Update on HTN and ABPM - Raj Padwal Division of General Internal Medicine University of Alberta
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Update on HTN and ABPM
Raj Padwal
Division of General Internal Medicine
University of Alberta
Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic Speaking and other Honoraria: Abbott
Outline 1. Understand how to interpret ABPM. 2. Review the pros and cons of different methods to diagnose hypertension. 3. Discuss some current controversies in HTN management.

Epidemiology and Significance
European Society of Hypertension
Classification of Blood Pressure
Category Systolic Diastolic
Optimal
Hypertension in Canada:
Prevalence and Control
Overall prevalence is 21%
McAlister et al. CMAJ 2011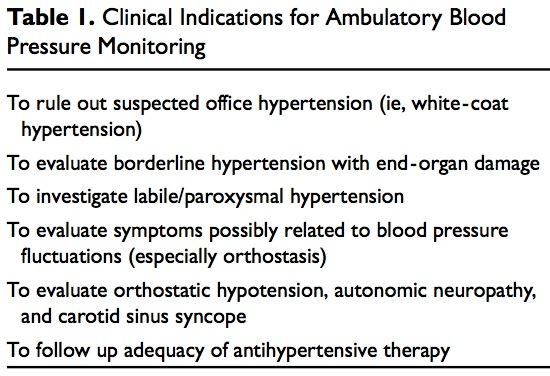
Life time risk of Hypertension in Normotensive
Women and Men aged 65 years
Risk of Hypertension % Risk of Hypertension %
100 100
Women Men
80 80
60 60
40 40
20 20
0 0
0 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
Years to Follow-up Years to Follow-up
JAMA 2002: Framingham data.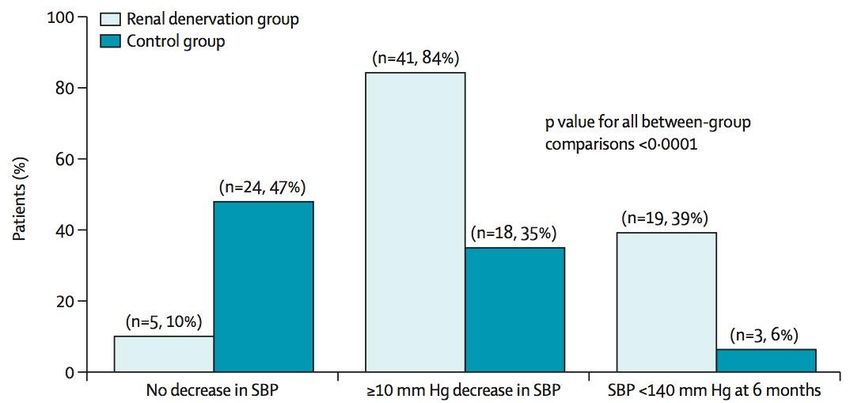
Diagnosing Hypertension
Blood Pressure Assessment:
Patient preparation and posture
Standardized Preparation:
Patient
1. No acute anxiety, stress or pain.
2. No caffeine, smoking or nicotine in the preceding
30 minutes.
3. No use of substances containing adrenergic
stimulants such as phenylephrine or
pseudoephedrine (may be present in nasal
decongestants or ophthalmic drops).
4. Bladder and bowel comfortable.
5. No tight clothing on arm or forearm.
6. Quiet room with comfortable temperature
7. Rest for at least 5 minutes before measurement
8. Patient should stay silent prior and during the
procedure.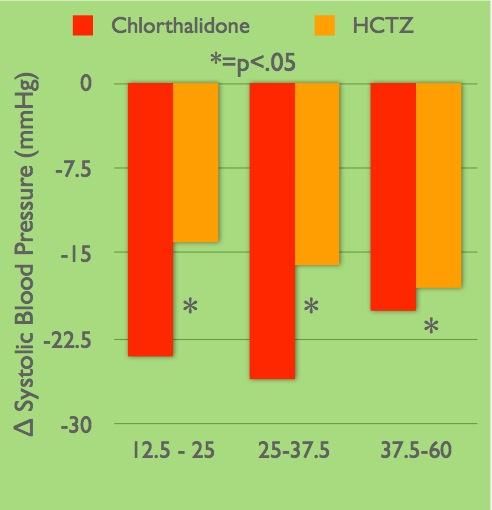
II. Criteria for the diagnosis of hypertension and
recommendations for follow-up
BP: 140-179 / 90-109
Clinic BP ABPM (If available) Home BPM
Hypertension visit 3
>160 SBP or Diagnosis
>100 DBP of HTN Awake BP Awake BP < 135/85 >135/85
135 SBP or
85 DBP or
or 24-hour Confirm
24-hour
130 SBP or with repeat
Hypertension visit 4-5 >80 DBP Home BPM
or ABPM
>140 SBP or Diagnosis
>90 DBP of HTN
Continue to Diagnosis Continue to Diagnosis
follow-up of HTN follow-up of HTN
Continue to
< 140 / 90 follow-up
Patients with high normal blood pressure (clinic SBP
130-139 and/or DBP 85-89) should be followed annually.Clinic, Home, Ambulatory (ABP) Blood
Pressure Measurement Equivalence Numbers
A clinic blood pressure of 140/90 mmHg has a
similar risk of a:
Description Blood Pressure mmHg
Home pressure average 135 / 85
Daytime average ABP 135 / 85
24-hour average ABP 130 / 80ABPM Indications Chughtai and Peixoto. Hosp Phys 2003
Contraindications to ABPM 1. Not cooperative 2. Severe PVD or thrombocytopenia 3. Afib (relative): not accurate 4. Arm too big 5. Severe office HTN (≈220/120)
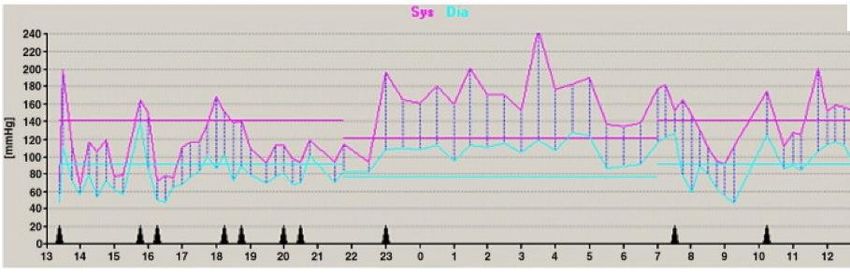
ABPM 1
ABPM 1
Information Provided by ABPM 1. Estimate of true overall 24 hour BP 2. Diurnal variation in BP 3. Variability in BP 4. Duration of action of drug
ABPM Normal Parameters
BP should dip by 10-20% during sleep
Chughtai and Peixoto. Hosp Phys 2003ABPM 2
ABPM 2
ABPM 3
ABPM 3
ABPM 4
ABPM: Number of Readings • Recommendation is at least 14 readings in the daytime (NICE Guidance). • Minimum number is 2 per hour. • We usually do a reading an hour at night.
ABPM 5
ABPM 5
ABPM 5 Ziemmsen. J Neurol Sci 2010
White Coat and Masked Hypertension
200
Home/Ambulatory SBP mmHg
180
Masked
Hypertension
Hypertension
160
140
135
120
Normotension White Coat
Hypertension
100
100 120 140 160 180 200
Office SBP mmHg
Derived from Pickering et al. Hypertension 2002: 40: 795-796Prognosis of Masked Hypertension
Prevalence of masked hypertension is approximately 10% in the general population but is
higher in patients with diabetes
J Hypertension 2007;25:2193-98Prognostic Significance of Clinic vs.
ABPM
Dawes. BP Monit 2006Prognostic Significance of Clinic vs.
ABPM
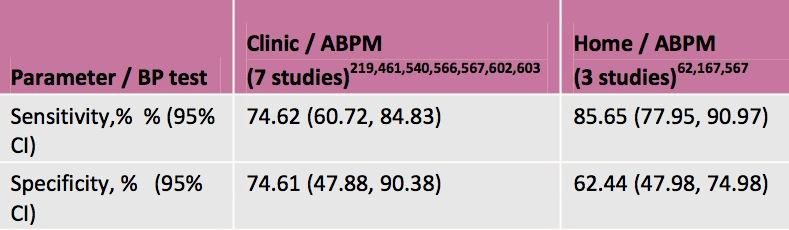
Dawes. BP Monit 2006Diagnostic Utility of BP Measures
NICE 2011 Guidance DocumentDiagnostic Utility of BP Measures
Hodgkinson. BMJ 2011Cost-Effectiveness of ABPM
Lovibond. Lancet 2011Diagnosis of Hypertension: Key
Points
• Non-automated office BP measurements are
not accurate.
• This results in inappropriate management.
• Out-of-office measurement – particularly
ABPM – should be used to confirm the
diagnosis of HTN.Bedtime Dosing of Antihypertensive Drugs
Predictive Role of Nighttime BP
Hansen. Hypertension 2012The MAPEC Trial
MAPEC Hypothesis: Bedtime chronotherapy leads to better BP control and reduces CV endpoints. Design: PROBE RCT Country: Spain Sample Size: 2156; mean age 56 Endpoints: 1. All-cause mortality and CVD events (huge composite endpoint) 2. 48-hour ABPM
MAPEC: Results Baseline awake systolic ABPM was 134 mm Hg. Baseline asleep systolic ABPM was 123 mm Hg.
MAPEC: Results
MAPEC Study: Issues • Inconsistent numbers presented across trial publications. Is this truly an RCT with a predefined start and end? Original sample size in the protocol was 3344. Subsequent publication mentions 734 normotensive subjects – uncertain if they are included in the main paper. • Most of the literature in the field comes from a single centre and one group of investigators. • Huge effect size from such a small, simple change.
Bottom Line: Bedtime Dosing • Practical point: relatively simple ‘intervention’ • Conversely, I don’t view the data as definitive yet. • I don’t routinely do it; however, I will in refractory hypertension. Also, in this group, I often use drugs that need bedtime dosing (alpha blockers and some CCBs).
Choice of ‘Thiazide’ Diuretic for
HTN
Chlorthalidone vs. HCTZPharmacologic Structure
• Chlorthalidone is often
mislabeled as ‘thiazide-
like’.
• It is a non-thiazide with a
distinct pharmacological
structure….
• ….that has similar
pharmacological action
(DCT NaCl symporter
blockade)
Kurtz. Hypertension 2012.Thiazides and Non-thiazides Thiazides Non-thiazides Hydrochlorothiazide Chlorthalidone Chlorothiazide Indapamide Methychlothiazide Metolazone Polythiazide Bendroflumethiazide
Pharmacokinetics
DRUG ONSET PEAK T1/2 (h) Duration (h)
(h)
HCTZ 2 4-6 6-9 (single) 12 (single)
8-15 (long 16-24 (long
term) term)
Chlorthalidone 2-3 2-6 40 (single) 24-48
45-60 (long (single)
term) 48-72 (long
term)
Carter BL. Hypertension 2004;43:4-9BP Control
• Meta-analysis of 108
HCTZ and 20
chlorthalidone studies
(n=10443)
• Comparisons are indirect,
not head-to-head
• Chlorthalidone is a more
Dose potent drug
Ernst, ME. Am J Hypertens. 2010MRFIT Trial Results
MRFIT. JAMA 1986Trial Results Trial Drug Result MRFIT Both + HDFP Chlorthalidone + ALLHAT Chlorthalidone + SHEP Chlorthalidone + Oslo BP HCTZ - MAPHY HCTZ - MRC HCTZ - Wing HCTZ - Amery HCTZ + MIDAS HCTZ + ANBP HCTZ + INSIGHT HCTZ + ACCOMPLISH HCTZ -
Diuretic Choice: Summary • Thiazides and non-thiazides are similar and dissimilar properties. • Chlorthalidone (non-thiazide) is more potent and can reduce BP more than HCTZ at equal doses. • Non-definitive ‘hard outcome’ indirect comparisons: ?chlorthalidone better
Diuretic Choice: Practical
Considerations
• Chlorthalidone: smallest dose available in Canada is 50 mg.
• Chlorthalidone: not commonly available in combos
(atenolol only). HCTZ: many combos
• If BP controlled on HCTZ, I don’t change. If I need to
choose a fixed dose combo with a diuretic, I use perindopril
indapamide or a HCTZ combo ($$ and coverage considered)
• In uncontrolled refractory hypertension, I will usually use
chlorthalidoneTreatment Target in Mild HTN
Treatment of Mild Hypertension
Treatment of Mild Hypertension
Treatment of Mild Hypertension
Primary Prevention Subjects with Mild HTN
Total events 77 vs 90: Nearly all from one study
Diao et al. Cochrane Collaboration 2013Comments on This Review
1. Essentially reflects one study (that used BB in
half the active treatment group)
2. Underpowered – study not designed to
specifically look at this subgroup.
Randomization not stratified for this subgroup.
3. The authors excluded relevant studies:
a) Non-placebo controlled studies (e.g., HDFP).
b) Didn’t have data for some studies (VA, Oslo, others)
but number of events for these would have been
smallMajor Trials Including Patients with Mild
Hypertension
Trial (n) Age Results for Primary Endpoint
BP (intervention vs. control)
MRC 35-64 Stroke events: 60 vs 109
17354 0.14 vs. 0.26 per 100 pt*y
5y 90-109 pMajor Trials Including Patients with
Mild Hypertension
Trial (n) Age Results for Primary Endpoint
BP (intervention vs. control)
HDFP 30-69 Total mortality: 231 vs. 291
7825 5.9% vs. 7.4%
90-104 stratum PHDFP Mortality RRR
HDFP. JAMA 1971Canadian Hypertension Education Program Recommendations For Initiating Drug Therapy 1. Prescribe for DBP ≥ 100 or SBP ≥ 160 (Grade A). 2. Strongly consider for DBP ≥ 90 and TOD or other CV risk factors (Grade A). 3. Strongly consider for SBP ≥ 140 and TOD (Grade C for mild HTN).
Major Trials Including Patients with Mild
Hypertension
Trial (n) Age Results for Primary Endpoint NNT over 1 year NNT over 10 y
BP (intervention vs. control)
MRC 35-64 Stroke events: 60 vs 109 4167 416
17354 0.14 vs. 0.26 per 100 pt*y
5y 90-109 pMajor Trials Including Patients with
Mild Hypertension
Trial (n) Age Results for Primary NNT over NNT over 10 y
BP Endpoint 1 year
(intervention vs. control)
HDFP 30-69 Total mortality: 231 vs. 291 333 33
subgroup 5.9% vs. 7.4%
7825 90-104 PHDFP Trial Alderman. Hypertension 1983
II. Indications for Pharmacotherapy
after diagnosis of hypertension (1)
• Patients at low risk with stage 1 hypertension (140-
159/90-99 mmHg)
– lifestyle modification can be the sole therapy.
• Patients with target organ damage (e.g. left
ventricular hypertrophy) (140-159/90-99 mmHg)
– Treat with pharmacotherapy
• Patients with chronic kidney disease should be
considered for pharmacotherapy if the blood pressure
is equal or over 140/90 mmHg
• Patients with diabetes should be considered for
pharmacotherapy if the blood pressure is equal or
over 140/90 mmHgII. Indications for Pharmacotherapy
after diagnosis of hypertension (2)
• Patients with other risk factors (over 90% of Canadians
with hypertension have other risk factors) (140-159/90-
99 mmHg despite lifestyle modification)
– Treat with pharmacotherapy
• Treatment Gap Alert: Many younger hypertensive
Canadians with multiple cardiovascular risks are
currently not treated with pharmacotherapy. Health care
professionals need to be aware of this important care
gap and recommend pharmacotherapy.Treatment of Mild Hypertension: Key
Points
1. All patients should be treated with lifestyle
modification.
2. Decision to institute drug treatment should
take into account global risk.Renal Denervation
Resistant Hypertension
• Failure to achieve BP target despite treatment
with three antihypertensive drugs (including a
diuretic) at optimal doses.
• Prevalence is not well studied. Appears to be
about 10-20% of hypertensive patients.
Sarafidis. J Clin Hypertens 2011Sympathectomy for Severe
Hypertension
Bilateral T8-L3
Sympathectomy
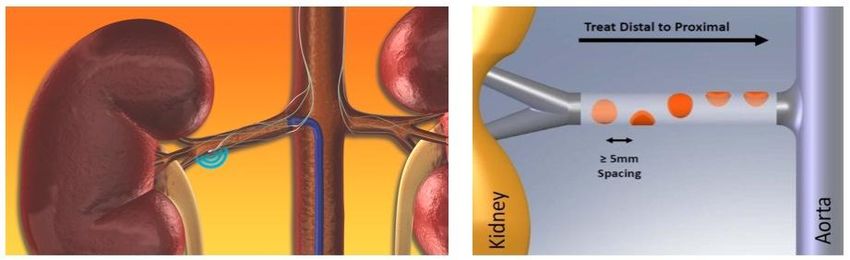
Ray BS. Ann Surg 1949Renal Sympathetic Denervation
Papademetriou et al. Int J Hypertens 2011Renal Sympathetic Denervation for Resistant
Hypertension
Source: Medtronic
73Renal Sympathetic Denervation for Resistant
Hypertension: SYMPLICITY HTN-2 RCT
6 month BP difference of 33/11
PRenal Sympathetic Denervation: Safety • Well tolerated – one femoral pseudoaneurysm was the only adverse effect. Renal function similar at end of six months. • Only half had ABPM measured; ABPM difference was 16/8 mm Hg between groups. • Irreversible nature of the procedure • Renal adverse effects? – Stenosis, dilation – Proteinuria – Renal function
Renal Sympathetic Denervation: Key Point • An emerging procedure • Potential to be used in a large number of patients • Long-term efficacy and safety data required.
Outline 1. Understand how to interpret ABPM. 2. Review the pros and cons of different methods to diagnose hypertension. 3. Discuss some current controversies in HTN management.
You can also read