Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Apical ballooning syndrome (Tako-Tsubo or stress
cardiomyopathy): A mimic of acute myocardial
infarction
Abhiram Prasad, MD, FRCP, FESC, FACC, Amir Lerman, MD, FESC, FACC, and Charanjit S. Rihal, MD, FACC,
Rochester, MN
Apical ballooning syndrome (ABS) is a unique reversible cardiomyopathy that is frequently precipitated by a stressful event and
has a clinical presentation that is indistinguishable from a myocardial infarction. We review the best evidence regarding
the pathophysiology, clinical features, investigation, and management of ABS. The incidence of ABS is estimated to be 1% to
2% of patients presenting with an acute myocardial infarction. The pathophysiology remains unknown, but catecholamine
mediated myocardial stunning is the most favored explanation. Chest pain and dyspnea are the typical presenting symptoms.
Transient ST elevation may be present on the electrocardiogram, and a small rise in cardiac troponin T is invariable. Typically,
there is hypokinesis or akinesis of the mid and apical segments of the left ventricle with sparing of the basal systolic function without
obstructive coronary lesions. Supportive treatment leads to spontaneous rapid recovery in nearly all patients. The prognosis is
excellent, and a recurrence occurs in b10% of patients. Apical ballooning syndrome should be included in the differential
diagnosis of patients with an apparent acute coronary syndrome with left ventricular regional wall motion abnormality and
absence of obstructive coronary artery disease, especially in the setting of a stressful trigger. (Am Heart J 2008;155:408-17.)
An association between emotional or physical stressful apical ballooning syndrome (ABS), Tako-Tsubo cardio-
triggers and adverse cardiovascular events such as death myopathy, and stress or ampulla cardiomyopathy.12-21
and myocardial infarction has been recognized for many It has also been referred to as the Broken Heart Syndrome
years.1,2 At a population level, earthquakes, wars, and in the popular press. The syndrome overlaps with the
major sporting events have all been linked to a surge in aforementioned conditions in that it is a reversible
cardiovascular mortality.3-6 Among hospitalized patients, cardiomyopathy that is frequently precipitated by a
noncardiac surgery is one of the most frequent trigger for stressful event and has a clinical presentation that is
cardiovascular events, with the highest risk in those indistinguishable from a myocardial infarction. This
undergoing vascular surgery due to coexisting severe distinct cardiac syndrome was originally described in
coronary artery disease.7 Myocardial dysfunction may 1990 in the Japanese population and was called “Tako-
occur in critically ill patients with sepsis due to a Tsubo cardiomyopathy,” named after the octopus trap-
pathogen-induced proinflammatory immune response,8 ping pot with a round bottom and narrow neck, which
and a reversible cardiomyopathy in critically ill patients resembles the left ventriculogram during systole in these
has also been reported in the absence of sepsis.9 Similarly, patients.12 Sporadic case reports followed22 until the last
neurologists have recognized an association between 5 years or so during which several cases series have been
subarachnoid hemorrhage and a reversible cardiomyo- reported from around the world, including Europe,18,23
pathy that has been termed neurogenic stunning, North America,14,16,24-26 and Australia.27 In 2006, the
characterized by acute brain injury and the absence of American Heart Association incorporated ABS into its
coronary artery disease.10,11 classification of cardiomyopathies as a primary acquired
Recently, there has been an increasing awareness of a cardiomyopathy.28
unique cardiac syndrome that has been described as the Apical ballooning syndrome is underrecognized and
often misdiagnosed. It is an important differential
diagnosis of an acute myocardial infarction. We review
From the The Division of Cardiovascular Diseases and Department of Internal Medicine, the best evidence regarding the pathophysiology, clinical
Mayo Clinic and Mayo Foundation, Rochester, MN.
Submitted September 26, 2007; accepted November 2, 2007.
features, investigation, and management of ABS.
Reprint requests: Abhiram Prasad, MD, FRCP, FESC, FACC, Cardiac Catheterization
Laboratory, Mayo Clinic, 200 First Street SW, Rochester, MN 55905.
E-mail: prasad.abhiram@mayo.edu Incidence
0002-8703/$ - see front matter
© 2008, Mosby, Inc. All rights reserved.
The precise incidence of ABS is unknown due to its
doi:10.1016/j.ahj.2007.11.008 novel nature, varied presentation, and evolving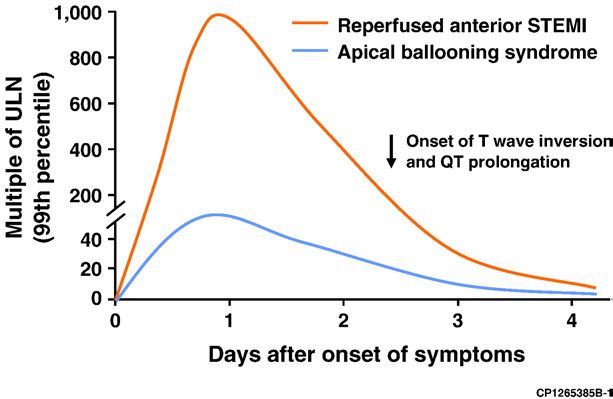
American Heart Journal
Volume 155, Number 3
Prasad, Lerman, and Rihal 409
Figure 1
Diffuse T-wave inversion with QT prolongation.
approximately 90% of all reported cases have been in
Figure 2
women. The mean age has ranged from 58 to 75 years,
with b3% of the patients being b50 years.15,34 The reason
for the female predominance is unknown but raises the
intriguing question as to whether withdrawal from
estrogens contributes to the pathogenesis. It has been
suggested that ABS may be not be diagnosed in males
because of the higher prevalence of coronary artery
disease, but this seems unlikely given the consistent sex
disparity among all published studies.
Clinical presentation
The clinical presentation in most patients is indis-
tinguishable from an acute coronary syndrome; 50%
to 60% present with chest pain at rest, which has an
Kinetics of cardiac troponin T release in patients with ABS versus angina-like quality. Dyspnea may also be the initial
acute anterior STEMI treated with mechanical reperfusion within presenting symptom, but syncope or out-of-hospital
3 hours of symptom onset. ULN, Upper limit of normal. cardiac arrest is rare.15,34 Intensive care unit patients
are likely to present with pulmonary edema, ischemic
changes on the electrocardiogram, or elevated
cardiac biomarkers. In general, hemodynamic com-
diagnostic criteria. Nevertheless, several studies have promise is unusual, but mild to moderate congestive
estimated that approximately 1% to 2% of all patients heart failure is frequent. Hypotension may occur
presenting with an initial primary diagnosis of either an because of the reduction in stroke volume and,
acute coronary syndrome or myocardial infarction have occasionally, because of dynamic left ventricular out-
ABS.14,29-32According to American Heart Association flow tract obstruction. Cardiogenic shock has been
statistics, there are 732 000 hospital discharges with a reported as a rare complication.
primary diagnosis of an acute myocardial infarction in the A unique feature of ABS is the occurrence of a
Unites States each year.33 Thus, a conservative estimate of preceding emotional or physical stressful event in
the annual rate of ABS in the United States may be 7000 to approximately two thirds of patients (Table I).15,34,35
14 000 cases. Importantly, such a trigger can not be identified in all
individuals, despite a careful history, and hence, its
absence does not exclude the diagnosis. A rise in the
Age and sex incidence of ABS was reported after the Central Niigata
Apical ballooning syndrome is a unique cardiomyo- Prefecture earthquake in Japan in 2004,36 an observa-
pathy in that it usually occurs in postmenopausal women. tion that leads us to believe that some of the
Recent review of the published case series reveals that cardiovascular morbidity and mortality associated withAmerican Heart Journal
410 Prasad, Lerman, and Rihal March 2008
Figure 3
Diastolic and systolic freeze frames from a left ventriculogram of a patient with classic ABS illustrating hyperdynamic basal contraction but akinesis
of the mid and apical segments (arrows).
Figure 4
Diastolic and systolic freeze frames from a left ventriculogram of a patient with the apical sparing variant of ABS. Function at the base and apex is
preserved with akinesis of the mid segments (arrows).
natural disasters, wars, and sporting events may be presentation may determine whether it is detected.
related to a stress cardiomyopathy. Second, there is potential for selection bias for patients
presenting with ST-segment elevation who are likely to
Electrocardiogram and cardiac undergo prompt coronary angiography and assessment of
left ventricular function. Typically, the elevation is
biomarkers present in the precordial leads, but it may be seen in the
The most common abnormality on the electrocardio- inferior or lateral leads. Nonspecific T-wave abnormality,
gram (ECG) is ST-segment elevation, mimicking an new bundle-branch block, and in some cases, a normal
ST-elevation myocardial infarction (STEMI).13 However, ECG may be the finding at presentation. When anterior
there is significant variability in the frequency (46%- ST-elevation is present, the magnitude of ST shift is usually
100%) of this finding in the published literature.15 At least less in ABS than that seen in a STEMI. The 12-lead ECG by
2 reasons may account for the variability in the reported itself is insufficient for differentiating ABS from
frequency of ST-segment elevation. First, the elevation is STEMI.37,38 Characteristic and common evolutionary
transient, and hence, the time from symptom onset to changes that may occur over 2 to 3 days includeAmerican Heart Journal
Volume 155, Number 3
Prasad, Lerman, and Rihal 411
resolution of the ST-segment elevation, development of Table I. Stressors reported to trigger ABS
diffuse and often deep T-wave inversion that involves
Emotional stress13-15,34
most leads, and prolongation of the corrected QT interval Death or severe illness or injury of a family member, friend, or pet
(Figure 1). Transient pathological Q waves may rarely Receiving bad news—diagnosis of a major illness, daughter's divorce,
develop. The T-wave inversion and QT interval prolon- spouse leaving for war
gation typically resolve over 3 to 4 months but may occur Severe argument
Public speaking
as early as 4 to 6 weeks and, in some cases, be present
Involvement with legal proceedings
beyond 1 year.39,40 Financial loss—business, gambling
Most if not all patients have a modest rise in cardiac Car accident
troponin T that peaks within 24 hours.14,16,18 The Surprise party
magnitude of increase in the biomarkers is less than that Move to a new residence
Physical stress13-15,34
observed with a STEMI and disproportionately low for the
Non-cardiac surgery or procedure—cholecystectomy, hysterectomy
extensive acute regional wall motion abnormalities that Severe illness—asthma or chronic obstructive airway exacerbation,
characterize ABS (Figure 2). Circulating brain natriuretic connective tissue disorders, acute cholecystitis, pseudomembranous
peptide, a marker of ventricular dysfunction, is invariably colitis
elevated and correlates with the left ventricular end- Severe pain—fracture, renal colic, pneumothorax, pulmonary embolism
Recovering from general anesthesia
diastolic pressure.21 Cocaine use79
Opiate withdrawal80
Stress test—dobutamine stress echo, exercise sestamibi81
Coronary angiogram and Thyrotoxicosis82
cardiac imaging
Most patients with ABS either have angiographically of delayed gadolinium hyperenhancement) from myo-
normal coronary arteries or mild atherosclerosis.15,34 cardial infarction and myocarditis in which delayed
Obstructive coronary artery disease may rarely coexist by hyperenhancement is present.16,23,26,46
virtue of its prevalence in the population at risk.
The characteristic regional wall motion abnormalities
involve hypokinesis or akinesis of the mid and apical Diagnosis
segments of the left ventricle (Figure 3). There is The diagnosis should be considered in the differential
sparing of the basal systolic function. Importantly, the diagnosis of any patient with acute myocardial infarction.
wall motion abnormality typically extends beyond the However, the classic situation is a postmenopausal
distribution of any single coronary artery. Transthoracic woman presenting with chest pain or dyspnea that is
echocardiography can detect the regional wall motion temporally related to emotional or physical stress, with
abnormality; however, visualization of the true ana- positive cardiac biomarkers or an abnormal electrocar-
tomic apex can be difficult, particularly in acutely ill diogram. Apical ballooning syndrome should also be
patients. The diagnosis is frequently made in the cardiac considered in the differential diagnosis of inpatients,
catheterization laboratory during left ventriculography including those in the intensive care unit, who develop an
because the patients are initially suspected of suffering acute reduction in left ventricular systolic function in
from an acute coronary syndrome and are referred for association with ≥1 of the following: hemodynamic
urgent or emergency coronary angiography. The right compromise, pulmonary edema, troponin elevation, or
ventricle may reveal similar regional wall motion ECG evidence of ischemia or infarction. There may be a
abnormality in approximately 30% of patients who tend higher prevalence of males in the intensive care unit
to be sicker and more likely to develop congestive heart population.16,47,48
failure.41,42 Recently, variants of ABS have been We have previously proposed the Mayo Clinic criteria
described, occurring in a significant minority of patients for the diagnosis of ABS that can be applied at the time of
with a clinical presentation similar to that of classic presentation.15 The criteria have evolved over time as our
ABS.43,44 In these patients, there is preserved function understanding of the cardiomyopathy improves.49 All 4
of the apex with wall motion abnormality that involves criteria must be present. Table II illustrates a modified
the mid segments (apical sparing variant) (Figure 4). version of the criteria. In the current version, we no
It is possible that this is simply a manifestation of early longer exclude patients who develop typical ballooning
recovery of function at the apex in some patients with in the setting of intracranial bleeding, including those
classical ABS. A rare variant presents with hypokinesis with subarachnoid hemorrhage. Neurogenic stunning in
of the base of the heart with preserved apical function this situation has the same features as ABS50,51 and is
(inverted Tako-Tsubo).45 Cardiac magnetic resonance likely a manifestation of the same spectrum of disease.
appears to be a useful imaging modality for document- The diagnosis of ABS is most likely to be made at
ing the extent of the regional wall motion abnormality institutions with cardiac catheterization laboratories
and differentiating ABS (characterized by the absence where primary percutaneous coronary intervention isAmerican Heart Journal
412 Prasad, Lerman, and Rihal March 2008
Table II. Proposed Mayo Clinic criteria for ABS may be present in as many one fifth of patients,13,16 but
symptomatic obstruction is uncommon. Dynamic out-
1. Transient hypokinesis, akinesis, or dyskinesis of the left ventricular mid
segments with or without apical involvement; the regional wall motion flow-tract obstruction may be associated with systolic
abnormalities extend beyond a single epicardial vascular distribution; a anterior motion of the mitral leaflet and mitral
stressful trigger is often, but not always present. ⁎ regurgitation.52 In the absence of heart failure, a
2. Absence of obstructive coronary disease or angiographic evidence of cautious trial of intravenous fluids and β-blockers may
acute plaque rupture. †
3. New electrocardiographic abnormalities (either ST-segment elevation
help by reducing the hypercontractility of the base of
and/or T-wave inversion) or modest elevation in cardiac troponin. the left ventricle and increase cardiac filling, thereby
4. Absence of: reducing the obstruction.53,54 Alternatively, an infusion
Pheochromocytoma of phenylephrine may be effective by increasing the
Myocarditis afterload and left ventricular cavity size in patients in
In both of the above circumstances, the diagnosis of ABS should be made with caution, whom β-blocker or intravenous fluids are contraindi-
and a clear stressful precipitating trigger must be sought. cated. Inotropes would be contraindicated in the
⁎ There are rare exceptions to these criteria such as those patients in whom the
regional wall motion abnormality is limited to a single coronary territory. presence of dynamic outflow tract obstruction.55 In
† It is possible that a patient with obstructive coronary atherosclerosis may also contrast, cardiogenic shock due to pump failure is
develop ABS. However, this is very rare in our experience and in the published
literature, perhaps because such cases are misdiagnosed as an acute coronary treated with standard therapies, which include ino-
syndrome. tropes and intraaortic balloon counterpulsation.
As with acute myocardial infarction, ABS may rarely
performed for STEMI and an early invasive strategy is lead to mechanical and arrhythmic complications.
practiced for non STEMI. The absence of obstructive Mechanical complications reported include free wall
coronary artery disease and characteristic regional wall rupture56 and severe mitral regurgitation.52 Atrial and
motion abnormality is likely to lead to the diagnosis. ventricular arrhythmias may occur, but ventricular
Diagnosing ABS in patients presenting at hospitals with- tachycardia and fibrillation is rare.13 Anticoagulation
out cardiac catheterization laboratories requires a high should be considered during the initial presentation if
index of suspicion. Establishing the diagnosis is particu- severe left ventricular systolic dysfunction is present and
larly important if fibrinolytic therapy is being considered continued for a few weeks with warfarin if there is slow
for a presumed diagnosis of STEMI. Inappropriate functional recovery to prevent thromboembolism. Left
administration of fibrinolytics to a patient with ABS may ventricular thrombus may rarely be present during the
lead to harm, and it would be reasonable to transfer a acute phase, and anticoagulation is clearly indicated in
patient suspected of the cardiomyopathy for emergency this circumstance.57
coronary angiography. In our practice, in the absence of contraindications, we
empirically recommend chronic β-blocker therapy with
Management the aim of reducing the likelihood of a recurrent episode.
Since the presentation mimics an acute coronary Initiation of angiotensin-converting enzyme inhibitor or
syndrome, initial management should be directed angiotensin receptor blocker therapy before discharge is
towards the treatment of myocardial ischemia with reasonable. This is particularly important because the
continuous ECG monitoring, administration of aspirin, diagnosis may not be certain at the time of discharge and
intravenous heparin, and β-blockers. The optimal man- these drugs would be indicated for nonreversible left
agement of ABS has not been established, but supportive ventricular dysfunction. Inhibitors of the renin angioten-
therapy invariably leads to spontaneous recovery. Once sin system can be discontinued once there is complete
the diagnosis has been made, aspirin can be discontinued recovery of systolic function in ABS. Annual clinical
unless there is coexisting coronary atherosclerosis. The follow-up is advisable because the natural history of ABS
efficacy of β-blocker therapy has not been formally remains unknown.
tested. If tolerated, it is reasonable to initiate β-blockers
empirically because excess catecholamines have been
implicated in the pathogenesis. The role of combined α-1 Prognosis
and β receptor blockade with drugs such as labetalol or The systolic dysfunction and the regional wall motion
carvedilol is unknown. abnormalities are transient and resolve completely within
Congestive heart failure is the most common com- a matter of days to a few weeks. In our experience14 and
plication occurring in approximately 20% of patients34 in other large series,13,16,25 complete recovery is seen in
and is more likely in the presence of right ventricular virtually all patients by 4 to 8 weeks. This is such a
involvement.41,42 Diuretics are effective in most cases. uniform finding that an alternative diagnosis should be
It is important to exclude dynamic left ventricular considered in patients in whom the cardiomyopathy does
outflow tract obstruction with echocardiography in not resolve. Patients with ABS generally have a good
patients with severe heart failure or significant hypo- prognosis in the absence of significant underlying
tension. Aysmptomatic intracardiac pressure gradient comorbid conditions.35 The ejection fraction should beAmerican Heart Journal
Volume 155, Number 3
Prasad, Lerman, and Rihal 413
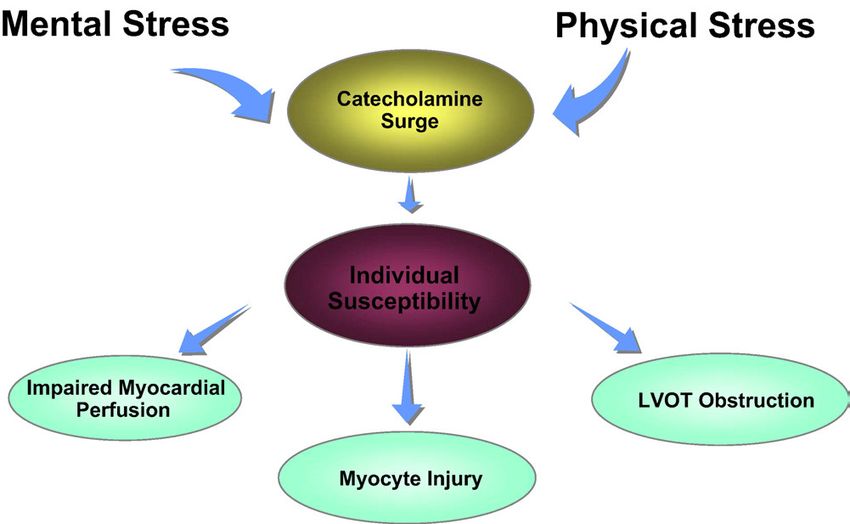
Figure 5
Proposed pathophysiology of ABS.
measured in approximately 4 to 6 weeks after discharge conjunction with a rise in catecholamines.61 Moreover,
from the hospital to document recovery of cardiac wall motion abnormalities and depressed ejection frac-
function. Inhospital mortality from ABS is very low and tion have been observed in diseases associated with high
unlikely to be N1% to 2%. Overall, the long-term survival is catecholamines such as a pheochromocytoma62,63 and
similar to that of the general age-matched population.35 subarachnoid hemorrhage.64 Wittstein et al25 have
The subgroup of patients in whom there is a physical reported very high levels of catecholamines in ABS at the
trigger such as major surgery or illness appear to have a time of presentation, which remained elevated for 7 to
worse prognosis, most likely related to the underlying 9 days. Endomyocardial biopsies in a subset of their
condition. The recurrence rate of ABS is no N10%.35 patients demonstrated contraction band necrosis, a
feature of catecholamine toxicity. However, neither the
elevation in circulating catecholamines21,47 nor the
Pathophysiology contraction band necrosis17,25,58,59 has proven to be
The pathophysiology of ABS is not well understood. consistent finding. Interestingly, in a rat immobilization
Several mechanisms for the reversible cardiomyopathy stress model of ABS, investigators have been able to
have been proposed, including catecholamine-induced induce ST-segment elevation and apical ballooning that
myocardial stunning, ischemia-mediated stunning due to can be prevented by the administration of combined
multivessel epicardial or microvascular spasm, and alpha and β adrenoreceptor antagonist.65
myocarditis (Figure 5). Myocarditis is extremely unlikely Early Japanese literature suggested that ABS may result
to be the mechanism since studies reporting endomyo- from ischemia due to multivessel epicardial spasm.66 This
cardial biopsy data have consistently shown the absence has not been confirmed in the recent larger series or in
of myocarditis.17,24,58,59 Furthermore, cardiac magnetic our experience, and we believe that epicardial spasm is
resonance imaging does not show regional delayed unlikely to be the underlying cause of ABS in most cases.
gadolinium hyperenhancement, which is a feature of It is possible that the routine administration of nitrates for
myocarditis.16,23,26 ischemic chest pain may obscure the presence of spasm.
Catecholamines may play a role in triggering the Tsuchihashi et al13 have reported that coronary spasm
syndrome because many patients have emotional or may be induced with acetylcholine provocation in 21% of
physical triggers. There is an increasing awareness of the patients in their series. However, the clinical relevance of
close interaction between cortical brain activity and the this finding is questionable because endothelial dysfunc-
heart.60 In clinical studies, mental stress has been tion is highly prevalent in postmenopausal women.
demonstrated to reduce left ventricular ejection fraction Microvascular dysfunction measured using angio-
and, rarely, induce regional wall motion abnormalities in graphic techniques such as myocardial blush grade canAmerican Heart Journal 414 Prasad, Lerman, and Rihal March 2008 be detected in at least two thirds of the patients at the myocarditis in the past. Others believe that ABS may time of presentation, and its severity correlates with the indeed be a “novel” cardiomyopathy with a true rise in magnitude of troponin elevation and ECG abnormal- incidence. It is speculated that the decreasing use of ities.67 Similarly, the TIMI frame count is prolonged in all hormone replacement therapy among postmenopausal 3 major epicardial coronary vessels in the acute setting, women may have contributed to its emergence. A indicating the presence of impaired microvascular protective role of estrogens is possible because the flow.14,19 Single photon emission computed tomography cardiomyopathy predominantly occurs in postmenopau- using thallium and sestamibi tracers and positron sal women. Experimental data indicate that estrogen emission tomography using 13 N-ammonia have consis- supplementation may abolish the deleterious effect of tently demonstrated impaired perfusion in the regions of mental stress on cardiac function in ovariectomized the wall motion abnormality.68,69 However, the meta- rats.71,73 Similarly, clinical investigations have found that bolic defect measured as fatty acid or glucose metabo- chronic estrogen supplementation attenuates the hemo- lism in these studies has generally been larger than the dynamic and catecholamine responses to mental stress,74 perfusion defect. This may be either because the and catecholamine mediated vasoconstriction.75 primary abnormality in ABS is metabolic dysfunction and An intriguing hypothesis that merits further investiga- not impaired perfusion or because the microcirculation tion is that ABS is not a unique cardiomyopathy, but recovers more rapidly than the myocardial metabolism. myocardial stunning resulting from a spontaneously At this time, it is unknown whether the impairment in aborted myocardial infarction in the territory of a large microvascular function is the primary mechanism for the left anterior descending (LAD) artery.76 To support their injury or an epiphenomenon. hypothesis, Ibanez et al have published data on five It has been suggested that development of a severe patients demonstrating the presence of plaque rupture by intracardiac gradient due to the basal hypercontractility intravascular ultrasound that was not detected by may be a primary mechanism for the disease. A geometric angiography.77 However, there are several reasons why predisposition in elderly females with a sigmoid inter- this mechanism is unlikely to account for the pathophy- ventricular septum or hypovolemia in the postoperative siology of most cases of ABS. First, the regional wall patients may lead to outflow tract or midventricular motion abnormality in typical cases is far greater than obstruction in the presence of excessive catecholamines. what can be accounted for by even a large wrap-around The resulting elevation in wall stress, oxygen require- LAD. Second, plaque rupture has not been reported in ment, and ischemia in the apical segments could cause any large case series. Third, extensive regional wall apical ballooning.70 However, if this was the case, one motion abnormality of the right ventricle in one third of would expect to document an intracardiac gradient more patients cannot be explained on the basis of LAD territory often than it has been reported in the literature or seen in ischemia. Fourth, the female predominance would be our experience.13,16 unusual for a manifestation of coronary atherosclerosis. Controversies Conclusions There is debate over the most suitable nomenclature Apical ballooning syndrome is a distinctive reversible for ABS.71,72 Tako-Tsubo cardiomyopathy12 and ABS13 cardiomyopathy that mimics an acute coronary syn- were the original names proposed by the Japanese. drome. It should be included in the differential diagnosis Most non-Japanese-speaking physicians are not familiar of patients with an apparent acute coronary syndrome with the meaning of Tako-Tsubo. Apical ballooning with regional wall motion abnormality and absence of syndrome has become popular because it is descriptive obstructive coronary artery disease. of the appearance of the left ventricle. However, ABS One of the hallmarks of ABS is that it is almost does not account for the less common variants. Some exclusively seen in postmenopausal women. This is have favored using stress cardiomyopathy or neuro- unique to the medical field and warrants further genic stunning.71 These descriptions also are not all investigation regarding the potential mechanisms. The encompassing because a stressor is absent in one third central hypothesis that a catecholamine surge is respon- of patients, and the role of the nervous system in the sible for the cardiomyopathy is challenged by the sex pathophysiology remains to be established. disparity. If this was the predominant mechanism, one There is also divergence of opinion as to the reason for would expect similar incidence in men and women. In the apparent increase in incidence of ABS. We believe fact, males have a greater adrenergic response to mental that it is not a new disease entity but that its recognition stress.57 Thus, additional hypotheses should be enter- has increased because of the greater use of cardiac tained to explain the phenomenon. It is possible that, in imaging, coronary angiography, and sensitive cardiac women, estrogen plays a protective role on the vascular biomarkers such as troponin. In addition, such cases may bed from the adverse effects of catecholamine surges. have been diagnosed as aborted myocardial infarctions or Thus, a relative deficiency of estrogen after menopause
American Heart Journal
Volume 155, Number 3
Prasad, Lerman, and Rihal 415
may predispose them to developing ABS. An alternative to heart failure (in Japanese). Tokyo: Kagakuhyoronsha Publishing
potential mechanism for the female predisposition is that Co; 1990. p. 56-64.
women are more likely to have microvascular disease 13. Tsuchihashi K, Ueshima K, Uchida T, et al. Angina Pectoris–
Myocardial Infarction Investigations in Japan. Transient left ventri-
than men.78 Thus, the preexisting microvascular dys-
cular apical ballooning without coronary artery stenosis: a novel
function in women may certainly lead to myocardial
heart syndrome mimicking acute myocardial infarction. Angina
ischemia in response to mental or physical stress. This Pectoris–Myocardial Infarction Investigations in Japan. J Am Coll
hypothesis is underscored by the observation that Cardiol 2001;38:11-8.
women have a higher incidence of acute coronary 14. Bybee KA, Prasad A, Barsness G, et al. Clinical characteristics,
syndrome with normal epicardial coronary arteries. outcomes, and impaired myocardial microcirculation in patients with
Future research also needs to explore why (1) a very transient left ventricular apical ballooning syndrome: a case-series
small proportion of the population appears to be at risk from a U.S. medical center. Am J Cardiol 2004;94:343-6.
for ABS suggesting a role for genetic predisposition; (2) in 15. Bybee KA, Kara T, Prasad A, et al. Transient left ventricular apical
ballooning syndrome: a mimic of ST-segment elevation myocardial
the classic variant, there is sparing of the basal segments
infarction. Ann Intern Med 2004;141:858-65.
of the heart with characteristic dysfunction of the apical
16. Sharkey SW, Lesser JR, Zenovich AG, et al. Acute and reversible
and mid segments; and (3) the recurrence rate is low cardiomyopathy provoked by stress in women from the United States.
despite the repeated exposure to stressful events over a Circulation 2005;111:472-9.
lifetime. Finally, there is a need to establish a registry for 17. Abe Y, Kondo M, Matsuoka R, et al. Assessment of clinical features in
ABS to investigate its natural history and conducting transient left ventricular apical ballooning. J Am Coll Cardiol 2003;
randomized trials of pharmacotherapy aimed at strategies 41:737-42.
to promote myocardial recovery and prevent recurrence. 18. Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left
ventricle: first series in white patients. Heart 2003;89:1027-31.
19. Kurisu S, Inoue I, Kawagoe T, et al. Myocardial perfusion and fatty
acid metabolism in patients with Tako-Tsubo–like left ventricular
References dysfunction. J Am Coll Cardiol 2003;41:743-8.
1. Willich SN, Maclure M, Mittleman M, et al. Sudden cardiac death. 20. Kawai S, Suzuki H, Yamaguchi H, et al. Ampulla cardiomyopathy
Support for a role of triggering in causation. Circulation 1993;87: “Takotsubo” cardiomyopathy–reversible left ventricular dysfunction:
1442-50. with ST segment elevation. Jpn Circ J 2000;64:156-9.
2. Muller JE, Abela GS, Nesto RW, et al. Triggers, acute risk factors and 21. Akashi YJ, Musha H, Nakazawa K, et al. Plasma brain natriuretic
vulnerable plaques: the lexicon of a new frontier. J Am Coll Cardiol peptide in Takotsubo cardiomyopathy. QJM 2004;97:599-607.
1994;23:809-13. 22. Pavin D, Le Breton H, Daubert C. Human stress cardiomyopathy
3. Trichopoulos D, Katsouyanni K, Zavitsanos X, et al. Psychological mimicking acute myocardial syndrome. Heart 1997;78:509-11.
stress and fatal heart attack: the Athens (1981) earthquake natural 23. Haghi D, Fluechter S, Suselbeck T, et al. Cardiovascular magnetic
experiment. Lancet 1983;1:441-4. resonance findings in typical versus atypical forms of the acute apical
4. Meisel SR, Kutz I, Dayan KI, et al. Effect of Iraqi missile war on ballooning syndrome (Takotsubo cardiomyopathy). Int J Cardiol
incidence of acute myocardial infarction and sudden death in Israeli 2007;120:205-11.
civilians. Lancet 1991;338:660-1. 24. Seth PS, Aurigemma GP, Krasnow JM, et al. A syndrome of transient
5. Witte DR, Bots ML, Hoes AW, et al. Cardiovascular mortality in Dutch left ventricular apical wall motion abnormality in the absence of
men during 1996 European football championship: longitudinal coronary disease: a perspective from the United States. Cardiology
population study. BMJ 2000;7276:1552-4. 2003;100:61-6.
6. Baumhakel M, Kindermann M, Kindermann I, et al. Soccer world 25. Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of
championship: a challenge for the cardiologist. Eur Heart J 2007;28: myocardial stunning due to sudden emotional stress. N Engl J Med
150-3. 2005;352:539-48.
7. Grayburn PA, Hillis LD. Cardiac events in patients undergoing 26. Mitchell JH, Hadden TB, Wilson JM, et al. Clinical features and
noncardiac surgery: shifting the paradigm from noninvasive risk usefulness of cardiac magnetic resonance imaging in assessing
stratification to therapy. Ann Intern Med 2003;138:506-11. myocardial viability and prognosis in Takotsubo cardiomyopathy
8. Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet 2005;365: (transient left ventricular apical ballooning syndrome). Am J Cardiol
63-78. 2007;100:296-301.
9. Ruiz Bailen M, Aguayo de Hoyos E, Lopez Martnez A, et al. Reversible 27. Abdulla I, Kay S, Mussap C, et al. Apical sparing in Tako-Tsubo
myocardial dysfunction, a possible complication in critically ill patients cardiomyopathy. Int Med J 2006;36:414-8.
without heart disease. J Crit Care 2003;18:245-52. 28. Maron BJ, Towbin JA, Thiene G, et al. American Heart Association
10. Kono T, Morita H, Kuroiwa T, et al. Left ventricular wall motion contemporary definitions and classification of the cardiomyopathies:
abnormalities in patients with subarachnoid hemorrhage: American Heart Association scientific statement from the Council on
neurogenic stunned myocardium. J Am Coll Cardiol 1994;24: Clinical Cardiology, Heart Failure and Transplantation Committee;
636-9. Quality of Care and Outcomes Research and Functional Genomics
11. Mayer SA, Fink ME, Homma S, et al. Cardiac injury associated with and Translational Biology Interdisciplinary Working Groups; and
neurogenic pulmonary edema following subarachnoid hemorrhage. Council on Epidemiology and Prevention. Circulation 2006;113:
Neurology 1994;44:815-20. 1807-16.
12. Sato H, Tateishi H, Uchida T, et al. Tako-Tsubo–like left ventricular 29. Elian D, Osherov A, Matetzky S, et al. Left ventricular apical
dysfunction due to multivessel coronary spasm. In: Kodama K, Haze ballooning: not an uncommon variant of acute myocardial infarction
K, Hori M, editors. Clinical aspect of myocardial injury: from ischemia in women. Clin Cardiol 2006;29:9-12.American Heart Journal
416 Prasad, Lerman, and Rihal March 2008
30. Pilliere R, Mansencal N, Digne F, et al. Prevalence of Tako-Tsubo 48. Haghi D, Fluechter S, Suselbeck T, et al. Takotsubo cardiomyopathy
syndrome in a large urban agglomeration. Am J Cardiol 2006;98: (acute left ventricular apical ballooning syndrome) occurring in the
662-5. intensive care unit. Int Care Med 2006;32:1069-74.
31. Parodi G, Del Pace S, Carrabba N, et al. Incidence, clinical findings, 49. Prasad A. Apical ballooning syndrome: an important differential
and outcome of women with left ventricular apical ballooning diagnosis of acute myocardial infarction. Circulation 2007;115:
syndrome. Am J Cardiol 2007;99:182-5. e56-9.
32. Azzarelli S, Galassi AR, Amico F, et al. Clinical features of 50. Lee VH, Connolly HM, Fulgham JR, et al. Tako-Tsubo cardiomyopathy
transient left ventricular apical ballooning. Am J Cardiol 2006;98: in aneurysmal subarachnoid hemorrhage: an underappreciated
1273-6. ventricular dysfunction. J Neurosurg 2006;105:264-70.
33. Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke 51. Lee VH, Oh JK, Mulvagh SL, et al. Mechanisms in neurogenic stress
statistics–2007 update: a report from the American Heart Association cardiomyopathy after aneurysmal subarachnoid hemorrhage. Neu-
Statistics Committee and Stroke Statistics Subcommittee. Circulation rocritical Care 2006;5:243-9.
2007;115:e69-e171. 52. Parodi G, Del Pace S, Salvadori C, et al. Tuscany Registry of Tako-
34. Gianni M, Dentali F, Grandi AM, et al. Apical ballooning syndrome Tsubo Cardiomyopathy. Left ventricular apical ballooning syndrome
or Takotsubo cardiomyopathy: a systematic review. Eur Heart J 2006; as a novel cause of acute mitral regurgitation. J Am Coll Cardiol
27:1523-9. 2007;50:647-9.
35. Elesber A, Prasad A, Lennon R, et al. Four-year recurrence rate and 53. Hashimoto A, Tsuchihashi K, Takuji Y, et al. Clinical implications of
prognosis of the apical ballooning syndrome. J Am Coll Cardiol mid-ventricular obstruction and intravenous propranolol use in patients
2007;50:448-52. with transient left ventricular apical ballooning, so-called Tako-Tsubo
36. Sato M, Fujita S, Saito A, et al. Increased incidence of transient cardiomyopathy. J Am Coll Cardiol 2007;49(Suppl A):93A.
left ventricular apical ballooning (so-called ‘Takotsubo’ cardio- 54. Ohba Y, Takemoto M, Nakano M, et al. Takotsubo cardiomyopathy
myopathy) after the mid-Niigata Prefecture earthquake. Circ J with left ventricular outflow tract obstruction. Int J Cardiol 2006;107:
2006;70:947-53. 120-2.
37. Bybee K, Motiei A, Syed I, et al. Electrocardiography cannot reliably 55. Previtali M, Repetto A, Scuteri L. Dobutamine induced severe
differentiation of transient left ventricular apical ballooning syndrome midventricular obstruction and mitral regurgitation in left ventricular
from anterior ST-segment elevation myocardial infarction. J Electro- apical ballooning syndrome. Heart 2005;91:353.
cardiol 2007;40:38e1-6. 56. Ishida T, Yasu T, Arao K, et al. Images in cardiovascular medicine.
38. Ogura R, Hiasa Y, Takahashi T, et al. Specific findings of the standard Bedside diagnosis of cardiac rupture by contrast echocardiography.
12-lead ECG in patients with ‘Takotsubo’ cardiomyopathy: compar- Circulation 2005;112:e354-5.
ison with the findings of acute anterior myocardial infarction. Circ J 57. Kimura K, Tanabe-Hayashi Y, Noma S, et al. Rapid formation of left
2003;67:687-90. ventricular giant thrombus with Takotsubo cardiomyopathy. Circu-
39. Kurisu S, Inoue I, Kawagoe T, et al. Time course of electrocardio- lation 2007;115:e620-1.
graphic changes in patients with Tako-Tsubo syndrome: comparison 58. Akashi YJ, Nakazawa K, Sakakibara M, et al. The clinical features of
with acute myocardial infarction with minimal enzymatic release. Circ Takotsubo cardiomyopathy. QJM 2003;96:563-73.
J 2004;68:77-81. 59. Kurisu S, Sato H, Kawagoe T, et al. Tako-Tsubo–like left ventricular
40. Matsuoka K, Okubo S, Fujii E, et al. Evaluation of the arrhythmo- dysfunction with ST segment elevation: a novel cardiac syndrome
genecity of stress-induced “Takotsubo cardiomyopathy” from the time mimicking acute myocardial infarction. Am Heart J 2002;143:
course of the 12-lead surface electrocardiogram. Am J Cardiol 2003; 448-55.
92:230-3. 60. Gray MA, Taggart P, Sutton PM, et al. A cortical potential reflecting
41. Elesber A, Prasad A, Bybee KA, et al. Transient cardiac apical cardiac function. Proc Natl Acad Sci U S A 2007;104:6818-23.
ballooning syndrome: prevalence and clinical implications of 61. Becker LC, Pepine CJ, Bonsall R, et al. Left ventricular, peripheral
right ventricular involvement. J Am Coll Cardiol 2006;47: vascular, and neurohumoral responses to mental stress in normal
1082-3. middle-aged men and women. Reference group for the Psychophy-
42. Haghi D, Athanasiadis A, Papavassiliu T, et al. Right ventricular siological Investigations of Myocardial Ischemia (PIMI) study.
involvement in Takotsubo cardiomyopathy. Eur Heart J 2006;27: Circulation 1996;94:2768-77.
2433-9. 62. Otsuka M, Kohno K, Itoh A. Periodic fluctuation of blood pressure and
43. Haghi D, Papavassiliu T, Fluchter S, et al. Variant form of the acute transient left ventricular apical ballooning in pheochromocytoma.
apical ballooning syndrome (Takotsubo cardiomyopathy): observa- Heart 2006;92:1837.
tions on a novel entity. Heart 2006;92:392-4. 63. Sanchez-Recalde A, Costero O, Oliver JM, et al. Images in
44. Hurst RT, Askew JW, Reuss CS, et al. Transient midventricular cardiovascular medicine. Pheochromocytoma-related cardiomyopa-
ballooning syndrome: a new variant. J Am Coll Cardiol 2006;48: thy: inverted Takotsubo contractile pattern. Circulation 2006;113:
579-83. e738-9.
45. Van de Walle SO, Gevaert SA, Gheeraert PJ, et al. Transient stress- 64. Naredi S, Lambert G, Eden E, et al. Increased sympathetic nervous
induced cardiomyopathy with an “inverted Takotsubo” contractile activity in patients with nontraumatic subarachnoid hemorrhage.
pattern. Mayo Clin Proceed 2006;81:1499-502. Stroke 2000;31:901-6.
46. Deetjen AG, Conradi G, Mollmann S, et al. Value of gadolinium- 65. Ueyama T, Hano T, Kasamatsu K, et al. Emotional stress induces
enhanced magnetic resonance imaging in patients with Tako-Tsubo– transient left ventricular hypokinesis in the rat via activation of the
like left ventricular dysfunction. J Cardiovasc Mag Res 2006;8: cardiac adrenoceptors: a possible animal model of “Tako-Tsubo”
367-72. cardiomyopathy. Circ J 2002;66:712-3.
47. Park JH, Kang SJ, Song JK, et al. Left ventricular apical ballooning 66. Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to
due to severe physical stress in patients admitted to the medical ICU. simultaneous multivessel coronary spasms: a review of 5 cases.
Chest 2005;28:296-302. J Cardiol 1991;21:203-14.American Heart Journal
Volume 155, Number 3
Prasad, Lerman, and Rihal 417
67. Elesber A, Lerman A, Bybee KA, et al. Myocardial perfusion in apical 75. Sung BH, Ching M, Izzo Jr JL, et al. Estrogen improves abnormal
ballooning syndrome. Correlate of myocardial injury. Am Heart J norepinephrine-induced vasoconstriction in postmenopausal women.
2006;152:469.e9-469.e13. J Hypertens 1999;17:523-8.
68. Bybee KA, Murphy J, Prasad A, et al. Acute impairment of regional 76. Ibanez B, Benezet-Mazuecos J, Navarro F, et al. Tako-tsubo
myocardial glucose metabolism in the transient left ventricular apical syndrome: a Bayesian approach to interpreting its pathogenesis.
ballooning (Tako-Tsubo) syndrome. J Nucl Cardiol 2006;13: Mayo Clin Proceed 2006;81:732-5.
244-50. 77. Ibanez B, Navarro F, Cordoba M, et al. Tako-Tsubo transient left
69. Kurisu S, Inoue I, Kawagoe T, et al. Myocardial perfusion and fatty ventricular apical ballooning: is intravascular ultrasound the key to
acid metabolism in patients with Tako-Tsubo–like left ventricular resolve the enigma? Heart 2005;91:102-4.
dysfunction. J Am Coll Cardiol 2003;41:743-8. 78. Bugiardini R, Bairey Merz CN. Angina with “normal” coronary
70. Penas-Lado M, Barriales-Villa R, Goicolea J. Transient left ventricular arteries: a changing philosophy. JAMA 2005;293:477-84.
apical ballooning and outflow tract obstruction. J Am Coll Cardiol 79. Arora S, Alfayoumi F, Srinivasan V. Transient left ventricular apical
2003;42:1143-4. ballooning after cocaine use: is catecholamine cardiotoxicity the
71. Sharkey SW, Lesser JR, Maron MS, et al. Stress cardiomyo- pathologic link? Mayo Clin Proc 2006;81:829-32.
pathy. J Am Coll Cardiol 2007;49:921. 80. Rivera JM, Locketz AJ, Fritz KD, et al. “Broken heart syndrome” after
72. Parodi G. Transient left ventricular apical ballooning—the need for a separation (from OxyContin). Mayo Clin Proc 2006;81:825-8.
common terminology. Int J Cardiol 2007;116:405. 81. Dorfman T, Aquel R, Allred J, et al. Takotsubo cardiomyopathy
73. Ueyama T, Hano T, Kasamatsu K, et al. Estrogen attenuates the induced by treadmill exercise testing: an insight into the pathophy-
emotional stress–induced cardiac responses in the animal model of siology of transient left ventricular apical (or midventricular)
Tako-Tsubo (Ampulla) cardiomyopathy. J Cardiovasc Pharmacol ballooning in the absence of obstructive coronary artery. J Am Coll
2003;42(Suppl 1):S117-9. Cardiol 2007;49:1223-5.
74. Komesaroff PA, Esler MD, Sudhir K. Estrogen supplementation attenuates 82. Rossor AM, Pearce SH, Adams PC. Left ventricular apical
glucocorticoid and catecholamine responses to mental stress in perime- ballooning (Takotsubo cardiomyopathy) in thyrotoxicosis. Thyroid
nopausal women. J Clin Endocrinol Metab 1999;84:606-10. 2007;17:181-2.You can also read

















































