tasks
Internal & external
factors driving TTP work
Quality Improvement
Metrics measured,
shared, & reflected on
Strategy
Aligns with mission Sustainability Technology
& has business plan EHR upgrades
support TTP work
Leadership Culture &
Billing
Communications
Bill for counseling,
Leadership engaged & Protocols & Process
NRT, & all tests
TTP team empowered TTP processes in place &
being followed
Sustainability Conclusions
CHI Strengths: CHI Opportunities:
Highly-focused attention to development and → Consider how aligning tobacco cessation work
maintenance of protocols processes and with other policies and/or framing work in
building these into the EHR (twice); terms of overall organizational mission/vision
Maximizing billing to support program costs can make a robust business case for tobacco
and to enhance sustainability; cessation;
A passion for tobacco cessation and raw → Formalize relationships with existing
determination to see the effort succeed that champions to strengthen leadership
leads to engagement and education of engagement and buy-in; and
hospital and health system colleagues; and → Obtain support to track measures and report
Learning from and sharing with the other them to maintain staff engagement and
NDQC grantees, as well as creating leadership support.
opportunities for others to learn.
Professional Data Analysts | May 2020 17NDQC, CHI, & The 6|18 Initiative
The 6|18 Initiative: The NDDoH and the North Dakota Department of Human Services Medicaid Office are
collaborating on the CDC-funded 6|18 Initiative to reduce tobacco use. The future goal of the 6|18 Initiative is for
certified tobacco treatment specialists (CTTS) or TTS, who have the National Certificate of Tobacco Treatment
Practice (NCTTP), to be recognized as Designated Providers for Medicaid. This will enable CTTS or NCTTP to be
reimbursed by Medicaid for outpatient counseling. Currently, there are at least 45 CTTS/NCTTP providers within
the NDQC Grant Program.
Almost 40% of North Dakotans with Medicaid coverage smoke cigarettes (39.1%).
This is more than double the rate of smoking in North Dakota overall (19.1%).
Better Care, Together
Counseling is linked to successful tobacco cessation. There is a strong dose-response relationship
between time spent in face-to-face counseling and quitting tobacco. A brief chart review found
CTTS at CHI St. Alexius Health Bismarck spent an average of 55 minutes providing cessation
counseling per outpatient.
Physician:
“Data demonstrates that patients are CTTS:
more likely to quit with proper “I think it's a great opportunity, too. I
counseling and pharmacotherapy. mean I think that the providers that
[The TTS] allow me to work more can bill for it and be reimbursed, I
efficiently and assess more patients don't think they have the time to do
on a daily basis who may also need what we're doing.”
cessation counseling.”
Saving Money-Saving Lives
Annual health care costs in North Dakota directly caused by smoking are $326 million. Almost 20%
of those costs - $57 million – are paid by Medicaid.1
A study in Massachusetts found that every $1 in program costs was associated with $3.12 (range
$3.00 to $3.25) in medical savings, for a $2.12 (range $2.00 to $2.25) return on investment to the
Medicaid Program for every dollar spent.2 These savings were realized within one year of the
benefits being used.
Short-term (≤ 3 years) Long-term (5+ years)
Health impacts3 Circulation improves and breathing is easier; reduced Reduced risk of stroke, cancer, and coronary artery
risk of respiratory infections disease; longer life expectancy
Cost savings Outpatient cessation treatment can lower health care Post-stroke care can cost an average of $4,850 each
costs within 18 months of quitting. Within three years, a month, accumulating to over $58,000 in health care
former smoker’s health care costs will be 10% less than costs in the first year alone.5 Health care costs in the
if they kept smoking and expenditures for cessation first month after a diagnosis of lung cancer can
programs in the range of $144 to $804 per smoker will average $37,000; cumulative costs in the first year can
be offset by those health care cost savings.4 average $140,000.6
1 Tobacco Free Kids. (2020, March 9) “The Toll of Tobacco in North Dakota.” https://www.tobaccofreekids.org/problem/toll-us/north_dakota
2 Richard, P., West, K., and Ku, L. (2012). The Return on Investment of a Medicaid Tobacco Cessation Program in Massachusetts. PLOS ONE.
3 CDC. (2020, April 28) “Benefits of Quitting.” https://www.cdc.gov/tobacco/quit_smoking/how_to_quit/benefits/index.htm
4 ClearWay MinnesotaSM. (2016, April 6) “Return on Investment for Tobacco Cessation.”
5 Rajsic, S., Gothe, H., Borba, H. H., et al. (2019). Economic Burden of Stroke: A Systematic Review on Post-Stroke Care. Eur J Health Econ, 20(1): 107-134.
6 Dieguez, G., Ferro, C., and Pyenson, B. S. (2017). “A Multi-Year Look at the Cost Burden of Cancer Care.” Milliman Research Report.
Professional Data Analysts | May 2020 18Conclusions & Recommendations
CHI St. Alexius Health has built a successful TTP
CHI St. Alexius Health started the NDQC Grant in 2012 and built their TTP from the ground up with
the support of the NDDoH. Their history with the NDQC Grant is full of successes and challenges.
Each time a barrier was encountered, the TTP team persisted in maintaining exceptional patient
care, building rapport with clinicians, expanding the program when they could, and providing
opportunities for education. TTP work seemed to happen in three eras:
2012-2014 2015-2017 2018-2020
Starting the NDQC Program Expanding TTP Amid Tobacco Cessation During
at CHI St. Alexius Health Setbacks Public Health Crises
Major Success: Major Success: Major Success:
Establishing their TTP Founding the NDC Increased focus on continued
learning
Challenge: Challenge: Challenge:
Doing it without leadership EHR change & organization Two major public health
champion at the organization contraction crises
When assessing factors contributing to CHI St. Alexius Health’s TTP success, four key
components emerge:
Tobacco use is considered and treated as a chronic disease
A passionate team of dedicated TTS with a strong champion push the program
forward
Strong collaborations with the NDDoH, other NDQC grantees, and their
communities
Persistence in achieving a successful program and adapting to changing contexts
for their work
These components have contributed to large reach and a successful program built by the CHI TTP,
but may not be the keys to success for all NDQC grantees. Varying organizational circumstances,
TTP settings, and other factors may provide other keys to success within other grantees.
There are opportunities to increase sustainability of the TTP
There are many aspects to CHI St. Alexius Health’s TTP that bode well for sustainability including
the strong focus on training, the protocols and policies already in place, and the EHR modifications
that have been made to accommodate TTP work. However, the CHI program lacks higher-level
organizational support.
Recommendations: Strengthening engagement of existing, informal supporters could help the
tobacco cessation team find new ways to align their work within the organization and its priorities,
engage leadership, and obtain resources to support data collection, analysis, and dissemination.
Additionally, the NDDoH should continue to pursue the 6|18 Initiative to aid in reimbursement of
TTS services.
Professional Data Analysts | May 2020 19Appendices
Appendix A – Methods
Appendix B – Sustainability Methods and Checklist
Attachment – Full Timeline
Attached file name: NDQC_CHI_Full_Timeline_FINAL.xlsx
Professional Data Analysts | May 2020 20Appendix A: Methods
For this study, a modified timeline mapping methodology was used covering the time period July
2012 – March 2020. Timeline mapping is the process of chronologically arranging important events,
activities, and other milestone markers, including program and external factors (i.e., social,
economic, political, etc.). Doing this enables stakeholders to see relationships between the factors
on the timeline.
Timeline mapping is meant to be facilitated in a face-to-face, interactive session with all
stakeholder's present. As this was not geographically possible, we used a modified timeline
mapping approach where information from this report was gathered from a comprehensive
historical document review and a phone discussion with the NDDoH staff and CHI TTP staff. The
historical document review consisted of examining and synthesizing information from past grant
announcements, work plans, quarterly progress reports, and other documents into a timeline that
called out success, challenges, and changes in activities over time. In total, over 100 documents
were reviewed spanning the time frame July 2012 – March 2020.
When reviewing the documents, all documents were catalogued and sorted by type. Each
document was reviewed, and information related to CHI accomplishments, barriers, works in
progress, and collaborations were abstracted chronologically. An initial timeline was created.
Internet searches supplemented the information found within documents.
Data Source Key details
NDQC Grant The annual call for funding highlights key aspects of the grant that the grantees should be working
Announcements towards with grant funding. Data abstracted from these documents include the grant components and
requested metrics for EHR data reporting.
NDQC Work Plans These documents contained the proposals for NDQC funding submitted to the NDDoH each year. They
often contained achievements from the prior year and plans for what they wanted to work on in the
upcoming year.
NDQC Progress The frequency and length of these reports as well as the types of information, variety of questions asked,
Reports and level of detail requested changed over time. Program accomplishments, barriers, reach, patient
success stories, and educational event summaries came from the progress reports.
Supplemental The NDDoH supplied a variety of supplemental materials including newspaper articles featuring
Materials interviews with CHI TTP staff, newsletters with articles authored by CHI TTP staff, photos, letters of
support, and sample EHR screenshots. These pieces of information highlighted collaborations and
education and outreach that were not otherwise highlighted.
From there, PDA facilitated a reflective conversation between the NDDoH cessation staff and CHI
TTP staff on April 3, 2020. During this conversation, progress, themes, and opportunities to date
were assessed and the timeline was reviewed for accuracy, completeness, and a discussion around
event relationships. PDA posed specific questions to clarify gaps in the story and piece together the
flow of important activities and accomplishments. Following the conversation, the conversation
recording was transcribed, reviewed for accuracy, and used as another data source.
All information was then compiled, the timeline refined, and timeline narrative drafted.
Professional Data Analysts | May 2020 21Appendix B: Sustainability Checklist
There is no validated, tailored instrument for the NDDoH to use to assess sustainability for tobacco
cessation systems change among grantees and to provide technical assistance based upon the
results.
To assess the potential for a sustainability assessment to guide the NDDoH and its grantees, PDA
modified a SAMHSA sustainability checklist and used it to explore strengths and opportunities for
CHI. Unlike other checklists, this one included concepts like maximizing billing for services and
engaging in community-wide conversations about tobacco cessation that the NDDoH and CHI St.
Alexius Health identified as important elements of sustainability in their NDQC work.
The modified checklist included nine sustainability concepts, along with the reflections for each
assessment criteria, are provided below.
Legend:
? Not enough information from the $Another look might yield new
Already addressing this concept document review to assess ideas or opportunities
Sustainability Concept and Assessment Reflections
Environment – What does the internal and external environment require of your program?
What internal and external policies drive the Tobacco Joint Commission measures drove the behavioral
Treatment Program (TTP) and reporting? Is your
program responding?
$ health collaboration. Are there other
opportunities to coordinate work?
Is your program exploring new revenue streams to Are there non fee-for-service payment
partially cover costs and/or demonstrate value? $ opportunities that might also help to
demonstrate value like Accountable Care
Organizations?
Is your program taking advantage of opportunities to CHI has set the standard for learning and
learn/share with others engaged in similar work? sharing for the NDQC Grant.
Strategy – What gives the program direction?
?
How is the TTP integrated in your organization’s Integration between the tobacco policy and
mission and vision? protocol and CHI’s mission/vision is unclear.
Do you have a business case and/or business plan for Business Plan from 2014 could be updated with
the TTP efforts? Can you demonstrate reach or
impact?
$ help from champions from other departments
who see the value of the TTP from other
perspectives.
Billing
Are you billing for all cessation counseling, Yes. The team has identified and taken
pharmacotherapy, and all tests? advantage of many billing opportunities.
Technology
Does the EHR include the 5 A’s or AAR to facilitate The 5 A’s are integrated into the EHR, with
integration into broader workflows? assessments being enhanced regularly.
Are you using registry or other functions like email, The TTP team uses a registry to track patients
text or EHR patient portals to track patients and
provide additional follow-up?
$ needing a TTP visit. Other EHR tools may
support follow-up.
Professional Data Analysts | May 2020 22You can also read