Amy Ravin, MD Katherine Massa, MD - Breastfeeding for the Medical Professional - ASTHO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Breastfeeding for the Medical
Professional
Amy Ravin, MD
Katherine Massa, MD
Source for much of this talk: Joan Younger Meek, MD, FAAP AAP Section on Breastfeeding

Disclosure • We have no actual or potential conflicts of interests. • We do not intend to discuss off label medication use.

Objectives: • Understand the benefits of breastfeeding and the risks of not breastfeeding • Understand the process of lactation • Become familiar with some of the initiatives and laws around breastfeeding
AAP Policy Statement • Human milk is the normative standard for infant feeding and nutrition • Breastfeeding should be considered a public health issue and not a lifestyle choice AAP Pediatrics 2012;129;e827-41.

AAP Policy Statement • Human milk is species-specific, uniquely superior for infant feeding, and promotes optimal growth, health, and development. • Direct breastfeeding is best, but expressed breast milk, fortified when appropriate for premature infants, is next best.

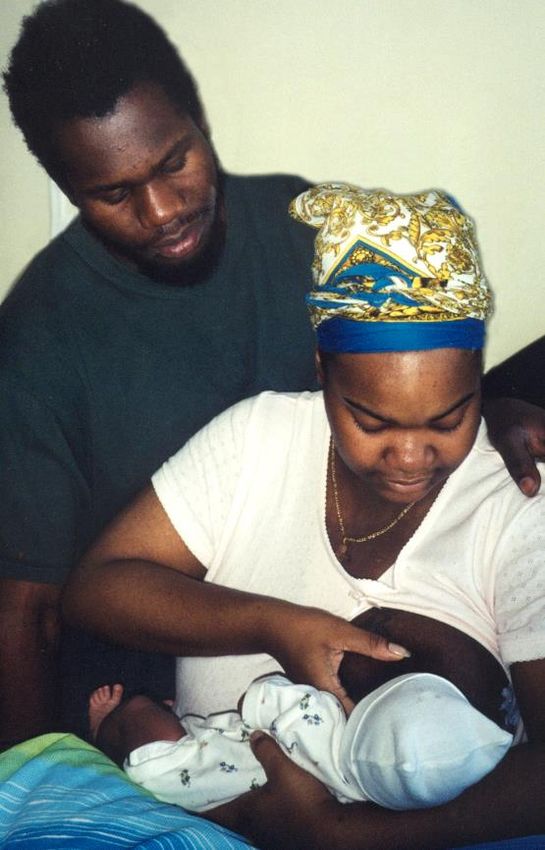
AAP Policy Statement • Medical providers should provide complete, current information on the benefits of breastfeeding and promote breastfeeding as a cultural norm. • A decision to choose not to breastfeed should occur only after the family has been fully informed about the benefits of breastfeeding and potential risk of not receiving human milk. Photo © Roni M. Chastain, RN

Healthy People 2020 Objectives • Increase the proportion of mothers who breastfeed their babies. • Decrease the percentage of breast-fed newborns who receive formula supplementation within the first 2 days of life. • Increase the percentage of live births that occur in facilities that provide recommended care for lactating mothers and their babies.

Healthy People 2020 Healthy People Maternal, Infant, and Child Health 2020 Objectives: http://www.healthypeople.gov/2020/topicsobjectives2020/objectives

National Immunization Survey
Infants Born in 2008 in US
HP 2020 US (%)
Goals (%)
Initiation 81.9% 74.6
6 mo (any) 60.6 44.3
12 mo (any) 34.1 23.8
3 mo (exclusive) 46.2 35.0
6 mo (exclusive) 25.5 14.8
http://www.cdc.gov/breastfeeding/data/NIS_data/2011 Breastfeeding Report Card Breastfeeding Report Card: http://www.cdc.gov/breastfeeding/data/reportcard.htm
Percent of Children Ever Breastfed by
State (2007)
http://www.cdc.gov/breastfeeding/data/NIS_data/2007Supplementation Rates in the US • Within 2 days of birth: 25% • Within 3 months: 36% • Within 6 months: 43% CDC, 2011 Data, for cohort born in 2008 http://www.cdc.gov/breastfeeding/data/nis_data/
Baby-friendly Hospital Initiative (BFHI) • A global effort launched by WHO and UNICEF to implement practices that protect, promote and support breastfeeding. • A maternity facility can be designated 'baby-friendly' when it does not accept free or low-cost breastmilk substitutes, feeding bottles or teats, and has implemented 10 specific steps to support successful breastfeeding.
WHO 1989 Ten Steps to Successful
Breastfeeding
• Every facility providing maternity services and care for
newborn infants should:
1.) Have a written breastfeeding policy that is routinely
communicated to all health care staff.
2.) Train all health care staff in skills necessary to
implement this policy.
3.) Inform all pregnant women about the benefits and
management of breastfeeding.
4.) Help mothers initiate breastfeeding within one hour of
birth.
5.) Show mothers how to breastfeed, and how to maintain
lactation even if they should be separated from their infants.6.) Give newborn infants no food or drink other than breast
milk, unless medically indicated.
7.) Practice rooming-in - that is, allow mothers and infants
to remain together - 24 hours a day.
8.) Encourage breastfeeding on demand.
9.) Give no pacifiers or artificial nipples to breastfeeding
infants.
10.) Foster the establishment of breastfeeding support
groups and refer mothers to them on discharge from the
hospital or clinic.
Source: Protecting, Promoting and
Supporting Breastfeeding: The
Special Role of Maternity
Services, a joint WHO/UNICEF
statement published by the World
Health Organization. 1989.Odds ration of continuing bf > 6 weeks Breastfed in the hospital 2.32 (1.89 - 2.84) Breastfed in the first hour after delivery 1.79 (1.57 - 2.05) Baby fed only breast milk in the hospital 3.42 (2.93 - 3.99) Hospital staff gave a BF support phone # 1.31 (1.10 - 1.57) Hospital gave info about breastfeeding 0.90 (0.68 - 1.19) Baby stayed in mom's hospital room 1.41 (1.20 - 1.65) Hospital helped with breastfeeding 0.85 (0.72 - 1.02) Hospital told mother to bf on demand 1.51 (1.29 - 1.77) Hospital gave a formula gift pack 0.74 (0.64 - 0.99) Baby given pacifier in hospital 0.62 (0.54 - 0.71)
Contraindications to Breastfeeding • Infant with classic form of galactosemia • Maternal HIV, HTLV-I, HTLV-II in U.S. • Herpes simplex lesions (active) of breast • Mothers with active, untreated tuberculosis • Mothers receiving antimetabolite or chemotherapeutic agents • Mothers with active radioisotopes • Maternal illicit substance use • Medications incompatible (rare)* Drugs and Lactation Database (LACTMED) (http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT American Academy of Pediatrics. Pickering LK (ed). Red Book: Report of the Committee on Infectious Diseases, 28th ed., 2009.
Maternal Medications • Most are compatible with breastfeeding. • Medication use in pregnancy is not the same as medication use in lactation. • Weigh benefits against risks. Drugs and Lactation Database (LACTMED) (http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT) Hale T. Medications and Mothers’ Milk 2010, 14th ed.. http://www.ibreastfeeding.com/
Maternal Medications • Choose the safest drug available. • Prescribe medications for the shortest length of time appropriate. • Use short-acting formulations. • Administer just after breastfeeding. • Monitor infant for side effects. • Report adverse effects. • See LactMed for up-to-date reference materials Drugs and Lactation Database (LACTMED) (http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?LACT) Breastfeeding and Human Lactation Study Center, University of Rochester, NY Hale T. Medications and Mothers’ Milk 2010, 14th ed. Briggs, Freeman, and Yaffe: Drugs in Pregnancy and Lactation, 9th Edition, Lippincott, Williams & Wilkins, 2011.
Conditions Not Contraindicated
During Lactation
• Hepatitis B • Maternal use of
• Hepatitis C - Caffeine
- Tobacco
• Cytomegalovirus - Alcohol (however,
• Maternal fever caution advised)
AAP Pediatrics 2012;129:e827-841.
American Academy of Pediatrics. Pickering LK (ed). Red Book: Report of the Committee on
Infectious Diseases, 28th ed., 2009.Benefits of Breastfeeding • Children • Maternal • Societal
Benefits of Breastfeeding • Species specific • Organic • Norm for infant feeding • Minimizes exposure to foreign protein • Host protection • Optimal development Photo © Roni M. Chastain, RN outcomes AAP Pediatrics 2012;129:e827-841.
Benefits of Breastfeeding • Customized • Promotes appropriate growth pattern • Provides multiple hormones and growth factors • Promotes mother-infant Photo © Roni M. Chastain, RN attachment
Immune Benefits • Secretory IgA and other immunoglobulins • Antiviral and antibacterial factors • Cellular immune components • Cytokines, including interleukins • Enzymes • Nucleotides
Childhood Growth Photo © Joan Younger Meek, MD, FAAP
Breastfeeding and Maternal Infant Health Outcomes in Developed Countries Current evidence demonstrates breastfeeding associated with reduction in risk of: • Acute otitis media • Non-specific gastroenteritis • Severe lower respiratory tract infections • Atopic dermatitis • Asthma in young children • Obesity • Type 1 and type 2 diabetes • Childhood leukemia • Sudden infant death syndrome (SIDS) • Necrotizing enterocolitis Ip S, et al: Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries, April 2007. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/clinic/tp/brfouttp.htm
Benefits of Breastfeeding
“Dose Dependency” EBF=Exclusive breastfeeding
BF=Breastfeeding
• Acute otitis media 50% less with EBF > 3-6 months
• Atopic dermatitis 42% less with EBF > 3 months
• Gastroenteritis 64% less with any BF vs. none
• Lower respiratory tract disease and hospitalization 72% less
with EBF > 4 months
• Asthma 40% less with BF > 3 months with positive family history
• Obesity 24% less with any BF
• Type 1 DM 30% less with BF > 3 months
• Type 2 DM 40% less with any BF vs. None
• Cancer:
– Acute lymphocytic leukemia 20% less with BF >6 months
– Acute myelogenous leukemia 15% less with BF >6 months
• SIDS 36% less with any BF > 1 month
Ip S, Chung M, Raman G, et al. Breastfeeding and Maternal and Infant Health Outcomes in
Developed Countries. Rockville, MD: Agency for Healthcare Research and Quality, 2007.
http://www.ahrq.gov/clinic/tp/brfouttp.htm
AAP Pediatrics 2012;129;e827-41.Child Health Benefits Decreased rates of: • Celiac disease • Inflammatory bowel disease • Hypertension • Hypercholesterolemia AAP Pediatrics 2012;129;e827-41.
Childhood Obesity • One of the most significant childhood health problems in the U.S. • Affects 20% of children in the U.S., with up to 30% classified as overweight for age • Incidence decreased in the breastfed population Breastfeeding and Maternal and Infant Health Outcomes in Developed Countries, Structured Abstract. April 2007. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/clinic/tp/brfouttp.htm AAP Section on Breastfeeding: Breastfeeding and the Use of Human Milk, Pediatrics 2005;115:496-506. Evidence on the Long Term Effects of Breastfeeding: Systematic Reviews and Meta-analyses, World Health Organization 2007, Geneva, Switzerland. http://www.who.int/child-adolescent-health/publications/NUTRITION/ISBN_92_4_159523_0.htm
Breastfeeding and Obesity • Obesity defined as a BMI > 95%ile for age • Data from the Pediatric Nutrition Surveillance System • 177,304 children followed up to 60 months • Controlled for gender, ethnicity/race, BW • Dose-responsive protective effect against obesity at age 4 years in non-Hispanic whites • Greatest protection with breastfeeding for > 12 months Grummer-Strawn LM, Mei Z: Does Breastfeeding Protect Against Pediatric Overweight? Analysis of Longitudinal Data From the Centers for Disease Control and Prevention Pediatric Nutrition Surveillance System. Pediatrics 2004;113:81-86.
Obesity Prevention • Encourage breastfeeding • “Extent and duration of breastfeeding have been found to be inversely associated with risk of obesity in later childhood, possibly mediated by physiologic factors in human milk as well as by the feeding and parenting patterns associated with nursing.” AAP Policy Statement, Committee on Nutrition, Pediatrics 2003; 112:424-430.
Cognitive Benefits
• Human milk
– Contains fatty acids, nucleotides,
oligosaccharides, and taurine
to enhance neural and retinal
development
– Enables child to reach full
developmental potential
• Human milk fat
– Provides essential fatty acids
– Provides long-chain polyunsaturated fatty acids,
including docosahexaenoic acid
(DHA) and arachidonic acid (ARA)Breastfeeding Outcomes for
Premature Infants
• Lower rates of • Improved
– Sepsis – Leptin and insulin
– Nectrotizing enterocolitis metabolism
– Retinopathy of – Neurodevelopmental
prematurity outcomes
– Metabolic syndrome
– Blood pressure
– Low-density lipoprotein
levels
AAP Pediatrics 2012;129:e827-841.Maternal Health Outcomes
from Breastfeeding
• Decreased postpartum
bleeding
• More rapid uterine
involution
• Decreased menstrual
blood loss
• Increased child spacing
Photo © Amy Kotler, MD, FAAP
AAP Pediatrics 2012;129:e827-841.Maternal Benefits of
Breastfeeding BF=Breastfeeding
• Type 2 diabetes mellitus 4-12% less for each year of
BF for women w/out history gestational DM
• Pre-menopausal breast cancer 4.3-28% less for each
year of BF
• Ovarian cancer 21% less for any vs. no BF and
evidence for dose response
• Postpartum depression less for short term BF vs. no
breastfeeding
Ip S et al: Breastfeeding and Maternal and Infant Health Outcomes in
Developed Countries, April 2007. Agency for Healthcare Research and
Quality, Rockville, MD. http://www.ahrq.gov/clinic/tp/brfouttp.htmMaternal Outcomes • Breastfeeding associated with decreased risk of • rheumatoid arthritis • obesity • cardiovascular disease AAP Pediatrics 2012;129:e827-841.
Lactational Amenorrhea Method
Have mother’s
menses returned?
Yes
No
Is mother supplementing Advise
regularly or allowing long Yes another method
periods without breastfeeding? of family
planning.
No
Is the baby older than Yes
6 months?
Reprinted from Contraception. 1997;55:328, Multicenter study
No of the Lactational Amenorrhea Method (LAM): I. Efficacy,
duration,and implications for clinical application,
Labbok MH et al, with permission from Elsevier
There is a 1%–2% risk
of pregnancy.The Economic Benefits of
Breastfeeding
• U.S. Department of Agriculture
• $3.6 billion dollars would be saved annually
if US breastfeeding rates increased to that
recommended in Healthy People 2010
guidelines
• Projected figures were based on analysis of
decreased otitis media, gastroenteritis, and
necrotizing enterocolitis cost savings only
J Weimer: U.S.D.A., Food Assistance and Nutrition Research Report No. 13, March 2001
http://www.ers.usda.gov/publications/fanrr13Burden of Suboptimal
Breastfeeding in the US
• Analyzed saving for those conditions validated by
the AHRQ report:
– necrotizing enterocolitis
– otitis media
– gastroenteritis
– hospitalization for lower respiratory tract infections
– atopic dermatitis
– sudden infant death syndrome
– childhood asthma
– childhood leukemia
– type 1 diabetes mellitus (type 2 DM excluded)
– childhood obesity
Bartick M: The Burden of Suboptimal Breastfeeding in the United
States: A Pediatric Cost Analysis. Pediatrics online April 2010.Burden of Suboptimal
Breastfeeding in the US
• Results: If 90% of US families could comply with
medical recommendations to breastfeed
exclusively for 6 months, the United States would
save $13 billion per year and prevent an excess
911 deaths, nearly all of which would be in infants
($10.5 billion and 741 deaths at 80% compliance).
• Conclusions: Current US breastfeeding rates are
suboptimal and result in significant excess costs
and preventable infant deaths. Investment in
strategies to promote longer breastfeeding
duration and exclusivity may be cost-effective.
Bartick M, Reinhold A. The Burden of Suboptimal Breastfeeding in the United
States: A Pediatric Cost Analysis. Pediatrics. 2010;125:e1048.Business Case for Breastfeeding www.womenshealth.gov
Community Benefits
• Breastfeeding is convenient, saves money,
and is “green”
• Reduced health care costs
• Lower employee absenteeism
• Convenient and cost effective
• Environmentally friendly
• Decreased energy demands for production
and transport of infant formulaSummary of Breastfeeding Benefits • Promotes optimal health outcomes for mothers and children • Prevents infectious diseases for children • Assures that children meet their full developmental potential • Reduces health care costs • Is environmentally conscious
Process of Breastfeeding • Breast anatomy • Physiology of milk production • Breastfeeding positions • Latch
Mammary Gland
Alveoli
Ducts
Nipple
Areola Robert McBride,
Medical Illustrator
Fat and
connective tissueAnatomy of Breast, Baby’s Mouth, Latch and Suckling Robert McBride, Medical Illustrator
Pituitary releases
prolactin and oxytocin
Stimulation of Hormones travel
nerve endings via bloodstream
in mother’s to mammary gland
nipple/areola sends signal to stimulate milk
to mother’s hypothalamus/ production and
pituitary. milk ejection
reflex (let-down).
Infant suckles
at the breast.Maternal Factors That Support
Optimal Lactation
• Normal breast anatomy
• Intact neuroendocrine reflex
• Good general health and nutritional status
• Effective support systemNutrition During Lactation • Generally healthy diet • Drink fluids to thirst • Adequate protein • Additional 450-500 kcal/day • Calcium and vitamin D • 200-300 mg docosahexaenoic acid (DHA) per day • Consider multivitamin/mineral supplement
Human Milk
• Colostrum
– Earliest stage of milk
– Present before delivery and in first days
after delivery
– Low volume ideally matched with small
gastric capacity of the newborn (~5-7 ml)
– High in host defense proteins and
secretory immunoglobulin A
– Infant’s “first immunization"Human Milk
• Colostrum
• Transitional milk
– Occurs between 2-5 days postpartum until 10-14
days
– Transitional in composition between colostrum
and mature milk
– Volume of milk available increases
– Gastric capacity increases from about 20 ml (< 1
oz) to 60-80 ml (2-3 oz)Human Milk • Colostrum • Transitional milk • Mature milk – Occurs after 10-14 days – Volume continues to increase – Milk appears more watery in consistency – Breasts appear softer
Twins
breastfeeding
Photo © Nancy Wight, MD, FAAP
Premature infant
breastfeeding
Photo © Ruth A. Lawrence, MD, FAAPBreastfeeding Positions
• Mother comfortable
• Infant head in
straight line with
body
• Tummy-to-tummy or
chest-to-chest
Photo © Ruth A. Lawrence, MD, FAAPCradle Position
Cross-cradle or Transitional
Position
Photo © Joan Meek, MD, FAAPSide-lying Position
Photo © Roni M. Chastain, RNClutch or Football Position
Photo © Lori Feldman-Winter, MD, MPH, FAAPLatch • Stimulate rooting reflex. • Take sufficient areola into mouth. • Flange lips around the breast—“fish lips.” • Have wide angle at corner of mouth.
The Process of Breastfeeding • Better understanding of the process of breastfeeding and milk production can help physicians and others address early concerns about supply. • Better education may decrease early weaning and unnecessary supplementation.
AAP Policy Statement Recommended Breastfeeding Practices • Initiate in the first hour. • Keep newborn and mother together in recovery and after. • Avoid unnecessary oral suctioning. • Avoid traumatic procedures. AAP Pediatrics 2012;129:e827-841.
Breastfeeding Initiation
• Skin-to-skin contact
– Promotes physiologic
stability
– Provides warmth
– Enhances feeding
opportunities
– Infant crawls to breast
and self-attaches Photo © Joan Younger Meek, MD, FAAP
• Delay weights and measurements, vitamin K
and eye prophylaxis until after first feeding
• Knowledgeable breastfeeding advocate in
labor & deliveryAAP Policy Statement Recommended Breastfeeding Practices: • Avoid the routine use of supplements unless there is a true medical indication and the physician has ordered the supplement • Avoid the use of pacifiers in healthy, term infants, until breastfeeding is well established (approximately 3-4 weeks of age)
Medical Indications for
Supplementation
• Very low birth weight or some premature infants
• Hypoglycemia that does not respond to
breastfeeding
• Severe maternal illness
• Inborn errors of metabolism
• Acute dehydration not responsive to routine
breastfeeding or excessive weight loss
• Maternal medication use incompatible with
breastfeeding
Academy of Breastfeeding Medicine Clinical Protocol #3: Hospital
guidelines for the use of supplementary feedings in the healthy
term breastfed neonate.(www.bfmed.org)AAP Policy Statement Feeding Pattern • Encourage at least 8–12 feedings per day. • Alternate the breast that is offered first. • Allow infant to nurse on at least one side until infant falls asleep or comes off the breast to increase fat and calorie consumption.
ACA: breastfeeding • The health care law requires most health insurance plans to provide breastfeeding equipment and counseling for pregnant and nursing women.
ACA:Coverage of breast pumps • Your health insurance plan must cover the cost of a breast pump – and may offer to cover either a rental or a new one for you to keep. • Your plan may have guidelines on whether the covered pump is manual or electric, how long the coverage of a rented pump lasts, and when they’ll provide the pump (before or after you have the baby).
Patient Protection and
Affordable Care Act
• Employers must provide reasonable
break times and a private, non-
bathroom place for nursing mother to
express milk
• Applies to non-exempt (hourly) wage
earners
http://www.dol.gov/whd/nursingmothers/Some Illinois state laws
•
Ill. Rev. Stat. ch. 720 § 5/11-9 (1995) clarifies that
breastfeeding of infants is not an act of public indecency.
(SB 190)
Ill. Rev. Stat. ch. 740 § 137 (2004) creates the Right to
Breastfeed Act. The law provides that a mother may
breastfeed her baby in any location, public or private,
where the mother is otherwise authorized to be; a mother
who breastfeeds in a place of worship shall follow the
appropriate norms within that place of worship. (SB 3211)Some Illinois state laws • Ill. Rev. Stat. ch. 820 § 260 (2001) creates the Nursing Mothers in the Workplace Act. Requires that employers provide reasonable unpaid break time each day to employees who need to express breast milk. The law also requires employers to make reasonable efforts to provide a room or other location, other than a toilet stall, where an employee can express her milk in privacy. (SB 542)
Messages • Almost all women can and should breastfeed • Start in the “magic hour” right after birth • Breast feed on demand • No pacifiers until breastfeeding is well established • There are lots of benefits for mom and baby
Some online resources • http://www.ilbreastfeedingblueprint.org/ • http://health.mo.gov/living/families/wic/breastfeeding/sho wme5.php • https://www2.aap.org/breastfeeding/ • http://www.who.int/topics/breastfeeding/en/ • http://www.unicef.org/programme/breastfeeding/ • http://www.womenshealth.gov/breastfeeding/breastfeedin g-resources.html • http://www.cdc.gov/breastfeeding/resources/guide.htm • http://toxnet.nlm.nih.gov/newtoxnet/lactmed.htm – Medications in breastfeeding resource
You can also read