Appendix 2 Prescribing Incentive Scheme 2018-19 - (Full version) - NHS Great Yarmouth and Waveney CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Appendix 2
Prescribing Incentive Scheme 2018-19
(Full version)
Document Control Sheet
Name of document: Prescribing incentive scheme 2018-19
Version: 0.5
Status: Draft
Owner: Lois Taylor/Michael Dennis
N\Primary Care\Medicines
File location / Filename: Optimisation\QIPP\Prescribing Incentive Scheme
(Workplans)
Date of this version: December 2017
Produced by: Michael Dennis, Medicines Optimisation Team
Synopsis and outcomes of
consultation undertaken:
Synopsis and outcomes of
Equality and Diversity Impact NA
Assessment:
Approved by (Committee):
Date ratified:
Copyholders:
Next review due: N/A
Enquiries to: Michael Dennis/Lois Taylor
Revision History
Revision Summary of changes Author(s) Version
Date Number
Approvals
This document requires the following approvals either individual(s), group(s) or board.
Name Title Date of Version
Issue Number
Page 2 of 15Summary of indicators for 2018-19 incentive scheme
Entry Criteria
All medicines listed below (except for vitamin D) are listed in the NHS England guidance as
items which should not routinely be prescribed in primary care. Click here for the link to this
guidance.
Co-proxamol No scripts issued from April 18
Glucosamine and Chondroitin
Herbal treatments
Homeopathy
Doxazosin MR No scripts issued from June 18
Dosulepin
Oxycodone and naloxone (Targinact®) (In the case of dosulepin and Targinact®, no scripts
Lutein + Antioxidants should be continued unless there is clear evidence
Omega 3 supplements of benefit gained since being on it and there is no
Tramacet® clinically appropriate alternative.)
Perindopril arginine
Rubefacients
Vitamin D (colecalciferol) maintenance
doses 400IU to 2000 IU (this is not in
the NHSE guidance but is included in
local guidance.
Liothyronine Local guidance to be implemented within two months
of launch.
Entry criteria continued
Warfarin and edoxaban to make up a The 80% target to be achieved by July 18.
minimum of 80% of all oral
anticoagulants prescribed in atrial
fibrillation
Prescribing Leads Meetings Nominate a practice Prescribing Lead GP who will
attend all quarterly Prescribing Leads meetings or
send a deputy GP in their place.
Non-Medical Prescriber Meetings Nominate one Non-Medical Prescriber (if the
practice has one) to attend all quarterly Non-Medical
Prescriber meetings or send an appropriate deputy
in their place.
Medicines Optimisation Support Group Nominate one practice medicines lead to attend all
Meetings (Prescribing Clerks) quarterly Medicines Optimisation Support Group
meetings or send an appropriate deputy in their
place.
Improved utilisation of pharmacy Continue to develop positive relationships with key
services - New Medicines pharmacies providing services to your patient
Services/Medicines Use Reviews population.
Develop an action plan by 30th June 2018 with an
appropriate pharmacy to support the use of targeted
pharmacy services (New Medicines Service and/or
Page 3 of 15Medicines Use Review) for the benefit of your
patients.
For example agree with the pharmacy that patients
who are prescribed a new inhaler will be referred to
the asthma/COPD New Medicines Service so that
the pharmacy can follow up the patient to check their
inhaler technique and how they are getting on with
their new inhaler.
The Medicines Optimisation Team will support these
discussions and will be able to provide referral to
pharmacy forms for the GP practice.
Indicators
Payment of £1.60 per patient plus a possible bonus of 20p per patient for exceptional
budgetary performance.
1. Budget
70p
i) Achieve budget (≤ 1% overspent) by March 2019.
ii) Come in below budget by March 2019 or practice spend to be Bonus 20p
≥8% below 17/18 forecast outturn.
iii) If the practice is >5% overspent by March 2019 but practice 40p
spend is >2% below the 17/18 forecast outturn.
iv) If the practice is between >1 – 5% overspent by March 2019 but 50p
practice spend is >2% below the 17/18 forecast outturn.
The Medicines Optimisation Team will provide a list of switches and
stops on Eclipse to support practices with coming in on budget
(appendix 2). This list will evolve as different opportunities arise.
Key savings opportunities will be e mailed to practices each month to
review and action (see monthly progress report metric number 8).
Practices more than 10% overspent will be visited on a monthly basis
to review progress and support needed.
The finance team are currently working to generate indicative
practice budgets for next year to validate this metric and ensure it
is reasonable.
2. High dose opioids
30p
Part 1
Develop an action plan to reduce the prescribing of high dose opioids Payment for this
(>120mg morphine or equivalent a day) in your practice by 30th May target will be
2018. Send a copy to GYWCCG.medsqueries@nhs.net by 30th May available in
February 2019
2018.
Page 4 of 15Part 2
Reduce the prescribing of high dose opioids per 1,000 patients by 15%.
Baseline data will be from September to November 2017. Achievement
will be measured using data from September – November 18.
Payment will be made upon achievement of the target and submission
of the action plan.
3. Benzodiazepines
30p
Part 1
Develop, agree and implement a practice policy on benzodiazepine Payment for this
and Z drug prescribing by 30th May 2018. Send a copy to target will be
GYWCCG.medsqueries@nhs.net by 30th May 2018. available in
February 2019
Part 2
Reduce the prescribing of benzodiazepines (average daily quantity per
STAR PU) by 15% from baseline if higher than the England average. If
baseline is under the England average then reduce by 5%.
Baseline data will be taken from September – November 17.
Achievement will be measured using data from September – November
18.
Payment will be made upon achievement of the prescribing target and
submission of the action plan.
4. Eclipse Live
5p
Review and action all red admission avoidance alerts on Eclipse Live
each week.
5. Urinary Tract Infection Review
5p
To evaluate the diagnosis of uncomplicated urinary tract infections
using urine dipsticks and/or urine cultures and to assess antibiotic Payment for this
prescribing using Public Health England guidance on the diagnosis and target will be
available in
antibiotic treatment (appendix 4) February 2019
Please send your completed audit to GYWCCG.medsqueries@nhs.net
by 30th September 2018.
6. National antibiotic targets
5p
Antibacterial items per STAR PU to be below 1.161
Co-amoxiclav, cephalosporins and quinolone prescribing to account for
less than 10% of all antibiotic prescribing.
Page 5 of 15Ratio of trimethoprim to nitrofurantoin items to be below 1.740
Achievement of these targets will be based on the average achieved
for the full financial year April 18 – March 19.
7. Prescribing of Proton Pump Inhibitors 5p
Daily PPI therapy increases the risk of Clostridium difficile infection. Payment for this
Many patients end up on long term PPIs and the continued need is not target will be
always thoroughly reviewed to check that benefit outweighs risks. available in
February 2019
PPI items per cost based STAR PU to be below the England average
or if already below the England average reduce by 5%.
Baseline data will be taken from September – November 17.
Achievement will be measured using data from September – November
18.
8. Reduce or maintain spend on oral nutritional supplements toPractices will receive a monthly data pack showing current position with respect to the
indicators.
Use of Payment from Scheme:
Payments received from this Scheme may only be used to benefit patient care under the
Department of Health rules attached in appendix 3.
Page 7 of 15Appendix 1 - Template to return to GYWCCG.medsqueries@nhs.net within two weeks of the
each monthly e mail being sent out.
Name of Practice
Month return relates to
Name of person completing
the return
Actions taken so far
Actions outstanding with an
estimated completion date
Page 8 of 15Appendix 2 – list of suggested switches, version 0.1
Switch from Switch to
Ezetimibe No prescribing
Dicycloverine Hyoscine tablets (Buscopan)
Tramadol SR (Zamadol SR) Tramulief SR
Diltiazem XL Diltiazem (Tildiem)
Calcium Carbonate1.5g / Vit D 400IU Calci-D (2.5g calcium carbonate 1000IU
colecalciferol)
Metformin SR tablets Sukkarto MR tablets (metformin)
Levodopa / Carbidopa / Entacapone tablet Sastravi (Levodopa / Carbidopa / Entacapone
(Stalevo) tablet)
BD Micro-Fine pen needles GlucoRX finepoint needles
Tolterodine 4mg XL capsules Neditol 4mg XL capsules
Tiotropium (Spiriva) Braltus Zonda
Diltiazem XL (Adizem XL) Diltiazem XL (Zemtard XL)
Singulair 4mg paediatric chewable tablets Montelukast 4mg chewable tablets
Rivastigmine Transdermal patch Alzest transdermal patches
Concerta XL tablets Xaggitin XL tablets
Acetylcysteine 600mg tablets NACSYS 600mg effervescent tablets
Pramipexole MR tablets Pipexus MR tablets
Nasonex spray Mometasone Nasal spray
Xalatan eye drops Latanoprost eye drops
Flixonase nasal spray Fluticasone nasal spray
Levetiracetam (Keppra) Levetiracetam
Co-codamol capsules Co-codamol tablets
Macrogol laxative (Movicol) CosmoCol
Rosuvastatin Atorvastatin or simvastatin
Buprenorphine patch Buprenorphine
Ethinylestradiol / norgestimate (Cilest) Ethinylestradiol / Norgestimate (Lizinna)
Ibuprofen Gel Fenbid gel
Ethinylestradiol / Levonorgestrel (Microgynon) Ethinylestradiol / Levonorgestrel (Rigevidon)
Elocon ointment Mometasone ointment
Cerelle or Cerazette Desogestrol
Felodipine Amlodipine
BGTS GlucoRx strips
Prednisolone EC tablet Prednisolone tablet
Ethinylestradiol / Levonorgestrel (Orvanette) Ethinylestradiol / Levonorgestrel (Rigevidon)
Ramipril tablets Ramipril capsules
Page 9 of 15Appendix 3
DH Guidance on approved uses of Incentive Scheme Funds
Approved Uses
The purchase of material or equipment which is to be used for the treatment of patients or
members of the practice, including diagnostic equipment, ECG machines, blood testing equipment, sterilisers,
nebulisers, foetal heart detectors, cryothermic probes, defibrillators and related consumables. (Where practice
staff have made significant savings in the cost of dressings and wound management, we would encourage the
purchase of items for use by nursing staff, e.g. vascular Doppler equipment).
Payments to dieticians or counsellors providing advice on diet, lifestyle, alcohol consumption or smoking.
The purchase of material or equipment which will enhance the comfort or convenience of patients of
members of the practice including furniture, furnishings, security features, vending machines or heating/air
conditioning for the practice.
The purchase of computers including hardware and software.
Non-recurring staff costs.
Initiatives to improve prescribing.
The purchase of material or equipment relating to health education including television, videos, leaflets and
posters and payment for advice on how best to disseminate health education advice to patients.
Investment in existing practice premises where the improvement or development proposals are consistent
with the Primary Care Investment Plan.
Purposes for which Practice Incentive Surplus Payments may not be spent
The purchase of services or equipment which are unconnected with healthcare.
To reduce a practice’s contribution to the employment costs of existing practice staff.
10Appendix 4 Urinary Tract Infection Review
Aim
To evaluate the diagnosis of uncomplicated urinary tract infections using urine dipsticks and/or urine
cultures and to assess antibiotic prescribing using Public Health England guidance on the diagnosis and
antibiotic treatment.
How to use this audit
Step 1: Familiarise yourself with the guidance by reviewing Figure 1: Diagnosis of UTI quick reference
guide for Primary Care, the Public Health England Quick reference guide for primary care to assess your
practice’s or your individual compliance with the recommended algorithm or visit the website for more
information and the rationale behind the recommendations:
https://www.gov.uk/government/collections/primary-care-guidance-diagnosing-and-managing-infections
Please also view Figure 2: PHE management for infection guidance in Primary Care, to determine the
proportion of your patients who have been prescribed the recommended antibiotics, including dose,
frequency and duration. You can visit the website for more information and the rationale behind the
recommendations https://www.gov.uk/government/collections/primary-care-guidance-diagnosing-and-
managing-infections
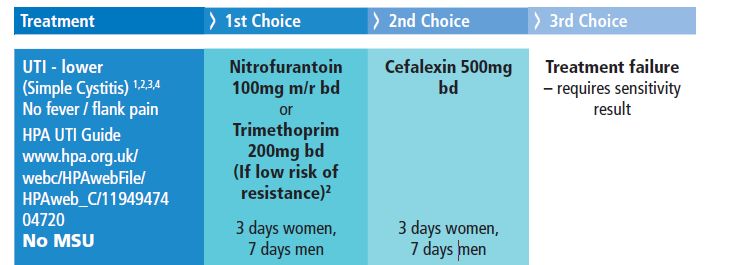
You may wish to use your local primary care organisation’s guidance as an alternative. Table 2: Great
Yarmouth and Waveney CCG Formulary for Uncomplicated UTI
Please view the TARGET treating Your Infection UTI (TYI-UTI) leaflet for self-care safety netting and other
patient advice to share during the consultation.
Step 2: Search for 20-40 consultations (minimum 20) relating to uncomplicated UTI in patients under the
age of 65 years. The Read codes below are a sample of codes that can be used, but consider adding
codes that you or your colleagues are likely to use when you see patients with uncomplicated UTIs.
Searching for just a few Read codes that you usually use may identify all the consultations you require for
the audit.
K15 Cystitis
K190 Urinary tract Infection
1J4 Suspected UTI
K190z UTI, site not specified NOS
11Figure 1: Diagnosis of UTI quick reference guide for Primary Care
Diagnosis of UTI
Quick Reference Guide for Primary Care
URINARY SYMPTOMS IN ADULT WOMENFigure 2: PHE management for infection guidance in Primary Care. Please click link for most recent updates.
Table 1: PHE Primary Care Guidance for Uncomplicated UTI
CONDITION COMMENTS DRUG DOSE DURATION
Treat women with severe/≥3 100mg m/r BD OR 50mg i/r
UTI in adults symptoms. First line: nitrofurantoin QDS (BD dose increases
(lower) All patients first line antibiotic: compliance)
nitrofurantoin if GFR >45mls/min. If low resistance risk: 200mg BD
trimethoprim Women: 3d
If GFR 30-45, only use if no
PHE UTI alternative. If first line unsuitable 400mg stat then 200mg TDS Men: 7d
Diagnosis and GFR38°C, or recent travel to a country with increased resistance; previous UTI resistant to
NHS Scotland
UTI 1.5°C above base twice in 12 hours, trimethoprim, cephalosporins, or quinolones.
and >1 other symptom.
If treatment failure: always perform
If risk of resistance: send urine for culture and susceptibilities; safety net.
culture.
Table 2: Great Yarmouth and Waveney CCG Formulary for Uncomplicated UTI
Link to GY&W CCG Antibiotic formulary 2018
http://nww.knowledgeanglia.nhs.uk/LinkClick.aspx?fileticket=qAVEeJXZw3k%3d&tabid=319&portalid=1
13Step 3: Compete the data collection table below for each selected patient.
Compliance with PHE Guidance for Management Your target %
of 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 for good
Uncomplicated UTI practice
A. No antibiotic given
B. Back-up/delayed antibiotic given with
advice about how to access
C. Immediate antibiotic given with advice on
compliance
D. Management appropriate for clinical
presentation?
E. Advice given on natural history and
average length of illness
3 days
F. Advice given about managing symptoms
including fever
Self-care advice
G. Information about when to re-consult
safety netting advice
H. Information shared on antibiotic use and
resistance
I. Shared the TARGET Treating Your
Infection UTI leaflet
J. Antibiotic choice correct
1st line: nitrofurantoin
If low resistance risk trimethoprim
K. Dose/frequency correct
nitrofurantoin 100mg m/r BD OR 50mg i/r
QDS
trimethoprim 200mg BD
L. Course length correct
women: 3 days
men: 7 days
14For ease of use you can now summarise your data the Summary table below.
Total number of patients …………………..
Row
Number Total
in
of % of Target
table Criteria
patients Patient %
belo
(N) s
w
Management decision
A No antibiotic given >70%
Back-up/delayed antibiotic given with advice about how to
BYou can also read

















































