A Primer for the Evaluation and Integration of Dietary Intake and Physical Activity Digital Measurement Tools into Nutrition and Dietetics Practice
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FROM THE ACADEMY
A Primer for the Evaluation and Integration of
Dietary Intake and Physical Activity Digital
Measurement Tools into Nutrition and Dietetics
Practice
Holly L. McClung, MS, RDN, LDN; Hollie A. Raynor, PhD, RDN; Stella L. Volpe, PhD, RDN, ACSM-CEP, FACSM; Johanna T. Dwyer, DSc, RD;
Constantina Papoutsakis, PhD, RD
BACKGROUND structure for the appropriate use of specific behaviors.14 The technology
technology is vital to provide effective should theoretically improve the effi-
T
HE RISING PREVALENCE OF
noncommunicable diseases nutrition care in the COVID-19 era.9 ciency and quality of data collection
(NCDs) is a global public health While taking into account Standards and facilitate attainment of all of these
concern.1,2 Unhealthy eating of Practice and Standards of Profes- goals, and yet many questions remain
habits and physical inactivity increase sional Performance,10,11 Registered Die- about their use and acceptability. For
the risk or severity of major NCDs titians and Nutritionists (RDNs) and example, because DI/PA assessment
such as obesity, coronary heart disease, Nutrition and Dietetics Technicians, methods are often criticized as being
diabetes mellitus, osteoarthritis, some Registered (NDTRs), are uniquely posi- inaccurate and imprecise, are the data
cancers, and depression.3-5 Primary tioned to play an active role in the from these new tools any more accu-
prevention or treatments to combat development, use, and evaluation of rate?15 Which tools are well-validated?
NCDs include the adoption of a healthy DI and PA related technology for Medi- Are there technologies that are avail-
diet without energy excess, routine cal Nutrition Therapy (MNT).12 This able and appropriate for different
physical activity, reducing sedentary type of work is part of the practice populations, such as those of different
time, and maintenance of a healthy area of nutrition informatics. ages or of different functional or
body weight.6 Technological innova- Today, health care providers can cognitive capacities? Who owns the
tions, such as digital measurement of transition from paper to digital-based individual’s or group’s data once
DI and PA, have become widely tools for many measurement tasks. aggregated? What are the ethical/reg-
accepted and are increasingly used to The explosion of mobile applications ulatory framework and steps needed to
assess and monitor lifestyle behavior. and wearables allows individual con- ensure anonymity and privacy? It is
Recently, the need for physical sumers to self-monitor their DI/PA, for important to be aware of these factors
distancing because of the outbreak of their own purposes or for sharing data when evaluating digital tools. A
the novel coronavirus (COVID-19), has with their providers for subsequent research priority of the Academy’s
revealed an additional urgent and dy- evaluation and feedback.12 In 2018, it Research International and Scientific
namic use of valid and reliable technol- was estimated that there were more Affairs team is to support utility and
ogy in health care. Providers aspire that than 160,000 mobile health applica- application of emerging technologies,
digital tools and telehealth platforms tions to track DI/ PA patterns, and over information management and knowl-
will help them to continue to provide $500 million was spent on these edge management, processes to inform
health care even when face-to-face in- applications.13 and advance nutrition and dietetics
teractions with clients are imprudent The possibilities are endless. Soft- programming and practice. In this pa-
or impossible. Delivering nutrition ware and application designers are per, the Academy’s Research Interna-
care in a framework of telenutrition focused on merging the needs of tional and Scientific Affairs Data
continues to grow as the health care diverse users, providers, and con- Science Center and the International
environment evolves and adapts.7,8 sumers. For clinical researchers, the Life Sciences Institute North America’s
However, whether increased demand potential of big data aggregation and (now the Institute for the Advance-
for telenutrition will be supported by data mining hold promise and excite- ment of Food and Nutrition Sciences)
insurance coverage remains to be ment in generating more accurate DI/ working group on dietary intake and
determined. Therefore, building a PA captures of “point-in-time” and in physical activity tools present essential
developing more viable interventions information and perspectives on digital
with long-term benefits. In contrast, dietary intake (DI)/physical activity
2212-2672/Copyright ª 2021 by the most consumers’ use of DI/PA technol- (PA) measurement tools. The goal is to
Academy of Nutrition and Dietetics. ogies is aimed at self-monitoring, provide emerging definitions used to
https://doi.org/10.1016/j.jand.2021.02.028
related to personal evaluation or describe digital technology in DI and
Available online xxx
awareness to maintain or change their PA measurement. Second, we describe
ª 2021 by the Academy of Nutrition and Dietetics. JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 1FROM THE ACADEMY
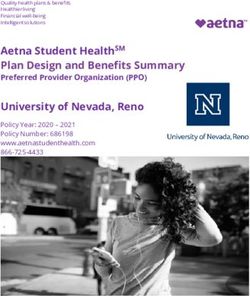
factors to consider when evaluating DI/ organizations in the field of digital require evidence and do not require
PA measurement technology products health: the Digital Medicine Society, regulatory oversight (Figure 2).17
as part of nutrition care. Finally, we Digital Therapeutics Alliance, HealthXL, Digital medicine is a subset of digital
delineate the outlook of digital DI/PA and Health Network of Digital Evidence health (Figure 2). The main difference
technology. in Health.17 The framework differenti- between digital health and digital
ates between products with different medicine is that digital medicine
levels of clinical evidence, and degree products must be backed by clinical
Definitions for Health Care of regulatory oversight. It classifies all evidence.17,19 Digital medicine products
Technology Measurement types of digital health tools in three are used for measurements or in-
Products major categories: digital health, digital terventions aiming at health promo-
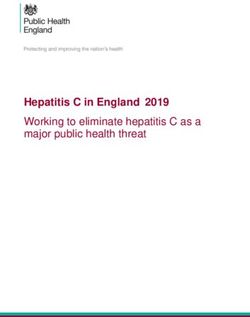
Many terms are used to describe the medicine, and digital therapeutics tion, disease prevention, treatment, or
intersection of health and technology. (Figure 2). recovery.
The World Health Organization has Digital health is very broad and in- Digital therapeutics is a subset of
provided a large and detailed taxon- cludes all categories of health technol- digital medicine (Figure 2), because not
omy of intervention terms for Digital ogy products such as mobile health all digital medicine products deliver an
Health.16 Terms and definitions tar- (mHealth), health information tech- intervention. Digital therapeutics is
geted to nutrition and dietetics pro- nology, wearables, telehealth, and defined as an evidence-based health
fessionals are provided below and in personalized health.18 This category of technology product that delivers a
Figure 1. products includes all applications that health intervention and has been
A good starting point is a consensus can be found in smart phone “app reviewed or certified by a regulatory
framework proposed by four stores.” Digital health products do not body (most commonly the Food and
Term Definition
Applications (apps) Mobile applications used on a smart phone, tablet, or computer
70
Connected products Mobile technologies, wearables, ingestibles, implantables, and portable technologies with
sensors for data collection
Devices71 A subset of lifestyle technology products with successful FDA approval for safety and
effectiveness
Digital health18 Health technology products that do not require validity or efficacy or regulatory oversight
Digital medicine19 Health technology products used for measurement/intervention that are supported by
evidence to demonstrate quality and validity
Digital therapeutics20 Evidence-based health technology products that deliver a health intervention and have been
reviewed or certified by a regulatory body
Health information Electronic medical records and related information systems
technology (HIT)72
Image-based assessment73 Tools that rely solely on images using a camera-enabled smart phone, tablet, or computer to
log food or activity
Image-assisted Use of images in combination with another assessment method (eg, photos to supplement a
assessment73 written record or to proceed an oral recall in the office)
Telehealth or Use of electronic information and telecommunication technologies to deliver and support long-
telemedicine74 distance clinical health care, patient- and professional health-related education, public health,
and health administration
Telenutrition74 The interactive use, by an RDN, of electronic information and telecommunication technologies
to implement the Nutrition Care Process with clients at a remote location (within provisions
of their state licensure)
Wearable technology General term for body-worn sensors capable of tracking location, time, environment, motion,
and certain body measures (eg, blood glucose, etc.)
Web-based assessment Tool requiring internet connection to log food or activity; often “cloud-based” data source
Figure 1. Health care technology measurement definitions. FDA ¼ Food and Drug Administration, RDN ¼ Registered Dietitian
Nutritionist.
2 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2021 Volume - Number -FROM THE ACADEMY
Data & informaon collecon,
storage and display
• User-facing technologies
Digital health All digital health products • HIT
Data & informaon
transmission
• Telehealth
Digital
medicine All digital health products used Measurement products
for measurement or • Electronic clinical outcomes
assessments
intervenon that are supported • Remote paent monitoring
by clinical evidence • Decision support soware
Digital
therapeucs
All digital health products used Soware that delivers a
therapeuc intervenon
for intervenon that are
Medical claims include:
supported by clinical evidence • Treat a disease
and are under regulatory • Manage a disease
oversight • Improve a health funcon
Figure 2. A Digital Health Framework; Adapted by the Data Science Center, Academy of Nutrition and Dietetics17. HIT ¼ Health
Information Technology.
Drug Administration [FDA]) for wearable products, and others make claims about the product’s
safety.17,20 (Figure 1). The definitions that follow intended use.22 Claims can cover dis-
explain frequently used terms. ease treatment (digital therapeutics
Evidence Supporting Digital and that deliver a medical intervention to
Therapeutic Medicine Product- Wearable Technology. “Wearable treat a disease), disease management
s. Clinical evidence is required that technology” is any electronic product (digital therapeutics that deliver a
demonstrates the products’ high qual- that can be worn as an accessory on the medical intervention to manage a dis-
ity and validity, for products to be user’s body, embedded in clothes, ease), or improving a health function
classified as digital medicine or thera- implanted, or tattooed on the skin, (digital therapeutics that deliver a
peutics. Thus, it is reasonable to ask: typically to track information related to medical intervention to improve a
What type, amount, and caliber of ev- health and fitness (Figure 1). Common health function or prevent a disease).
idence is required for a health tech- examples include step counters—smart
nology product to qualify as a digital jewelry such as rings, wristbands, Connected Products. Connected
medicine or therapeutic product? watches, or pins. Smaller wearable products are those with a real-world
There are no established or widely technology typically connects wire- function that are connected to the
agreed-on criteria. Nutrition and di- lessly with a smartphone application internet to transmit data or are
etetics professionals are encouraged to for display and interaction. This term is controlled remotely. This comprehen-
learn how and what digital tools to use not comprehensive because there are sive term includes mobile technologies,
and to conduct research demonstrating other technology products such as wearables, ingestibles, implantables,
how digital tools complement MNT and portable monitors, ingestibles, and so and portable technologies that have
improve health outcomes. These data forth that are not necessarily worn on sensors (Internet of Things) for the
are vital to support successful value- the body. collection of outcomes data (Figure 1).
based reimbursements, especially as Connected products can connect with
we navigate the COVID-19 era, in which Devices. “Device” is a “term of art,” each other and with other systems via
effective use of technology may be in- that is, a word with specific legal the internet, and they can share data
tegral in positive client outcomes and meaning used by the FDA. The term about themselves, their environment,
the future of the dietetics profession. device refers to a small subset of lifestyle and their users. The range of connected
Recently, an easy-to-administer tool on technology products approved by the products is ever expanding, from cars to
self-efficacy with using mobile health FDA for a specific intended function medical equipment (such as continuous
applications in dietetics practice was (Figure 1). Whether a product is a “de- glucose monitors), industrial machin-
validated.21 This tool may be a good vice” depends primarily on the prod- ery, and even packaging that is capable
place for the RDN to start a self- uct’s intended function as determined of reporting the location and condition
assessment exercise.21 A later section by the FDA’s Center for Drug Evaluation of packaged food or other commodities.
focuses on choosing the best connected and Research’s review process. A prod-
product, to provide guidance and uct may be called a device once it has
reasoning in the selection process. undergone successful FDA approval for Is There a Role for Connected
Digital technologies for DI/PA mea- safety and effectiveness. The FDA Products in Nutrition Care?
surements are frequently described by approval process is voluntary for man- Instead of episodic measures collected
the technology type used, and these ufacturers, but when it is successful, it at client visits, connected products
may include online websites, mobile works in the manufacturer’s best inter- provide the practitioner with longitu-
applications, camera-based tools, est, because then the manufacturer can dinal, and potentially more
-- 2021 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 3FROM THE ACADEMY
comprehensive, “real world” datasets loss interventions described the effi- monitoring adherence regardless of
for DI/PA, which the Clinical Trials cacy of self-monitoring on weight loss intervention tool used.
Transformation Initiative and other (primarily paper-based tools used).32 In More technological advances in di-
expert groups consider to be more that review, 22 studies were included, etary self-monitoring have occurred
valuable.23 Connected products may with 15 reporting on self-monitoring of since then. However, few researchers
create a digital virtual “twin” of the DI, one reporting on self-monitoring of have examined the efficacy of
client that captures data that histori- PA, and six reporting on self-weighing technology-based dietary self-
cally have been difficult to collect. and weight loss. For DI self- monitoring vs paper-based dietary
Intermittent collection of 24-hour di- monitoring, all 15 studies reported a self-monitoring on weight loss out-
etary recalls or food records provide significant relation between self- comes. Because self-monitoring with
single or only a few representations of monitoring and weight loss. Of the paper-based systems is known to have
DI, whereas a connected product may studies examined, four explored the flaws, it has often been assumed that
potentially record DI around the clock quality of DI self-monitoring that was real-time technology-based dietary
for long periods. Such around-the- associated with weight loss. More self-monitoring will address some is-
clock monitoring provides a more ac- comprehensive self-monitoring (ie, sues by invariably enhancing outcomes
curate picture of the targeted behavior captured more eating occasions compared with paper-based dietary
in the client’s life and greater aware- throughout the day) and regular self- self-monitoring.32,35 Therefore, there
ness of it. Conventional 24-hour dietary monitoring (ie, more days of the has been more research on which
recalls and food records are frequently week) was related to a greater weight components of technology-based di-
criticized for inaccuracy.24,25 Some loss.32 Related, Carels et al33 investi- etary tools should be used to enhance
studies suggest that data capture by gated self-monitoring of PA (paper- self-monitoring adherence and weight
digital means are more complete. For based) and also reported that greater loss outcomes. Mobile applications
example, an online 24-hour dietary self-monitoring was associated with provide various electronic forms and
recall (myfood24) for dietary assess- higher frequency of PA (r ¼ 0.52, P < interfaces to assist in logging DI (ie, text,
ment provided higher-quality DI data 0.01) and greater weight loss (r ¼ 0.44, photos) with capabilities to provide
than standard interviews when P < 0.05).33 multiple reports/summaries of intake
compared with biomarkers.26 Further- With respect to the integration of (ie, text, graphs). There is considerable
more, an electronic 12-hour dietary technology into lifestyle interventions, research on identifying which compo-
recall was superior in assessing DI than the impact on enhancing self- nents of the technology-enhanced
either a food frequency questionnaire monitoring of DI was directly exam- method are ideal for promoting self-
or 4-day food records.27 In energy ined within a 24-month weight loss monitoring.36 For example, Dunn and
expenditure, the reference standard trial.34 Paper-based self-monitoring colleagues37 examined a mobile photo
method is indirect calorimetry, which was compared with self-monitoring on dietary self-monitoring application to a
is not easy to use routinely in clinical a personal digital assistant (PDA) in 210 calorie tracking DI self-monitoring
care. Also, with inpatient energy esti- adults. Although the PDA was not application on self-monitoring fre-
mates using visual estimation of food connected to the internet, the Dietmate quency and weight loss in 41 adults
amounts eaten, there is a high proba- Pro software had automated capabil- receiving a remotely delivered 6-month
bility for human error. There are ities to calculate DI for energy and nu- lifestyle intervention.37 Outcomes were
different validated connected products trients consumed for point-in-time similar between the tools used over the
that provide a practical alternative to diet self-monitoring. Investigators number of days the diet was logged
indirect calorimetry and inpatient en- compared three conditions, paper di- (defined as logging at least one food or
ergy estimates for different pop- ary, PDA, and PDAþfeedback (FB). In beverage item). Overall, reported log-
ulations.28-31 PDAþFB, additional feedback software ging was low across all participants
was used to interact with Dietmate Pro (FROM THE ACADEMY
- Accuracy
— Validation studies (technical, clinical, systems)
- Intended use
— Measurement of the desired variable
— Appropriate for length time
— Automation as required
— Flexibility across platforms
- Target population
— Cultural acceptability
— Age group (acceptability and feasibility, and level of interest)
— Related conditions that can influence usability or benefit (clinical suitability)
— Literacy and numeracy skills
- Cost (in relation to system, client, value-based reimbursement)
- Ease of use (user experience or UX)
— User friendly
— Easy access
— Use across technology platforms
— App features can be tailored
— App offers a platform for health care professionals to access data (this provides a way to track, observe,
facilitate engagement) (two-way communication)
- Transparent data use, ownership, and privacy
Client uses the app effectively!
DI/PA data are informative and actionable
Generated data contribute to improving behavior change, care, and practice patterns
Safe experience
(continued on next page)
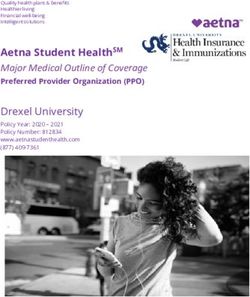
Figure 3. Important factors for RDNs/NDTRs to consider when selecting an app and desirable outcomes. DI/PA ¼ Dietary intake/
physical activity.
Similar to the situation with DI self- of wearable activity trackers on adher- monitor that was not a pedometer (ie,
monitoring, research is lacking to ence. Eighteen studies with middle- measured vertical acceleration move-
examine the efficacy of technology- aged and older participants reported ment while providing feedback), and
based as compared with paper-based greater weight loss outcomes when an outcomes of PA or weight had to be
PA self-monitoring on weight loss out- activity tracker was part of a weight reported at 3 months or later.39
comes.38-41 A systematic review pub- loss program.42 Three studies with Comparative conditions included inac-
lished in 2018 examined the effect of younger adults did not find this rela- tive (no active intervention) and active
wearable activity trackers on adher- tionship.42 Thus, the authors concluded interventions. Unfortunately, adher-
ence and weight loss outcomes when that short-term (55 years) corroborates mate indicated a small, statistically
ture for weight loss. Studies varied improvement of PA in the short term significant effect, in which wearable
greatly; some included programs when using a PA mobile application.43 activity monitors increased PA (stan-
without PA goals, others had programs A 2017 meta-analysis examined the dardized mean difference ¼ 0.26; 95%
that only focused on PA, and some had effects of wearable activity monitors on confidence interval [CI] ¼ 0.04e0.49).
no intervention at all. Because of improving PA and weight-related out- For weight loss, the pooled estimate
incongruent methods of tracking attri- comes. Included studies were ran- also indicated a small, statistically sig-
tion, the authors could not make domized controlled trials in which one nificant effect (mean
overall conclusions regarding the effect condition used a wearable activity difference ¼ 1.65 kg; 95% CI ¼ 3.03
-- 2021 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 5FROM THE ACADEMY
Client uses the app effectively!
DI/PA data are informative and actionable
Generated data contribute to improving behavior change, care, and
practice patterns
Safe experience
▪ Accuracy
-Validation studies (technical, clinical, systems)
▪ Intended use
-Measurement of the desired variable
-Appropriate for length time
-Automation as required
-Flexibility across platforms
▪ Target population
-Cultural acceptability
-Age group (acceptability and feasibility, and level of
interest)
-Related conditions that can influence usability or benefit
(clinical suitability)
-Literacy and numeracy skills
▪ Cost (in relation to system, client, value-based
reimbursement)
▪ Ease of use (User Experience or UX)
-User friendly
-Easy access
-Use across technology platforms
-App features can be tailored
-App offers a platform for healthcare professionals
to access data (this provides a way to track, observe,
facilitate engagement) (two-way communication)
▪ Transparent data use, ownership and privacy
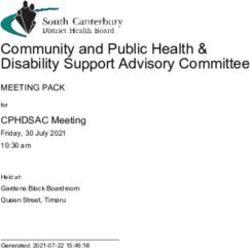
Figure 3. (continued) Important factors for RDNs/NDTRs to consider when selecting an app and desirable outcomes. DI/PA ¼ Di-
etary intake/physical activity.
to 0.28). These results, combined kind of technology-based self-moni- particular circumstances of use. In the
with the results of the 2018 systematic toring would be optimal. Beyond client selection process, three key factors
review by Cheatham et al,42 support preference, another important factor for should be considered: level of accuracy
that wearable activity trackers can be practitioners to consider regarding self- required (eg, research- or client-
helpful for weight loss, but the effect monitoring is whether the self- focused need); intended use (eg, base-
sizes are rather small.39,42 monitoring strategy tracks the area in line assessment, intervention moni-
Taken together, research in this area which goals have been set. For example, toring, and so forth); and target
suggests that self-monitoring of DI/PA is if the goal is focused on increased fruit population (Figure 3).15 However, even
related to weight loss outcomes, when and vegetable intake, then the tool must with these factors in play, settling on
self-monitoring is a component of a be able to track cups of fruit and vege- the “right-fit” DI/PA technology to
weight loss intervention. What is not table intake as an output. Although provide real value to the RDN and
clear at this time is whether paper-based self-monitoring can be client can be a challenge among the
technology-based self-monitoring, easily adapted to goals, not all cluttered landscape of new
compared with paper-based self-moni- technology-based self-monitoring tools technologies.
toring, enhances efficacy of provider- have the capability to track all DI or PA In 2019, Eldridge et al44 led an expert
led obesity treatment programs, and goals and may not be adaptable to all group to review 43 new DI assessment
what type of technology-based self- potential goals. This requires the prac- technologies aimed to provide guide-
monitoring might enhance outcomes. titioner to be familiar with a variety of line criteria for future tool assessments
In practice, what is important to recog- tools to “custom-fit” to the client and and offer standardized reporting rec-
nize is that self-monitoring of DI/PA the client’s outcome goals throughout ommendations.44 This report compares
enhances treatment efficacy. Which the phases of treatment. and contrasts between research- and
type of self-monitoring enhances consumer-designed technologies (re-
treatment efficacy is not clear. Thus, ported in literature from 2011 to 2017)
factoring in individualized client pref- Selecting the Best-Connected over 25 attributes for evaluation,
erence for type of self-monitoring, pa- Product including methods to validate the
per-based vs technology-based is The process of selecting a technology technologies (eg, energy intake
important. If technology-based self- or tool that fits best should focus on compared with total energy expendi-
monitoring is preferred, RDNs are user or provider preferences and limi- ture from doubly labeled water or
encouraged to carefully evaluate what tation of barriers that are unique to the traditional dietary assessment).
6 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2021 Volume - Number -FROM THE ACADEMY Validation studies were more likely to show promise in specific age groups, or technology will be used by a client. An be reported for research-facing DI over particular spans of time, and some application or technology used for a technologies than those targeted to are considered accurate under only short-term baseline assessment may consumers.44 This raises the question specific activities.49 For example, a warrant different standards and effi- about what preferences are the focus systematic review of 67 studies ciency from a technology to be used for when selecting a technology—is the compared use of Fitbit vs a research- long-term or regular monitoring for “fit” provider- or user-based? A recent standard criterion and consistently maintenance care or intervention. study surveyed 1,001 international found that Fitbit devices were only Automation of DI or PA logged activities health professionals (eg, RDNs, nurses, likely to be accurate for step count 50% by the user into useful numerical and physicians) of which approxi- of the time when used in an adult values for assessment and feedback by mately 45% (of these, 50% were RDNs) population.50 Findings suggest that the provider may be preferred over had previously recommended DI Fitbit has a tendency to underestimate longer use periods because of the sheer application use to clients.45 The pri- steps in a controlled setting and over- amount of data collected.52,53 Another mary factors influencing DI application estimate in a free-living setting. Addi- area to evaluate is the flexibility of a choice by providers were ease of use tionally, Fitbit is not likely to provide technology across platforms (eg, (87%), free of charge (73%), and vali- accurate measures for total energy Android vs iOS) to allow compatibility dated technology (69%). Providing a expenditure under any condition, but it with a user’s mobile device. With this, client with new technology that is user- provides a measure similar to acceler- the provider must have a detailed un- friendly and easy to access on the cli- ometers to capture the amount of time derstanding of how personal data will ent’s personal device is key to pro- spent doing lower-intensity activities, be stored and shared (with the pro- moting long-term use and acceptance such as sitting or sleeping. vider and across the software in self-monitoring. Both are relatively A common thread evident designer). Ideally, an open access soft- easy for the provider to determine, but throughout current DI/PA technology ware platform and structure allows finding a valid and trusted connected measurement research is the lack of insight as to data use and privacy. Some product is a much more complex issue standardization and transparency in current technology and applications for the provider. the validation process. In the United available have research-grade options Digital health technologies require a Kingdom, a consortium has been of the software available for use in a robust and transparent validation pro- established among the technology in- private setting, with user-defined con- cess that should encompass three do- dustry, researchers, clinicians, and trols in output and data ownership.44 mains: technical (eg, how accurately regulatory agencies to provide users Mobile devices with health applica- does the tool measure?), clinical (eg, and health care providers with a library tions create new opportunities and does the tool have support to improve of currently available and validated risks to the user and provider or health-specific outcomes?), and sys- health applications. The National researcher. More data than ever are tems (eg, does the tool integrate into a Health System Apps Library is the collected in a streamlined and simpli- client’s life, provider workflow, and largest health website in the United fied process from smartphone hard- health care system?).46 Few research- Kingdom with a section specifically ware and sensors, and then with the based technologies provide informa- devoted to reviewing applications.51 addition of secondary mobile devices tion on technical validity with respect The National Health System Apps Li- to expand the platform to application- to data accuracy and software limita- brary currently features approximately navigated health devices (eg, glucose tions, and even fewer provide infor- 100 applications that have been vali- meters, heart rate monitors, pulse ox- mation to support clinical and system dated by experts from technology, imetry, and others).54 Applications that validation.47 New technologies and health care, and policy backgrounds. can be tailored to the client’s needs or tools in DI/PA assessment show close Application developers self-nominate allow two-way data flow between agreement to traditional methods, but their technology to be featured in this provider and client may result in wider gaps are evident when they are library by completing an assessment improved outcomes.55 Data sharing compared with more objective mea- that covers national standards, regula- requires clients to opt in so that the sures (eg, total energy expenditure tions, and industry best practices to provider has ongoing access. Applica- from doubly labeled water).44 Current gauge how the technology performs tions that come with platforms for DI technology validation research fo- against important criteria. The greater providers facilitate two-way commu- cuses on comparisons with traditional the effectiveness potential of the nication, provide a benefit of seamless DI assessment methods (eg, 24-hour application, the more complex the monitoring, and support engagement recalls, food records, food frequency assessment. A similar trusted peer- between provider and client. Research questionnaires, and so forth).48 Ideally, reviewed resource in the United conducted using many new health in the future, developers and re- States would be highly beneficial and is monitoring technologies is “unregu- searchers will include more objective sorely needed. lated,” meaning it is not covered by criteria measures (eg, doubly labeled The intended use of a technology federal research regulations and is not water, biomarkers, and so forth) to needs to be strongly considered before referred to an Institutional Review compare new technologies and publish down-selection of the “right-fit” tool Board, unless the technology has been the detailed evaluation of validity by the provider. Consideration must be approved as an FDA device. The regu- work.15,45 A handful of technologies given to the length of time the latory oversight of connected products -- 2021 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 7
FROM THE ACADEMY is evolving. Since the 21st Century et al59; and for older adults, Takemoto likely do not pose overt health risks by Cures Act,56 the specific role and et al.60 Because of the growing number miscalculation in the measurements involvement of the FDA is being more of older adults seeking DI/PA in- themselves. However, a systematic re- rigorously explored.57 terventions, we describe here many view of 46 applications calculating in- There is concern that widely used barriers that might be encountered; sulin dosing by leveraging data from technologies in “unregulated” research others also may be pertinent. In- planned carbohydrate intake among are unethical, result in low-quality dividuals with vision problems may persons with diabetes mellitus showed data, and are possibly exposing partic- find it difficult to see the small screens that two-thirds of them calculate ipants to harms ranging from privacy on mobile devices such as smartphones incorrect insulin doses.63 Such erro- violations to psychological and physical and smartwatches. Physical limitations neous measurements may put in- injury.58 Extending federal research such as arthritis, tremor, and other dividuals at health risk for suboptimal regulations to cover all research with tactile problems may make it difficult glucose management or other unde- human participants would be the most to touch and activate screens or keys sirable health consequences. RDNs are effective way to address the issue. successfully. Few devices have audio uniquely positioned to counsel clients However, this may not be a viable op- options that can overcome this limita- appropriately to ensure the choice of tion in the immediate future. There- tion. Cognitive deficits may make re- tools is a good fit for the health prob- fore, recommendations to protect cord keeping difficult or impossible. lem in question and specific to the clients include best practice measures Data interpretation and acceptability client. monitored by government (state and barriers in addition to habits and po- federal), the technology industry itself tential lack of economic resources may (application designers), and re- lead some older individuals to not Digital Technologies as Adjuncts searchers to include education, owning personal mobile devices or to Nutrition Care consultation, transparency, self- computers, or if they do, they may not Digital technologies are adjuncts to, governance, and regulations to cover use them often.60 rather than substitutes for, the effort of basic research ethics.58 RDNs in crafting effective behavior A favorable user experience change programs involving nutrition (frequently abbreviated as UX) has the Unintended Health care.64 RDNs may match clients with potential to improve overall usability of Consequences tools that are a valid, reliable, and the application. Providers should look There are unintended health conse- acceptable fit. RDNs are health care for products that provide ease of use quences in using digital technologies professionals who synthesize DI/PA and have been developed in accor- that need to be considered. For data, with other important and rele- dance with industry UX standards. A example, tracking applications have vant variables identified in nutrition key consideration in selecting technol- been reported to intensify behaviors assessment, to prioritize and address ogies for use is matching the target related to disordered eating. In a recent effectively their clients’ nutrition population to the intended tool. study, self-use of energy consumption problems.65,66 For example, step coun- Choosing a technology that “fits” both tracking applications were associated ters and digital reminders are useful the user and provider not only provides with disordered eating patterns such as adjuncts to a weight loss program that a more valuable output; it is instru- increased eating concern, and dietary includes group meetings, weigh-ins, or mental in the longevity of technology restraint, but not with shape and nutrition counseling. If the rest of the use and potential to impact the health weight concerns.61 Thus, individuals program is abandoned, effectiveness outcomes of the client. Cultural using energy tracking applications may may be lost. As trained professionals, acceptability must be considered so be doing so for reasons unrelated to RDNs/NDTRs leveraging their expertise that food items and activities align well body satisfaction. In the same study, PA and critical reasoning to design/select/ with the target population. Clinical tracking was related to eating disorder use technology to track and improve suitability is also important. When symptomatology, which may be of clients’ DI/PA are necessary to achieve working with clients with disordered concern. Use of Instagram, a photo and health outcomes for clients.67 In a eating or body image disturbances, it video-sharing social media platform, recent international survey on the use may be important for the application to was associated with orthorexia nerv- of diet applications in health care that allow a provider to “turn off” numerical osa, a behavior characterized by the invited providers to participate, 833 values to the user while the clinician obsessive pursuit of eating a healthy dietitians from 73 countries reported uses them for tracking DI/PA to aid in diet.62 Although the literature is quite application usage and experiences in interventions.45 It is also important to limited, available results suggest that, provision of care, and this comprised consider acceptability and feasibility for some people, connected products more than 80% of the survey sample. when dealing with young children, may exacerbate propensity to disor- Physicians and nurses ranked next in older adults, or those with limited lit- dered eating behaviors. frequency participation (in the range of eracy and numeracy skills. There are Health-related harm also may be 6% to 7% each).45 Nutrition and di- several factors to consider in these involved when the measurement of a etetics professionals around the world populations. For a full discussion on connected product is not accurate, are learning, using, and applying DI/PA modern considerations in a pediatric potentially jeopardizing health. In applications to best reap the benefits population, refer to Spruijt-Metz general, DI/PA connected products for clients.68 It will be important to 8 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2021 Volume - Number -
FROM THE ACADEMY
study the use of applications in attention is needed to applying dietitian nutritionists. J Acad Nutr Diet.
2018;118(1):132-140.
measuring DI/PA with and without the behavior change theory in technology
facilitation of trained providers (ie, development. Digital measurement 11. Academy of Nutrition and Dietetics.
Revised 2017 standards of practice in
RDNs/NDTRs) to understand the dif- tools also need to be using more plain nutrition care and standards of profes-
ferences and potentially emerging language and reflect health literacy, sional performance for nutrition and
consequences in health outcomes. especially when it comes to any dietetics technicians, registered. J Acad
Nutr Diet. 2018;118(2):317-326.
messaging that is provided so that
12. Hamideh D, Arellano B, Topol EJ,
OUTLOOK/CONCLUSION different target populations benefit in Steinhubl SR. Your digital nutritionist.
an inclusive fashion. Integrating tech- Lancet. 2019;393(10166):19.
The growth of digital health DI/PA
nology into routine nutrition care, and 13. Grundy QH, Wang Z, Bero LA. Challenges
technologies is exponential. Health
showing related efficacy, may be the in assessing mobile health app quality: a
care providers must keep pace with systematic review of prevalent and inno-
way forward for successful value-based
new methods and tools, because vative methods. Am J Prev Med.
reimbursements, especially as we 2016;51(6):1051-1059.
increasing evidence suggests that self-
navigate in the COVID-19 era.64 14. Burrows TL, Rollo ME. Advancement in
monitoring improves health outcomes
dietary assessment and self-monitoring
across noncommunicable diseases. References using technology. Nutrients.
New technologies offer the potential to 1. Mozaffarian D, Benjamin EJ, Go AS, et al. 2019;11(7).
monitor DI/PA over longer periods with Heart disease and stroke statistics—2015 15. McClung HL, Ptomey LT, Shook RP, et al.
more efficiency and potentially greater update: a report from the American Heart Dietary intake and physical activity
Association. Circulation. 2015;131(4):e29- assessment: current tools, techniques,
impact. Providers’ goals should be, first, e322. and technologies for use in adult pop-
to provide clients individualized tools 2. Pescatello LS, MacDonald HV, Lamberti L, ulations. Am J Prev Med. 2018;55(4):e93-
and methods that are valid, reliable, Johnson BT. Exercise for hypertension: a e104.
acceptable, and second, to help them prescription update integrating existing 16. World Health Organization. Classification
recommendations with emerging of Digital Health Interventions v1. 0: A
use the tools appropriately as part of an research. Curr Hypertens Rep. Shared Language to Describe the Uses of
MNT plan of care. However, the current 2015;17(11):87. Digital Technology for Health. World
state of the DI/PA technologies lack 3. Dietz WH, Douglas CE, Brownson RC. Health Organization; 2018.
standardization and transparency in Chronic disease prevention: tobacco
17. Goldsack J, Coder M, Fitzgerald C, Navar-
avoidance, physical activity, and nutrition
validation, privacy, and sharing of data. for a healthy start. JAMA. 2016;316(16):
Mattingly N, Coravos A, Atreja A. Digital
Together with other health care pro- health, digital medicine, digital thera-
1645-1646.
peutics (DTx): what’s the difference?
viders, we need to insist on improve- 4. Penninx BW, Leveille S, Ferrucci L, van 2019. Medium. https://medium.com/digital-
ment in the regulation of health Eijk JT, Guralnik JM. Exploring the effect medicine-society-dime/digital-health-digital-
of depression on physical disability: lon- medicine-digital-therapeutics-dtx-whats-
technologies to protect our clients and gitudinal evidence from the established the-difference-92344420c4d5. Accessed
advance the nutrition and dietetics populations for epidemiologic studies of February 4, 2020.
profession. The future of DI/PA tech- the elderly. Am J Public Health.
1999;89(9):1346-1352. 18. U.S. Food and Drug Administration. Digi-
nologies would benefit from a “health- tal Health. 2020. https://www.fda.gov/
centered design,” an approach that 5. Scarmeas N, Luchsinger JA, Schupf N, et al. medical-devices/digital-health. Accessed
Physical activity, diet, and risk of Alz- February 25, 2020.
would function to bridge the gap be- heimer disease. JAMA. 2009;302(6):627-
tween provider/client wants and de- 637. 19. Goldsack J. Laying the foundation:
defining digital medicine. Medium. 2019.
velopers’ products.69 In addition, 6. Arena R, Guazzi M, Lianov L, et al. Healthy https://medium.com/digital-medicine-
“people-centered design” is needed lifestyle interventions to combat non- s o c i e t y - dime/laying-the-foundation-
communicable disease: a novel nonhier- defining-digital-medicine-49ab7b6ab6ef.
where products are developed, tested, archical connectivity model for key Accessed February 25, 2020.
and updated with both providers and stakeholders: a policy statement from the
American Heart Association, European 20. Digital Therapeutics Alliance. Digital ther-
clients in mind (and with input from apeutics: how they relate to digital health.
Society of Cardiology, European Associa-
these audiences). Such an approach tion for Cardiovascular Prevention and https://dtxalliance.org/wp-content/uploads/
would engage providers, clients, and Rehabilitation, and American College of 2019/05/DTA_TheDigitalHealthLandscape.
Preventive Medicine. Eur Heart J. pdf. Accessed September 24, 2020.
application/device designers
2015;36(31):2097-2109. 21. Chen J, Allman-Farinelli M. Development
throughout the technology product
7. Peregrin T. Telehealth is transforming and validation of a tool to measure di-
development and gracefully integrate health care: what you need to know to etitians’ self-efficacy with using mobile
technology into routine health care. A practice telenutrition. J Acad Nutr Diet. health apps in dietetic practice. J Nutr
comprehensive electronic platform 2019;119(11):1916-1920. Educ Behav. 2018;50(5):468-475.
that rigorously evaluates available DI/ 8. Ventura Marra M, Lilly CL, Nelson KR, 22. U.S. Food and Drug Administration. De-
Woofter DR, Malone J. A pilot randomized vice Classification Under Section
PA applications in real time is a much- controlled trial of a telenutrition weight 513(f)(2)(De Novo). https://www.
needed resource. Overall, RDNs/NDTRs loss intervention in middle-aged and accessdata.fda.gov/scripts/cdrh/cfdocs/
and other health care professionals older men with multiple risk factors for cfpmn/denovo.cfm?ID¼DEN180044.
cardiovascular disease. Nutrients. Accessed April 13, 2019.
must work to align and improve the 2019;11(2).
design of technologies to not just assist 23. Clinical Trials Transformation Initiative.
9. Mehta P, Stahl MG, Germone MM, et al. Recommendations Executive Summary:
but optimize nutrition care across the Telehealth and nutrition support during Advancing the Use of Mobile Technologies
board. Future technology will benefit the COVID-19 pandemic. J Acad Nutr Diet. for Data Capture & Improved Clinical Trials.
2020;120(12):1953-1957. In: Clinical Trials Transformation Initiative,
from greater engagement among de-
10. Academy of Nutrition and Dietetics. ed, 2021. https://www.ctti-clinicaltrials.
velopers, RDNs/NDTRs, or targeted pa- org/sites/www.ctti-clinicaltrials.org/files/
Revised 2017 Standards of practice in
tient groups to improve UX (user nutrition care and standards of profes- mobile-technologies-executive-summary.
experience) and usability. More sional performance for registered pdf. Accessed March 29, 2021.
-- 2021 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 9FROM THE ACADEMY
24. Archer E. The use of implausible data calorie tracking but not through a digital 51. National Health System. NHS Apps Li-
without caveats is misleading. Am J Clin photography app is associated with sig- brary. NHS. https://www.nhs.uk/apps-
Nutr. 2017;106(3):949-950. nificant weight loss: the 2SMART pilot library/. Accessed August 14, 2020.
25. Subar AF, Freedman LS, Tooze JA, et al. study—a 6-month randomized trial. J Acad 52. American Medical Association. 2019 CPT
Addressing current criticism regarding Nutr Diet. 2019;119(9):1525-1532. codes offer new paths to payments for
the value of self-report dietary data. 38. Bravata DM, Smith-Spangler C, digital medicine. https://www.ama-assn.
J Nutr. 2015;145(12):2639-2645. Sundaram V, et al. Using pedometers to org/practice-management/cpt/2019-cpt-
26. Wark PA, Hardie LJ, Frost GS, et al. Validity increase physical activity and improve codes-offer-new-paths-payment-digital-
of an online 24-h recall tool (myfood24) health: a systematic review. JAMA. medicine. Accessed August 27, 2020.
for dietary assessment in population 2007;298(19):2296-2304.
53. American Medical Association. AMA
studies: comparison with biomarkers and 39. Goode AP, Hall KS, Batch BC, et al. The Release 2020 CPT code set. http://www.
standard interviews. BMC Med. impact of interventions that integrate ama-assn.org/press-center/press-releases/
2018;16(1):136. accelerometers on physical activity and ama-releases-2020-cpt-code-set. Accessed
27. Bejar LM, Reyes OA, Garcia-Perea MD. weight loss: a systematic review. Ann August 27, 2020.
Electronic 12-hour dietary recall (e- Behav Med. 2017;51(1):79-93.
54. Nebeker C. mHealth research applied to
12HR): comparison of a mobile phone app 40. Lewis ZH, Lyons EJ, Jarvis JM, Baillargeon J. regulated and unregulated behavioral
for dietary intake assessment with a food Using an electronic activity monitor sys- health sciences. J Law Med Ethics.
frequency questionnaire and four dietary tem as an intervention modality: a sys- 2020;48(1_suppl):49-59.
records. JMIR Mhealth Uhealth. 2018;6(6). tematic review. BMC Public Health.
55. Huang Z, Lum E, Jimenez G, Semwal M,
2018;e10409. 2015;15:585.
Sloot P, Car J. Medication management
28. Elbelt U, Haas V, Hofmann T, et al. Eval- 41. Richardson CR, Newton TL, Abraham JJ, support in diabetes: a systematic assess-
uation of a portable armband device to Sen A, Jimbo M, Swartz AM. A meta- ment of diabetes self-management apps.
assess resting energy expenditure in pa- analysis of pedometer-based walking in- BMC Med. 2019;17(1):127.
tients with anorexia nervosa. Nutr Clin terventions and weight loss. Ann Fam
56. Kesselheim AS, Avorn J. New “21st cen-
Pract. 2016;31(3):362-367. Med. 2008;6(1):69-77.
tury cures” legislation: speed and ease vs
29. Hughes MJ, Harrison EM, Wigmore SJ. 42. Cheatham SW, Stull KR, Fantigrassi M, science. JAMA. 2017;317(6):581-582.
Energy expenditure after liver resection: Motel I. The efficacy of wearable activity
57. Kasperbauer TJ, Wright DE. Expanded
validation of a mobile device for esti- tracking technology as part of a weight
FDA regulation of health and wellness
mating resting energy expenditure and loss program: a systematic review.
apps. Bioethics. 2020;34(3):235-241.
an investigation of energy expenditure J Sports Med Phys Fitness. 2018;58(4):534-
change after liver resection. JPEN J 548. 58. Rothstein MA, Wilbanks JT, Beskow LM,
Parenter Enteral Nutr. 2017;41(5):766- et al. Unregulated health research using
43. Sohaib Aslam A, van Luenen S, Aslam S,
775. mobile devices: ethical considerations
van Bodegom D, Chavannes NH.
and policy recommendations. J Law Med
30. Koehler K, Drenowatz C. Monitoring en- A systematic review on the use of
Ethics. 2020;48(1_suppl):196-226.
ergy expenditure using a multi-sensor mHealth to increase physical activity in
device-applications and limitations of older people. Clin eHealth. 2020;3:31-39. 59. Spruijt-Metz D, Wen CKF, Bell BM,
the sensewear armband in athletic pop- Intille S, Huang JS, Baranowski T. Ad-
44. Eldridge AL, Piernas C, Illner AK, et al.
ulations. Front Physiol. 2017;8:983. vances and controversies in diet and
Evaluation of new technology-based tools
physical activity measurement in youth.
31. Ofei KT, Mikkelsen BE, Scheller RA. Vali- for dietary intake assessment: an ILSI
Am J Prev Med. 2018;55(4):e81-e91.
dation of a novel image-weighed tech- Europe dietary intake and exposure task
nique for monitoring food intake and force evaluation. Nutrients. 2018;11(1): 60. Takemoto M, Manini TM, Rosenberg DE,
estimation of portion size in hospital 55. et al. Diet and activity assessments and
settings: a pilot study. Public Health Nutr. 45. Vasiloglou MF, Christodoulidis S, Reber E, interventions using technology in older
2019;22(7):1203-1208. et al. What healthcare professionals think adults. Am J Prev Med. 2018;55(4):e105-
32. Burke LE, Wang J, Sevick MA. Self-moni- of “nutrition & diet” apps: an interna- e115.
toring in weight loss: a systematic review tional survey. Nutrients. 2020;12(8):2214. 61. Simpson CC, Mazzeo SE. Calorie count-
of the literature. J Am Diet Assoc. 46. Mathews SC, McShea MJ, Hanley CL, ing and fitness tracking technology: as-
2011;111(1):92-102. Ravitz A, Labrique AB, Cohen AB. Digital sociations with eating disorder
33. Carels RA, Darby LA, Rydin S, health: a path to validation. NPJ Digit Med. symptomatology. Eat Behav. 2017;26:
Douglass OM, Cacciapaglia HM, 2019;2:38. 89-92.
O’Brien WH. The relationship between 47. Chen J, Bauman A, Allman-Farinelli M. 62. Turner PG, Lefevre CE. Instagram use is
self-monitoring, outcome expectancies, A study to determine the most popular linked to increased symptoms of orthor-
difficulties with eating and exercise, and lifestyle smartphone applications and exia nervosa. Eat Weight Disord.
physical activity and weight loss treat- willingness of the public to share their 2017;22(2):277-284.
ment outcomes. Ann Behav Med. personal data for health research. Telemed 63. Huckvale K, Adomaviciute S, Prieto JT,
2005;30(3):182-190. J E Health. 2016;22(8):655-665. Leow MK, Car J. Smartphone apps for
34. Burke LE, Styn MA, Sereika SM, et al. Us- 48. Ferrara G, Kim J, Lin S, Hua J, Seto E. calculating insulin dose: a systematic
ing mHealth technology to enhance self- A focused review of smartphone diet- assessment. BMC Med. 2015;13:106.
monitoring for weight loss: a random- tracking apps: usability, functionality, 64. Barnett J, Harricharan M, Fletcher D,
ized trial. Am J Prev Med. 2012;43(1):20- coherence with behavior change theory, Gilchrist B, Coughlan J. myPace: an inte-
26. and comparative validity of nutrient grative health platform for supporting
35. Burke LE, Sereika SM, Music E, intake and energy estimates. JMIR weight loss and maintenance behaviors.
Warziski M, Styn MA, Stone A. Using Mhealth Uhealth. 2019;7(5). IEEE J Biomed Health Inform. 2015;19(1):
instrumented paper diaries to document 2019;e9232. 109-116.
self-monitoring patterns in weight loss. 49. Wellard-Cole L, Chen J, Davies A, et al. 65. Lewis SL, Wright L, Arikawa AY,
Contemp Clin Trials. 2008;29(2):182-193. Relative validity of the eat and track (EaT) Papoutsakis C. Etiology intervention link
36. Mandracchia F, Llaurado E, Tarro L, et al. smartphone app for collection of dietary predicts resolution of nutrition diagnosis:
Potential use of mobile phone applica- intake data in 18-to-30-year olds. Nutri- a nutrition care process outcomes study
tions for self-monitoring and increasing ents. 2019;11(3):621. from a veterans’ health care facility
daily fruit and vegetable consumption: a 50. Feehan LM, Geldman J, Sayre EC, et al. [Published online ahead of print July 27,
systematized review. Nutrients. Accuracy of fitbit devices: systematic re- 2020]. J Acad Nutr Diet; 2020. https://doi.
2019;11(3):686. view and narrative syntheses of quanti- org/10.1016/j.jand.2020.04.015.
37. Dunn CG, Turner-McGrievy GM, Wilcox S, tative data. JMIR Mhealth Uhealth. 66. Swan WI, Vivanti A, Hakel-Smith NA, et al.
Hutto B. Dietary self-monitoring through 2018;6(8). 2018;e10527. Nutrition care process and model update:
10 JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS -- 2021 Volume - Number -FROM THE ACADEMY
toward realizing people-centered care 69. Joshi A, Amadi C, Schumer H, 72. The Office of the National Coordinator for
and outcomes management. J Acad Nutr Galitzdorfer L, Gaba A. A human centered Health Information Technology (ONC).
Diet. 2017;117(12):2003-2014. approach to design a diet app for patients 2017. https://www.healthit.gov/topic/health-
67. Chen J, Gemming L, Hanning R, Allman- with metabolic syndrome. Mhealth. it-basics/glossary. Accessed September 24,
Farinelli M. Smartphone apps and the 2019;5:43. 2020.
nutrition care process: current perspec- 70. Trials Transformation Initiative. Digital 73. Gemming L, Utter J, Ni Mhurchu C. Image-
tives and future considerations. Patient Health Technologies. https://www.ctti- assisted dietary assessment: a systematic
Educ Couns. 2018;101(4):750-757. clinicaltrials.org/projects/digital-health- review of the evidence. J Acad Nutr Diet.
68. Chen J, Lieffers J, Bauman A, Hanning R, technologies. Accessed September 24, 2015;115(1):64-77.
Allman-Farinelli M. The use of smart- 2020. 74. Academy of Nutrition and Dietetics.
phone health apps and other mobile 71. U.S. Food and Drug Administration. https://www.eatrightpro.org/practice/
health (mHealth) technologies in dietetic https://www.accessdata.fda.gov/scripts/ practice-resources/telehealth/practicing-
practice: a three country study. J Hum cdrh/cfdocs/cfpmn/denovo.cfm?ID¼DEN telehealth. Accessed September 24,
Nutr Diet. 2017;30(4):439-452. 180044. Accessed September 24, 2020. 2020.
-- 2021 Volume - Number - JOURNAL OF THE ACADEMY OF NUTRITION AND DIETETICS 11You can also read