AROs in Health Care Workers "Superbad" Bacteria - Dr. Maureen Cividino InfectionControl/Occupational Health, PHO Grateful Acknowledgement to Dr ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

AROs in Health Care Workers
“Superbad” Bacteria
Dr. Maureen Cividino
InfectionControl/Occupational Health, PHO
Grateful Acknowledgement to Dr. Allison McGeer
for her generous sharing of presentation content
February 15, 2012 CHICA/TPIC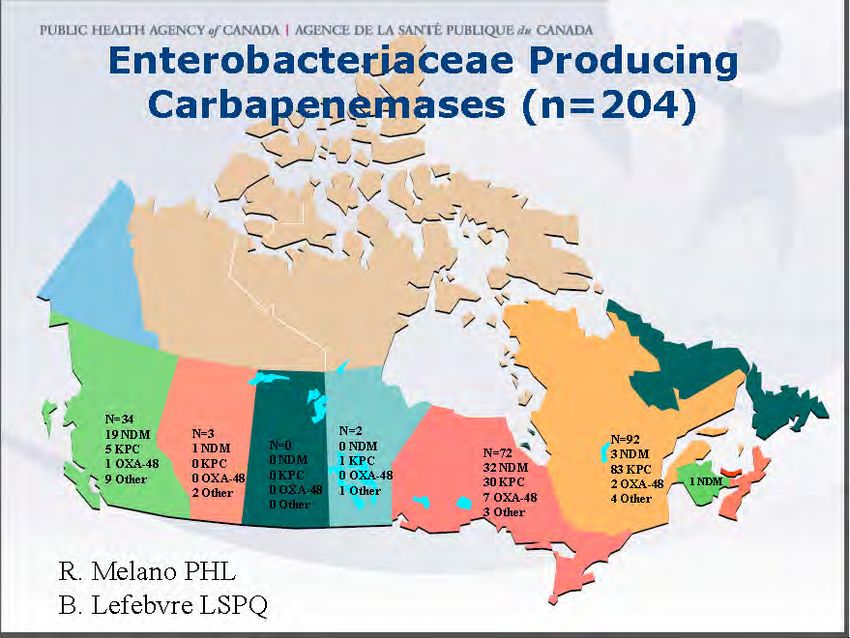
I have no conflict of interest to declare Objective: TO DISCUSS BEST PRACTICES FOR IDENTIFYING AND MANAGING HEALTH CARE WORKERS WITH AROS
Meeting the Objective
• Identification
• Who is at risk?
• Patient
• Health Care Worker
• What are they at risk for?
• MRSA
• VRE
• C. difficile
• ESBL CRE
• Management
• Who do you treat?
• What do you treat them for?
• Prevention
• RPAP
3
W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
4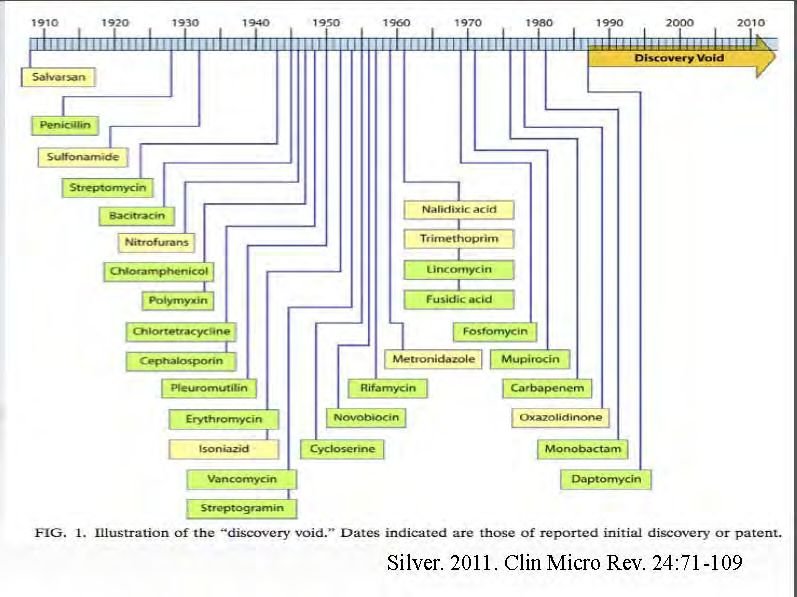
Way Back When…
The start of antibiotic resistance: Penicillin
Science Museum/Science &
Society Picture Library
Fleming Florey
1928 & Chain
Public Health Information Library
1940
Bacterial evolution vs mankind’s ingenuity
• Adult humans contains 1014 cells, only
10% are human – the rest are bacteria
• Antibiotic use promotes Darwinian
selection of resistant bacterial species
• Generation time for bacteria: 20
minutes vs years for humans
• Bacteria have efficient mechanisms of
genetic transfer – this spreads
resistance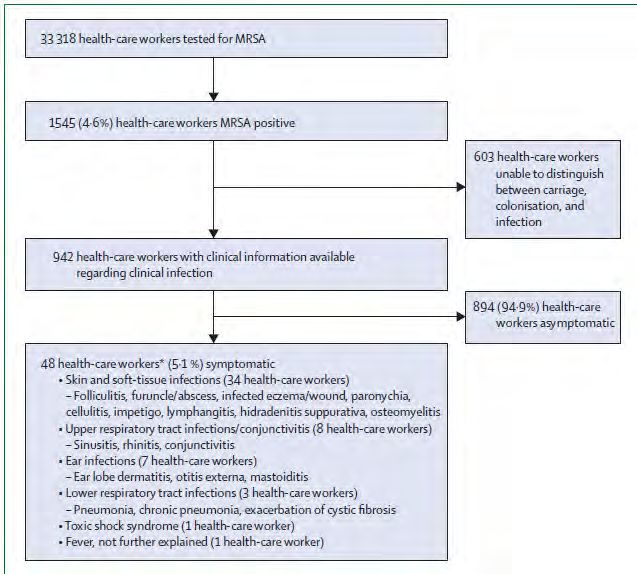
W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
7
Hospitals and Antibiotic
Resistance
www.CartoonStock.com
victim Contaminated
environment
vector Colonization
anterior nares Clean
equipment
source
Unwashed
Clean Hands
hands
9
Who is at risk?
• ARO Protocol
This protocol applies to all persons carrying on
activities in the hospital who have direct patient
contact including employees, students, volunteers,
undergraduate and postgraduate medical trainees,
physicians and contract workers. The term Health Care
Worker (HCW) is used in this protocol to describe
these individuals
• TB Protocol
Airborne transmission—MDR TB
10Who is at risk?
11Risk Factors for MRSA in HCWs
Health-care workers: source, vector, or victim of MRSA
Albrich, Harbarth htt;://infection.thelancet.com Vol 8
2008
• MRSA carriage—co-morbidities
• Cutaneous lesions or conditions, (dermatitis, eczema, psoriasis,
pemphigus)
• Sinusitis, rhinitis (chronic, allergic, infectious)
• Chronic otitis externa, CF, recent UTI
• MRSA carriage—work-related factors
• Poor attention to infection control practices
• Longer duration of service
• Area of service
• Work in areas of high patient MRSA prevalence (country)
12http://infection.thelancet.com Vol 8 May 2008
13Health Care Worker’s Family and MRSA transmission
• 8 studies report transmission to HCW families
• Eveillard found 29% prevalence among family members of
colonized HCWs with identical PFGE patterns
• Kniehl, Becker and Forster found extensive contamination in
homes of HCWs with unsuccessful eradication of colonization
• Screening of close household contacts found colonization in 8 of 11
carriers
14W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
15What are the bugs of concern for HCWs? Canadian Hospital AROs • S. aureus: MRSA √ • Enterococci: VRE × • Clostridium difficile ×? • Enterobacteriaceae (gram negatives): ESBL/CRE × • MDR-TB and XDR-TB ×?
Evolution of antimicrobial-resistant S. aureus as a cause
of nosocomial and, then, community-acquired infections
Grey diamonds, nosocomial infection;
Black diamonds, community-acquired infection.
McDonald CID, 2006CNISP MRSA rates
Figure 1A: Overall MRSA rates, CNISP 1995-2009: (per 1,000 patient-admissions)
10.0
9.0
Rate per 1,000 patient-admissions
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Surveillance year
Overall MRSA rate Overall MRSA infection rate Overall MRSA colonization rateMRSA colonization in HCWs
16 15
14
Percent HCWs colonized
12
10
8
6.2 6.6
6 5.2
4 3.4
2
0
0.2
Portugal France US (1) US (2) Australia Netherlands
Verwer EJCMID 2011;epubMRSA colonization by clinical exposure
9
9
8
Australia 8
France
7
Percent colonized
7
6
6
5
5
4
4
3 3
2 2
1 1
0 0
PCA RN MD Allied Clinical Lab/Xray Admin
Verwer EJCMID 2011;epub; Eveillard ICHE 2004;25:114MRSA colonization by clinical exposure
12 Australia
10
Percent colonized
8
6
4
2
0
High risk wards Low risk wards
Verwer EJCMID 2011;epubVRE (Vancomycin-resistant enterococci) • Avirulent, and don’t compete effectively with normal flora • Organism becomes endemic in hospital, but only the most compromised patients develop infection • Not an occupational health issue
What implications does this have for HCWs?
• Risk of infection
• For hospital-acquired strains, very small risk
•Additional Implications for HCWs
• Transmission to others
• Patients
• HCW source in 11/191 (6%) outbreaks; only 3
asymptomatic
• Transmission from HCWs to patients in 27/106
(26%) outbreaks
• BUT – numerous outbreaks due to HCW
colonization
• Families
• Transmission to families in 4 of 10 colonized HCWs
in French hospital, 5 of 16 HCWs in 2 Dutch
hospitals
Albrich Lancet ID 2008;8:289; Vonberg ICHE 2006;27:1123
Eveillard ICHE 2004;25:114; Mollema JCM 2010;48/ 202Addressing the Threat of Drug-Resistant Tuberculosis: A Realistic Assessment of the Challenge:
Workshop Summary.
Institute of Medicine (US).
Washington (DC): National Academies Press (US); 2009.
25What do you do for contact AROs?
• Reassure post-exposure – most exposures are too
low risk to worry about
• Offer culture if necessary ($7/specimen)
• For colonized staff
• Offer decolonization, follow-up
• Coordinate patient monitoring with infection control
• Consider work restriction only if evidence of
transmission, or in staff in the OR during implants
• Work with infection control on a policy regarding
WSIB claimsClostridium difficule
Ingestion
Transit to colon
Germination
Proliferation
Toxin productionDisease – very variable severity
Normal Sigmoid Colon
• Asymptomatic (colonized)
• Mild
• Watery diarrhea
• Colitis
• Diarrhea, pain, fever
• Toxic megacolon (local)
or septic shock (systemic)
Pseudomembranous colitisIncidence of CDAD L’Estrie (Sherbrooke and area) 1991-2003
What has happened? • New, hyper-toxin producing strains of C. difficile are spreading around the world • The incidence of disease is increasing (5-25x) • The case fatality rate has increased from 1-2% to 16% • Healthy adults with minimal (or no) antibiotic exposure are developing serious illness/dying • Community-acquired disease is appearing
Donskey EDITORIAL COMMENTARY • CID 2010:50
(1 June) • 1459
HCW impact
31Is there a risk to healthcare providers?
• At least 2 lab-acquired cases identified (defined by typing)
• Several (old) reports of suspected HCW transfer – e.g.:
• Lancet, 1989: 19yo paraplegic with meningitis and CDI; 3 nurses
with CDI onset day 7-10 after care
• Clostridium difficile isolated from hospital environment
outside of patient roomsCan it be serious?
Pregnancy associated cases, US
• 10 cases of severe pregnancy associated CDAD
• 7 without prior hospitalization
• 1 without antibiotic use
• 6 pre-partum, 4 post-partum
• 6 with toxic megacolon requiring ICU admission
• 5 with colectomy
• 3 maternal losses, 3 fetal losses
Rouphael Am J Obs Gynecol 2008;198:635What can you do about worries with AROs and HCWs ?
• (as with everyone else), ensure that staff recognize disease
and risk for disease
• Decide how to handle cases where occupational
acquisition is raised
• Where possible, advocate for hospital practices that
protect against C. difficileWHO policy on TB infection control in health-care facilities,
congregate settings and households 2009
35Emerging resistance in E. coli and
Klebsiella spp.
ESBLs
• E. coli and Klebsiella
• Most common cause of urinary tract infections in the community
• Cause of UTI, SSI, pneumonia in hospitals
• ESBLs confer resistance to third generation cephalosporins,
and/or pip-tazo and are frequently associated with other
resistance determinants
• 2-5% of community UTIs now cannot be treated with oral
antimicrobials
• A small but non-significant minority of patients admitted with
gram negative sepsis have organisms resistant to ceftriaxone,
ciprofloxacin and pip-tazo“ESBLs” – gram negative organisms frequently not susceptible
to oral antibiotics
• Theoretically could be acquired from patients, but
very unlikely
• e.g. hospital transmission of Salmonella spp.
• BUT
• Community acquisition now common, especially from
overseas travel
• Indian subcontinent>East Asia >Africa
• >Caribbean/MexicoCredit: http://hopenchangecartoons.blogspot.com/2010_08_08_archive.html
38What about “CRE”? • Enterobacteriaceae with enzymes that confer resistance not only to all penicillins and cephalosporins, but also to carbapenems
40
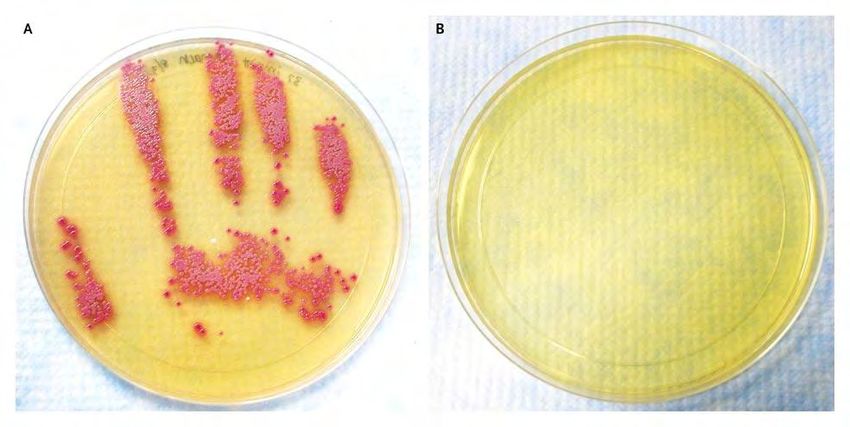
Susceptibilities of NDM containing E. coli and Klebsiella
Why are CRE a problem?
1. Enterobacteriaceae are associated with a significant burden
of disease
2. 60% of patients who acquire CRE in hospital outbreaks
develop an infection
3. CRE infections cannot be adequately treated
4. CRE outbreaks in hospitals have been very difficult to
controlSo What do we do with all this information?
43Screen or not to Screen?
Do not Screen Screening may be appropriate
• Preplacement—no routine • HCWs who are
screening at time of hire epidemiologically linked to
transmission of AROs may
• No need to reassign
immunocompromised staff; require screening
RPAP including hand hygiene • In outbreak situations when
will prevent acquisition of there is ongoing
AROs. transmission despite use of
• No need for routine ongoing Additional Precautions
screening
44HCW Post-exposure Follow-up
• First of all once patient is identified as colonized or infected
with ARO IPAC will have instituted precautions appropriate to
the specific organism
• HCW Compliance is expected with hand hygiene and
appropriate barrier precautions
• Compliance with screening if indicated:
• Swabs for culture appropriate for the ARO e.g. nasal, rectal, any open
lesion(s)
• Compliance with and completion of treatment protocols to
eradicate the ARO
• Compliance with work placement modifications if required,
pending eradication of colonization
45Screening Procedures
MRSA VRE ESBL CRE
• Consult with IPAC to determine • Rarely associated with
required sampling sites transmission—therefore
screening not generally
• Both anterior nares (one swab)
recommended
and any open lesions or areas
of dermatitis • If association with ongoing
nosocomial transmission
• Rectal or perineal or groin expected, swab should be
swabs (employees may prefer taken from the rectum, and
the option of doing their own any open lesions or areas of
rectal/perineal swab dermatitis
46Sample Decolonization Protocol for
HCWs colonized with MRSA
• 4% chlorhexidine bath daily
• Avoid contact with eyes/ears
1
• 2% mupirocin cream or ointment to anterior nares 3 times
daily
2
All for 7 days • Trimethoprim/sulfamethoxazole one DS tab orally twice daily
OR
3 • Doxycycline 100 mg orally twice daily
• Rifampin 300 mg orally twice daily
4
4
47Decolonization Protocol Follow-up
One week after treatment
swab anterior nares and
other positive sites
Week 2 repeat 3
negative Clear
sets
Week 3 repeat
48Work Restrictions for MRSA
Case by Case Basis
• Strain isolated from the HCW same genotype as outbreak
strain
• Potential consequences of MRSA in high risk populations (e.g.
ICU, burn unit, surgical services, implantable devices)
• Effectiveness of decolonization therapy
• Compliance with treatment and IPAC
• Evidence for ongoing transmission of the organism
• presence of respiratory tract infection
• Poorly controlled allergic rhinitis
• Evidence HCW linked to ongoing transmission
• Severity of any infections caused by the MRSA
49Acute Disease
• Healthcare associated AROs are generally not more likely to
cause disease in healthy individuals than antibiotic susceptible
organisms
• The concern is in interrupting transmission of AROs as
treatment options are limited
• HCWs more commonly are asymptomatic carriers; if acute
disease develops they are medically managed as appropriate
to the organism
50VRE ESBL or CRE
• HCWs colonized with VRE ESBL or CRE have rarely been
associated with transmission
• Screening for and treatment of these AROs in HCWs not
usually required
• Currently there is no established treatment regimen for HCWs
colonized with these AROs
• If HCW is implicated in transmission and found to be colonized
work practices should be reviewed, particularly hand hygiene
• Treat any dermatitis or other lesion
51W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
52CDC images
MRSA
Soft tissue infection Lower respiratory infection
• Soft tissue infection
53W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
54MOL and PIDAC recommendations
5556
57
58
59
60
61
62
63
New England Journal of Medicine Jan 15 2009
Curtis Donskey
After using ABHR
MRSA growth
HCW hand imprint after abd examC. difficile cultured from hands of
HCW
6566
Healthy Skin Healthy Patient Equation
OR
+ =W6s of AROs and HCWs
• Way back when…to now
• Who is at risk?
• And who isn’t?
• What are they at risk of getting?
• And What do we do about it?
• Where will they get it?
• And how do we know?
• When will they ever learn?
• Risk assessment and RPAP
• Why do we care?
68Why do we Care?
“The war against infectious diseases
has been won”
- US Surgeon General, 1969
“The late 20th century will be witness to the virtual elimination of
infectious disease. To write about infectious disease is almost to
write of something which has passed into history”
- Sir MacFarlane Burnett, Virologist
1962 Nobel Prize Winner
“All of the experts agree that, by the year 2000....viral
and bacterial diseases will have been eradicated.”
-Time Magazine February 1966Press Release
WHO/41
12 June 2000
DRUG RESISTANCE
THREATENS TO REVERSE
MEDICAL PROGRESS
Curable diseases – from sore throats and ear infections
to TB and malaria -- are in danger of becoming
incurable
A new report warns that increasing drug resistance
could rob the world of its opportunity to cure illnesses
and stop epidemics.
7071
72
In summary • MRSA and Clostridium difficile pose small risks to HCWs • MRSA colonization by HCWs can be associated with transmission to patients • VRE poses no risk, although HCWS can be vectors • As antimicrobial resistance worsens, recognizing the small but non-zero risk may assist with improving prevention in hospitals • Prevention remains best control—early recognition of need for AP and meticulous hand hygiene are best weapons • MDR and XDR TB increasing concern for international colleagues • Stay tuned for new information!
74
You can also read