Assessment and Treatment of Anxiety in Youth With Autism Spectrum Disorders
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Assessment and Treatment of
Anxiety in Youth With Autism
Spectrum Disorders
Roma A. Vasa, MD,a Micah O. Mazurek, PhD,b Rajneesh Mahajan, MD,a Amanda E. Bennett, MD,c Maria
Pilar Bernal, MD,d Alixandra A. Nozzolillo, MS,e L. Eugene Arnold, MD,f Daniel L. Coury, MDg
OBJECTIVES: Anxiety is one of the most prevalent co-occurring symptoms in youth with autism abstract
spectrum disorder (ASD). The assessment and treatment recommendations proposed here
are intended to help primary care providers with the assessment and treatment of anxiety
in ASD.
METHODS: The Autism Speaks Autism Treatment Network/Autism Intervention Research on
Physical Health Anxiety Workgroup, a multidisciplinary team of clinicians and researchers
with expertise in ASD, developed the clinical recommendations. The recommendations were
based on available scientific evidence regarding anxiety treatments, both in youth with ASD
and typically developing youth, and clinical consensus of the workgroup where data were
lacking.
RESULTS: Assessment of anxiety requires a systematic approach to evaluating symptoms
and potential contributing factors across various developmental levels. Treatment
recommendations include psychoeducation, coordination of care, and modified cognitive-
behavioral therapy, particularly for children and adolescents with high-functioning ASD.
Due to the limited evidence base in ASD, medications for anxiety should be prescribed
cautiously with close monitoring of potential benefits and side effects.
CONCLUSIONS: Assessment and treatment of clinical anxiety in youth with ASD require a
standardized approach to improve outcomes for youth with ASD. Although this approach
provides a framework for clinicians, clinical judgment is recommended when making
decisions about individual patients.
aKennedy Krieger Institute and Department of Psychiatry and Behavioral Sciences at the Johns Hopkins University School of Medicine, Baltimore, Maryland; bDepartment of Health
Psychology at the University of Missouri and Thompson Center for Autism and Neurodevelopmental Disorders, Columbia, Missouri; cDivision of Developmental and Behavioral Pediatrics, The
Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; dChildren’s Health Council, Palo Alto, California; eCenter for Child and Adolescent Health Research and Policy, Massachusetts
General Hospital for Children and Harvard Medical School, Boston, Massachusetts; and fNisonger Center of Excellence in Developmental Disabilities and gDepartment of Developmental and
Behavioral Pediatrics, The Ohio State University, Columbus, Ohio
Drs Vasa, Mazurek, Mahajan, Bennett, and Arnold contributed to the conception and design, analysis and interpretation of data, and drafting and revising the
manuscript; Drs Bernal and Coury contributed to the conception and design, interpretation of the data, and revising the manuscript; Ms Nozzolillo contributed to the
conception and design and revising the manuscript; and all authors approved the final manuscript as submitted.
DOI: 10.1542/peds.2015-2851J
Accepted for publication Nov 9, 2015
Address correspondence to Roma A. Vasa, MD, Center for Autism and Related Disorders, Kennedy Krieger Institute, 3901 Greenspring Ave, Baltimore, MD 21211.
E-mail: vasa@kennedykrieger.org
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
To cite: Vasa RA, Mazurek MO, Mahajan R, et al. Assessment and Treatment of Anxiety in Youth With Autism Spectrum Disorders. Pediatrics. 2016;137(S2):e20152851J
Downloaded from www.aappublications.org/news by guest on January 25, 2020
PEDIATRICS Volume 137, Number S2, February 2016:e20152851 SUPPLEMENT ARTICLEAnxiety is one of the most prevalent care providers use in their clinical treatment of anxiety in TD youth.
and impairing co-occurring practice. The workgroup was Both assessment and treatment
conditions in youth with autism composed of 7 authors of this article. recommendations were informed by
spectrum disorder (ASD).1–3 A The goal was to help clinicians clinical consensus when data were
recent meta-analysis indicated that develop a systematic approach to lacking. For each recommendation,
39.6% of youth with ASD have at the assessment of anxiety in this clinical consensus was achieved
least 1 anxiety disorder.4 Despite population, to provide treatment through an iterative process. After
this burden, youth with ASD face recommendations, and to help extensive discussion, a written
barriers in accessing timely and clinicians decide when to refer to a draft of each recommendation
appropriate mental health treatment, mental health specialist. was circulated to all members for
which places increasing demands on feedback. Recommended changes
primary care providers to manage were discussed during subsequent
anxiety in these children.5 METHODS conference calls, incorporated into
the written draft, and redistributed to
Diagnosing anxiety in youth with The ATN/Autism Intervention
the workgroup members for further
ASD can be more challenging than Research Network on Physical Health
review. The process continued until
in typically developing (TD) youth Anxiety Workgroup developed the
all workgroup members reached
because of cognitive and language current assessment and treatment
consensus with the final revision.
impairments, compromised reporting approach through a systematic multi-
of emotions, overlapping symptoms iterative process. The ATN/Autism
between anxiety and ASD, and unique Intervention Research Network RESULTS AND DISCUSSION
behavioral expressions of anxiety on Physical Health is a consortium
in the ASD population. In addition of 14 ASD centers throughout the Assessment of Anxiety
to challenges with assessment, the United States and Canada focused on
The recommendations below
field is faced with limited proven improving the clinical care of youth
present a systematic process to
treatments to target anxiety in youth with ASD. The Anxiety Workgroup
assess anxiety. Conducting a full
with ASD. The Autism Speaks Autism is composed of a multidisciplinary
assessment may take a prolonged
Treatment Network (ATN) Anxiety group of clinicians and researchers
visit or multiple visits. Practitioners
Workgroup recently authored a (child psychiatrists, developmental
whose schedule does not allow
systematic review of pharmacologic pediatricians, and a clinical
adequate time may wish to delegate
and nonpharmacologic anxiety psychologist) with extensive clinical
this assessment to a mental health
treatment studies in ASD that were experience in working with this
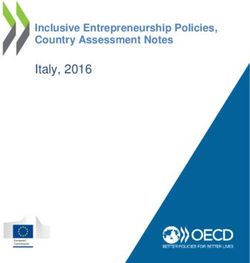
professional. The recommendations
published through June 2013.6 population.
below correspond to Fig 1.
These results showed modest
The workgroup held a series of
evidence for the efficacy of cognitive- Recommendation 1: Perform a
conference calls from April 2014
behavioral therapy (CBT) and lack Developmentally Appropriate
to November 2014 to discuss best
of randomized placebo-controlled Multi-Informant and Multi-Method
practices for both assessment and
trials investigating pharmacologic Assessment of Anxiety
treatment of anxiety in youth with
treatments for anxiety in youth with
ASD. The group reviewed relevant Current evidence recommends the
ASD. The few existing studies that
studies pertaining to anxiety and use of multiple assessment modalities
focus on anxiety are open-label or
ASD and discussed clinical practice and informants when assessing
retrospective chart reviews. This
patterns. For the assessment anxiety in children with ASD.11,12 This
finding is in contrast to data in TD
process, evidence was gleaned from process includes data from clinical
youth, which support the use of both
manuscripts on the topic indexed interviews and rating scales gathered
medications and therapy.7–9
in PubMed and/or PsychINFO, from multiple informants (eg, child,
Most primary care providers lack clinically relevant articles that parent, and teachers) as well as
specific training in managing were not indexed in PubMed or behavioral observations whenever
youth with ASD and co-occurring PsychINFO, and book chapters that possible. Assessment of anxiety
psychiatric conditions.10 On the basis were published between 2000 and in this population can be more
of this finding, coupled with the 2014. Treatment recommendations laborious than in TD youth because
lack of anxiety treatments for youth were based on findings from the of potentially compromised language
with ASD, the Anxiety Workgroup systematic review conducted by and cognitive functions in the child
sought to develop a systematic Vasa et al,6 anxiety treatment studies and the presence of multiple complex
approach to the assessment and in ASD published from June 2013 co-occurring conditions that overlap
treatment of anxiety that primary to January 2015, and studies on with anxiety. It is also important to
Downloaded from www.aappublications.org/news by guest on January 25, 2020
S116 VASA et alexplanations of these emotional
terms when needed.14 Some children
may respond better to forced choice
responses (ie, those requiring a “yes”
or “no” response) than open-ended
questions. Other children may be able
to provide responses using visual
analog scales rather than through
verbal response. If emotional insight
is compromised, results must be
interpreted cautiously.
Parent report and other caregiver
information. Clinicians must rely
on accurate reporting of children’s
anxiety symptoms by parents and
other caregivers. If child self-report
is compromised, the evaluation
must rely on reported observed
behaviors.15 These may include
avoidance and crying in response
to specific stimuli or contexts,
freezing behavior, fearful affect,
clinginess, and increased repetitive
behaviors and/or vocalizations.
Irritability, tantrums, disruptive
behavior, aggression, worsening
sleep problems, and self-injury may
also suggest the presence of anxiety.
Parents who have an anxiety disorder
may have enhanced perceptions of
anxiety in their child.16 Sometimes,
there may be disagreement between
parent and child reports.17 It is
therefore important for clinicians to
collect collateral information from
school staff and other caregivers in
the form of narratives and behavior
reports to supplement their findings.
Anxiety instruments. There are few
well-validated tools for assessing
anxiety in youth with ASD, and
as such, clinicians often depend
on measures used in TD children
when assessing anxiety in ASD.
FIGURE 1
Assessment of anxiety in youth with ASD. Some scales such as the Screen for
Child Anxiety Related Emotional
Disorders (SCARED)18 show
evaluate the anxiety symptoms in the capable of providing self-report, it
comparable psychometric properties
context of child and family stressors. is important to assess the child’s
between youth with ASD and TD
Child self-report. Children with ASD ability to understand and express youth, whereas others, such as the
may differ in their ability to self- emotions (eg, “Do you know what I Multidimensional Anxiety Scale
report symptoms of anxiety due to mean by nervous or scared?” “Tell me for Children (MASC),19 show factor
age, verbal fluency, and cognitive a time when you were nervous”) and structures that differ between the
ability.13 If the child appears to be provide developmentally appropriate 2 groups. Preliminary data on the
Downloaded from www.aappublications.org/news by guest on January 25, 2020
PEDIATRICS Volume 137, number S2, February 2016 S117Spence Children’s Anxiety Scale Recommendation 2: Assess for asking about behavioral signs of
(SCAS) indicate that it may serve Specific Anxiety Disorders and anxiety that may accompany the
as an effective anxiety-screening Anxiety Symptoms Related to the Core symptom in question (eg, is the social
tool in youth with ASD.20 Data Symptoms of ASD avoidance associated with fearful
from 2 systematic reviews indicate Many youth with ASD meet criteria affect, irritability, or physiologic
some support for the use of the for anxiety disorders according symptoms?). It is also important
following additional anxiety scales to the Diagnostic and Statistical to assess baseline ASD symptoms
in children with ASD: the Revised Manual, Fifth Edition (DSM-5).24 to differentiate preexisting ASD
Child Anxiety and Depression Scale The most common DSM-5 anxiety characteristics from new-onset
(RCADS), the Child and Adolescent disorders are social anxiety disorder, anxiety symptoms (eg, has the child
Symptom Inventory, Fourth Edition generalized anxiety disorder, and always avoided crowds or is this a
specific phobia.2 A substantial new behavior?). Other questions to
(CASI-4R), and the Pediatric Anxiety
number of children with ASD also ask include whether ASD symptoms
Rating Scale (PARS).21,22 However,
exhibit atypical anxiety symptoms have intensified (eg, has the
both reviews noted measurement
that are connected to the core frequency of repetitive behaviors
limitations across these scales.
symptoms of ASD and may not fit increased recently?) and whether
Furthermore, a recent study reported
neatly into DSM-5 categories.25 there is a relationship between
that some of these scales may not
Examples of atypical anxiety exposure to specific stimuli and
detect atypical fears.23 In summary, anxiety symptoms.
symptoms include anxiety about
data from anxiety instruments used
sensory stimuli, transitions, or social
in TD children should be interpreted Recommendation 3: Assess and
situations without accompanying Treat Other Psychiatric and Medical
cautiously when applied to youth
fear of negative evaluation. Thus, the Conditions That May Cause or
with ASD.
assessment of anxiety in children Aggravate Anxiety
with ASD should include a focus
Examination. In the office, clinicians Youth with ASD may present with
on both categorical and atypical
should conduct a physical and other types of psychiatric symptoms
symptoms.
mental status examination when such as inattention, hyperactivity,
Anxiety and ASD symptoms can irritability, aggression, self-injury,
evaluating for anxiety. Elevated
overlap. For example, social and tantrums.1,2 These symptoms
heart rate or blood pressure may
avoidance may represent behavioral may be a manifestation of anxiety
reflect situational anxiety related
avoidance of feared stimuli, which (eg, children who are anxious about
to the medical procedure or office
suggests social anxiety, or social schoolwork may exhibit irritability at
visit. Other signs of anxiety include indifference, which is a core school) or may be related to another
tremors, nail biting, bald spots feature of ASD.26 Ritualistic and disorder that is triggering the
secondary to hair pulling, and repetitive behaviors are core ASD anxiety (eg, symptoms of attention-
skin lesions due to skin picking. A symptoms and are also present in deficit/hyperactivity disorder
palpable thyroid, fine skin or hair, certain anxiety disorders, including at school may lead to academic
and/or brisk tendon reflexes suggest obsessive-compulsive disorder, struggles and subsequent anxiety
checking the thyroid status as a generalized anxiety disorder, and about schoolwork). Treating other
possible cause of anxiety symptoms. separation anxiety disorder.24 These conditions that may exacerbate
Mental status examination may rituals may serve to reduce anxiety or anxiety should therefore be part of
reveal poor eye contact, negative may be a preferred activity unrelated the treatment plan and should be
affect (eg, fear, irritability), and to negative affect.27 Clinicians should considered before treating anxiety
changes in communication (eg, therefore inquire about the function directly.
stuttering, increased vocalizations, of the ritualistic behaviors. A referral
Co-occurring medical disorders are
decreased verbal exchanges). The to a behavioral psychologist, who
prevalent in youth with ASD but may
presence of disruptive behaviors can conduct a functional behavioral
also reflect the presence of anxiety.
may reflect anxiety; however, these analysis, may help differentiate these
For example, gastrointestinal28
behaviors may also reflect a desire etiologies.
and sleep problems29may cause
to escape from the situation and Clinicians can also ask questions to or aggravate anxiety, particularly
therefore require careful assessment. help tease out whether overlapping if symptoms are more frequent or
Some children may not exhibit signs symptoms are explained solely severe or may be caused by anxiety.
of anxiety on examination even by ASD or are consistent with a Complex partial seizures can
though they experience anxiety in co-occurring anxiety disorder. present with anxiety-like symptoms,
other settings. Some of these questions include including fear, misperceptions, and
Downloaded from www.aappublications.org/news by guest on January 25, 2020
S118 VASA et alirritability.30 Some medications (eg, for increased services at school), first step. Other points to discuss
psychostimulants, bronchodilators, suggest strategies to stabilize the include delineating specific and
allergy medications) can also cause home environment (eg, increasing measurable treatment outcomes
anxiety and may need to be changed. structure and predictability), (eg, decreased avoidance of
Any medical issues affecting anxiety accessing resources (eg, behavioral feared stimuli, more responsive to
therefore warrant treatment. therapy, respite care), and promoting psychosocial interventions when
parental self-care (eg, taking breaks, anxious, sleeping in own room every
Recommendation 4: Address seeking personal mental health and night). Coordinating the treatment
Psychosocial Stressors or Suboptimal medical treatments). The child’s plan with parents and care providers
Behavioral and Educational Supports
anxiety level should be reassessed (eg, therapists, school staff) is
That May Be Contributing to Anxiety
to determine if symptoms have recommended to track progress.
Many children with ASD have a decreased after modifying these
strong need for sameness and prefer stressors. Recommendation 2: Anxiety Can Be
predictable routines and schedules.26 Treated With Modified CBT Techniques
Changes in the environment can Recommendation 5: Assess the Degree
of Anxiety-Related Impairment Preliminary data suggest that
therefore cause significant distress modified CBT (MCBT) is an
and anxiety. These changes can be After collecting all of the data, the efficacious treatment of children and
minor (eg, desks are moved in class) clinician should assess if anxiety- adolescents with high-functioning
or substantial (eg, new school, loss related impairment is present (eg, ASD and DSM-5 anxiety disorders.35
of a one-to-one aide, loss of in-home How much does anxiety interfere MCBT can be administered
behavioral support services, change with daily functioning? Is impaired individually or in a group and often
in a parent’s job schedule). functioning present across 1 or includes parental involvement.
Anxiety may also result from a multiple settings?). Assessing the
contribution of anxiety symptoms CBT in TD youth involves many
mismatch between the child’s needs
(eg, schoolwork avoidance or components, including affective
and the types of supports in place
behavioral challenges at school and education, cognitive restructuring,
in his/her daily life. For example,
home) to the overall impairment and reducing avoidance behaviors,
inadequate educational supports
functioning of the child with ASD will relaxation, modeling, and exposure
or high academic expectations
help to prioritize treatment. to the feared stimuli (with response
may cause increased stress due to
prevention). Some youth with high-
academic challenges.31 Unrecognized Treatment of Anxiety functioning ASD can understand
learning, gross or fine motor, or
If clinical anxiety persists despite basic cognitive concepts of CBT and
speech and language difficulties may
relieving potential sources of anxiety therefore may be responsive to both
aggravate such stress. Many children
or if stressors cannot be immediately the cognitive and the behavioral
with ASD experience bullying and
modified, then treatment is elements of MCBT.36 In ASD, special
peer victimization in school, which
recommended. Clinicians and parents CBT adaptations are needed to
may lead to significant anxiety.32
must decide together what the best facilitate understanding of cognitive
Stressors in the family environment treatment approach will be. Potential and emotional concepts. These
must also be evaluated. Parents of treatment barriers should be explored include the use of visual supports and
youth with ASD experience greater (eg, insurance constraints, parent concrete language, the use of written
stress than parents of children with work schedules, access to providers, materials and lists, opportunities for
Down syndrome and TD children.33 and transportation issues). Due to repetition and practice, incorporating
Stressors can include caregiver burden, limited treatment data in ASD, a special interests, video modeling,
lack of sleep, limited social and specific treatment algorithm is not and more active parent engagement
community engagement, and worries offered but rather various treatment in therapy.35 Behavioral therapy
about the future.34 Parental anxiety recommendations are presented with with exposure may be particularly
may contribute to anxiety in children, the caveat that clinicians tailor treat- useful for youth who have language
through modeling of anxious and ment on the basis of child and family and cognitive difficulties, thereby
overprotective parenting behaviors.15 circumstances and clinical judgment. precluding participation in the
Inquiring about recent stressors and cognitive components of treatment.37
working with parents to alleviate Recommendation 1: Psychoeducation Some families may have limited
and Coordination of Care Are the First access to mental health professionals
these stressors is critical. Clinicians
Steps of Treatment
can help with educational advocacy with expertise in ASD and MCBT
(eg, talking to school staff or Educating youth and families about protocols, in which case medications
writing letters indicating the need anxiety symptoms is an important may be an option. Sometimes, a child
Downloaded from www.aappublications.org/news by guest on January 25, 2020
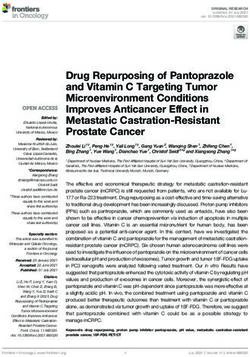
PEDIATRICS Volume 137, number S2, February 2016 S119may be resistant or severely anxious TABLE 1 Summary of Medications for the Treatment of Anxiety in Youth With ASD
during therapy (eg, exposure to a Symptomsa Medicationb Dose Rangeb References
feared stimulus results in severe Starting Dose Maximum Dose
tantrums). In these situations, Core anxiety Sertralinec 12.5 mg daily 200 mg daily Reviews in typically
parents and clinicians must decide symptoms Fluoxetinec 2.5–5 mg daily 60 mg daily developing youth:
together whether medication should Citalopramc 2.5–5 mg daily 40 mg daily Mohatt et al (2013),
be tried to facilitate engagement in Escitalopramc 1.25–2.5 mg daily 20 mg daily Strawn et al (2014)
Specific anxiety
symptomsd
therapy. Sleep Melatonin 2 mg hs 10 mg hs Guenoe et al (2011)
disturbance Clonidine 0.05 mg hs 0.2 mg hs
Nguyen et al (2014)
Trazodonee 12.5–25 mg hs 100 mg hs
Recommendation 3: Certain Physiologic Clonidinef 0.05 mg hs for 1 0.1 mg tid-qid No data in TD
symptomsf week then bid-qid or ASD youth;
Medications Can Be Considered for the Guanfacinef 0.05 mg hs for 1 1 mg tid recommendations
Treatment of Anxiety week then bid-qid based on clinical
Clonidine ERf 0.1 mg hs or qam 0.2 mg hs or consensus
Table 1 presents a summary of qamg
medications that could potentially Guanfacine 1 mg hs or qam 4 mg hs or
ERf qamg
be considered for the treatment Propanolol 10 mg bid-tid or prn 30 mg tid
of anxiety in youth with ASD. Behavioral Clonidine 0.05 mg hs for 1 0.1 mg tid-qid Reviews by: Mahajan
Because these medications have not dysregulationf week then bid-qid et al (2012), Ji and
been rigorously studied in youth Clonidine ER 0.1 mg daily 0.2–0.3 mg daily Findling (2014)
Guanfacine 0.5 mg hs for 1 week 1 mg tid
with ASD, the doses presented in then bid tid
Table 1 are based on data in TD Guanfacine 1 mg hsg 4 mg hs or qam
children and adolescents. The ER
recommendations, however, are to Situational Lorazepam 0.25–0.5 mg prn 2 mg prn No data in TD
anxietyg or ASD youth;
start medications at low doses and recommendation
titrate slowly with close monitoring based on clinical
(eg, monthly office visits) of both consensus
benefits and adverse effects. Most Propanolol 5–10 mg prn 20 mg prn
important, we recommend that bid, twice daily; ER, extended-release; hs, bedtime; prn, as needed; qam, each morning; qid, 4 times per day; tid, 3 times
per day.
primary care providers have a low a Specific anxiety symptoms refer to individual or limited symptoms of anxiety, whereas core anxiety symptoms refer to
threshold for seeking consultation the entire syndrome of cognitive, affective, and physiologic changes associated with anxiety.
b Maximum doses are based on data in TD children and adolescents. Higher doses in this table should only be used in
from a developmental/behavioral
consultation with a specialist versed in their use, such as a child psychiatrist or developmental-behavioral pediatrician
pediatrician or child psychiatrist c Discuss side effects including risk of behavioral activation. Higher doses may be needed for fast metabolizers. Slow
when prescribing psychotropic metabolizers may need lower doses.
d Behavioral dysregulation refers to symptoms of irritability, aggression, property destruction, and self-injury. For severe
medications. Consultation could be behavioral dysregulation, refer to a mental health specialist or follow the ATN pathway for treatment of irritability and
requested either before starting the problem behaviors.
e There are no data to support the use of trazodone. It is only recommended in children aged >8 years. The risk of priapism
medication or during the titration
should be discussed with the family.
process, especially if higher doses f For short and ER clonidine and guanfacine preparations, monitor blood pressure and heart rate at each visit. Check for
are used. Mental health professionals orthostatic hypotension if dizziness, light-headedness, or falls are reported. Guanfacine ER can be started in the evening
initially due to the possibility of sedation and then switched to morning, if needed. Alternatively, it can be started directly in
can assist pediatricians with titration the morning if tolerated by the patient. Guanfacine is preferred over clonidine during daytime hours because of its longer
and safety monitoring, and help tease half-life and lower potential for sedation.
g Lorazepam is a short-acting benzodiazepine (6–8 hours). For situational anxiety, it should be given 30 min before the
out the complex developmental,
event. There are no data on the use of propranolol in children and adolescents, but it is used by some experts for the
psychosocial, and medical issues that treatment of situational anxiety.
can affect treatment outcomes. If
medications are ineffective or poorly the efficacy of selective serotonin although benefits may not be seen
tolerated, gradual discontinuation is reuptake inhibitors (SSRIs) for for several weeks after treatment
recommended. Liquid preparations the treatment of anxiety disorders initiation.
are available for slower titration or if (separation anxiety, generalized
pills cannot be swallowed. anxiety, and social phobia) in TD SSRIs are frequently prescribed in
Medications with efficacy in TD youth.7 Indeed, SSRIs are the most youth with ASD38; yet, there is a lack of
children can be tried for anxiety effective pharmacologic treatments double-blind placebo-controlled trials
in ASD. Robust evidence supports for anxiety disorders in TD youth, supporting their efficacy for anxiety
Downloaded from www.aappublications.org/news by guest on January 25, 2020
S120 VASA et alin this population.6 Data from SSRI anxiety may exhibit significant response to medications should be
trials in youth with ASD report high physiologic arousal symptoms referred to an ASD mental health
rates of behavioral activation, which including increased heart rate, blood clinician (eg, a child psychiatrist,
manifests as increased activity level, pressure, sweating, and muscle developmental pediatrician,
impulsivity, insomnia, or disinhibition tension. Although no data are psychologist, and others). If the
without manic symptoms.39 available, α-agonists and propranolol child’s anxiety triggers self-injury
Thisbehavioral activation typically could be considered to reduce such and/or lopement, treating clinicians
occurs at the beginning of SSRI physiologic symptoms. should initiate appropriate
treatment or with dose increase and Anxiety can also result in interventions to keep the child
resolves with reducing the dose or behavioral dysregulation, which safe. Appropriate intervention may
discontinuing the medication. Other can be characterized by irritability, include a referral to an inpatient or
prescribing considerations include aggression, property destruction, partial hospitalization program.
a family history of bipolar disorder, and self-injury. α-Agonists (clonidine,
drug interactions, and the black box guanfacine, guanfacine extended
warning of suicidal ideation. Given SUMMARY
release), which improve symptoms
these factors, certain SSRIs (shown in of attention-deficit/hyperactivity The proposed assessment and
Table 1) are preferred over others. In disorder in youth with ASD, may treatment strategies provide a
summary, SSRIs should be prescribed potentially reduce some of these useful starting point for clinicians
cautiously in youth with ASD, with behaviors.42–44 The ATN pathway to develop a standardized approach
close monitoring. for the treatment of accompanying to the assessment and treatment of
Medications can be used to treat irritability and problem behaviors anxiety in youth with ASD. These
specific anxiety-associated symptoms can also be followed to manage these recommendations can be updated
based on evidence in ASD as well as behaviors.45 and specific treatment algorithms
expert clinical consensus. Several can be developed as research on
Youth with ASD frequently the phenomenology, risk factors,
studies discuss the management experience situational anxiety such
of sleep disturbance in youth with and treatments for anxiety becomes
as during family events, holiday available.
anxiety and ASD.40,41 Insomnia time, blood draws, and other
secondary to anxiety can be treated medical procedures. There are no
initially with melatonin, and if data on pharmacologic treatments
ineffective, there is preliminary for situational anxiety. Short-acting
evidence indicating that clonidine, benzodiazepines (eg, lorazepam) ABBREVIATIONS
a short-acting α-agonist, may help or a β-blocker (eg, propranolol) ASD: autism spectrum disorder
with insomnia. Although no data are can be considered temporarily ATN: Autism Treatment Network
available, low-dose trazodone can with close attention to sedation, CBT: cognitive behavioral
also be considered. Antihistamines cognitive impairment, and behavioral therapy
with anticholinergic effects (eg, activation. DSM-5: Diagnostic and Statistical
diphenhydramine) should be avoided
Manual, Fifth Edition
for chronic sleep difficulties due Recommendation 4: Refer to a Mental
Health Clinician if Anxiety Is Extremely MCBT: modified cognitive
to the potential for delirium and
Impairing or Is Not Responding to behavior therapy
constipation. Referral to a sleep
Interventions SSRI: selective serotonin
specialist should be considered as
reuptake inhibitor
necessary if these interventions Children with complex
TD: typically developing
are ineffective. Some children with presentations or partial or no
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr. Arnold has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, Young Living, NIH, and
Autism Speaks. Dr. Arnold has consulted with or been on advisory boards for Gowlings, Neuropharm, Novartis, Noven, Organon, Otsuka, Pfizer, Roche, Seaside
Therapeutics, Sigma Tau, Shire, and Tris Pharma and has received travel support from Noven. Dr. Coury has research grants from Autism Speaks and SynapDx.
He is on the advisory board for Cognoa and on the Data Safety Monitoring Board for Neuren Pharmaceuticals. He is also on the Speaker’s Bureau for Abbott Labs.
Dr. Vasa has a grant from Autism Speaks. Dr. Bennett has had research funding from Seaside Therapeutics, Shire, Neurim pharmaceuticals, NIH, and Autism
Speaks. The remaining authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: This research activity was supported by a cooperative agreement UA3 MC11054 through the US Department of Health and Human Services, Health
Resources and Services Administration, Maternal and Child Health Research Program to the Massachusetts General Hospital. This work was conducted through
the Autism Speaks Autism Treatment Network serving as the Autism Intervention Research Network on Physical Health.
Downloaded from www.aappublications.org/news by guest on January 25, 2020
PEDIATRICS Volume 137, number S2, February 2016 S121POTENTIAL CONFLICT OF INTEREST: Dr Arnold has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, Young Living, the
National Institutes of Health, and Autism Speaks; he has consulted with or been on advisory boards for Gowlings, Neuropharm, Novartis, Noven, Organon, Otsuka,
Pfizer, Roche, Seaside Therapeutics, Sigma-Tau, Shire, and Tris Pharma and has received travel support from Noven; Dr Coury has research grants from Autism
Speaks and SynapDx; he is on the advisory board for Cognoa and on the Data Safety Monitoring Board for Neuren Pharmaceuticals as well as on the Speaker’s
Bureau for Abbott Laboratories; Dr Vasa has a grant from Autism Speaks; Dr Bennett has had research funding from Seaside Therapeutics, Shire, Neurim
Pharmaceuticals, the National Institutes of Health, and Autism Speaks; Drs Mahajan and Mazurek and Ms Nozzolillo have indicated they do not have any potential
conflicts of interest to disclose.
The views expressed in this article do not necessarily reflect the views of Autism Speaks or the Health Resources and Services Administration.
REFERENCES
1. Gjevik E, Eldevik S, Fjæran-Granum T, tolerability of antidepressants 17. Lerner MD, Calhoun CD, Mikami AY, De
Sponheim E. Kiddie-SADS reveals high in pediatric anxiety disorders: a Los Reyes A. Understanding parent-
rates of DSM-IV disorders in children systematic review and meta-analysis. child social informant discrepancy in
and adolescents with autism spectrum Depress Anxiety. 2015;32(3):149–157 youth with high functioning autism
disorders. J Autism Dev Disord. spectrum disorders. J Autism Dev
9. Read KL, Puleo CM, Wei C, Cummings
2011;41(6):761–769 Disord. 2012;42(12):2680–2692
CM, Kendall PC. Cognitive-behavioral
2. Simonoff E, Pickles A, Charman treatment for pediatric anxiety 18. van Steensel FJ, Deutschman AA,
T, Chandler S, Loucas T, Baird G. disorders. In: Vasa RA, Roy AK, eds. Bögels SM. Examining the Screen
Psychiatric disorders in children Pediatric Anxiety Disorders, A Clinical for Child Anxiety-Related Emotional
with autism spectrum disorders: Guide. New York, NY: Springer Disorder-71 as an assessment
prevalence, comorbidity, and Publishing; 2013:269–287 tool for anxiety in children with
associated factors in a population- high-functioning autism spectrum
10. Golnik A, Ireland M, Borowsky IW.
derived sample. J Am Acad Child disorders. Autism. 2013;17(6):681–692
Medical homes for children with
Adolesc Psychiatry. 2008;47(8):
autism: a physician survey. Pediatrics. 19. White SW, Lerner MD, McLeod BD,
921–929
2009;123(3):966–971 et al. Anxiety in youth with and
3. Kerns CM, Kendall PC, Zickgraf H, 11. White SW, Oswald D, Ollendick T, Scahill without autism spectrum disorder:
Franklin ME, Miller J, Herrington J. Not L. Anxiety in children and adolescents examination of factorial equivalence.
to be overshadowed or overlooked: with autism spectrum disorders. Clin Behav Ther. 2015;46(1):40–53
functional impairments associated Psychol Rev. 2009;29(3):216–229 20. Magiati I, Chan JI, Tan WJ, Poon KK.
with comorbid anxiety disorders
12. Wood JJ, Gadow KD. Exploring the Do non-referred young people with
in youth with ASD. Behav Ther.
nature and function of anxiety in youth autism spectrum disorders and their
2015;46(1):29–39
with autism spectrum disorders. caregivers agree when reporting
4. van Steensel FJ, Bögels SM, Perrin Clin Psychol Sci Pract. 2010;17(4): anxiety symptoms? A preliminary
S. Anxiety disorders in children and 281–292 investigation using the Spence
adolescents with autistic spectrum Children’s Anxiety Scale. Res Autism
disorders: a meta-analysis. Clin Child 13. Davis TE, Moree BN, Dempsey T, et al. Spectr Disord. 2014;8(5):546–558
Fam Psychol Rev. 2011;14(3):302–317 The effect of communication deficits
on anxiety symptoms in infants 21. Wigham S, McConachie H. Systematic
5. Chiri G, Warfield ME. Unmet need and and toddlers with ASD. Behav Ther. review of the properties of tools
problems accessing core health care 2012;43(1):142–152 used to measure outcomes in anxiety
services for children with autism intervention studies for children with
spectrum disorder. Matern Child 14. Losh M, Capps L. Understanding of autism spectrum disorders. PLoS One.
Health J. 2012;16(5):1081–1091 emotional experience in autism: 2014;9(1):e85268
insights from the personal accounts of
6. Vasa RA, Carroll LM, Nozzolillo AA, et al. high-functioning children with autism. 22. Lecavalier L, Wood JJ, Halladay AK, et
A systematic review of treatments for Dev Psychol. 2006;42(5):809–818 al. Measuring anxiety as a treatment
anxiety in youth with autism spectrum endpoint in youth with autism
disorders. J Autism Dev Disord. 15. Ozsivadjian A, Knott F, Magiati I. spectrum disorder. J Autism Dev
2014;44(12):3215–3229 Parent and child perspectives on Disord. 2014;44(5):1128–1143
the nature of anxiety in children and
7. Mohatt JW, Keller AE, Walkup JT. young people with autism spectrum 23. Kerns CM, Maddox BB, Kendall PC,
Psychopharmacology of pediatric disorders: a focus group study. Autism. et al. Brief measures of anxiety in
anxiety disorders. In: Vasa RA, Roy AK, 2012;16(2):107–121 non-treatment-seeking youth with
eds. Pediatric Anxiety Disorders, A autism spectrum disorder. Autism.
Clinical Guide. New York, NY: Springer 16. Negreiros J, Miller LD. The role of 2015;19(8):969–979
Publishing; 2013:289–316 parenting in childhood anxiety:
etiological factors and treatment 24. American Psychiatric Association.
8. Strawn JR, Welge JA, Wehry AM, implications. Clin Psychol. Diagnostic and Statistical Manual of
Keeshin B, Rynn MA. Efficacy and 2014;21(1):3–7 Mental Disorders. 5th ed. Washington,
Downloaded from www.aappublications.org/news by guest on January 25, 2020
S122 VASA et alDC: American Psychiatric Association; 32. Storch EA, Larson MJ, Ehrenreich-May for people with autism spectrum
2013 J, et al. Peer victimization in youth disorder (ASD): a multinational
with autism spectrum disorders and study. Psychopharmacology (Berl).
25. Kerns CM, Kendall PC, Berry L, et al. co-occurring anxiety: relations with 2014;231(6):999–1009
Traditional and atypical presentations psychopathology and loneliness. J Dev
of anxiety in youth with autism 39. Walkup J, Labellarte M. Complications
Phys Disabil. 2012;24(6):575–590 of SSRI treatment. J Child Adolesc
spectrum disorder. J Autism Dev
Disord. 2014;44(11):2851–2861 33. Dabrowska A, Pisula E. Parenting Psychopharmacol. 2001;11(1):1–4
stress and coping styles in mothers 40. Guénolé F, Godbout R, Nicolas A, Franco
26. Kreiser NL, White SW. Assessment and fathers of pre-school children with P, Claustrat B, Baleyte JM. Melatonin
of social anxiety in children and autism and Down syndrome. J Intellect for disordered sleep in individuals
adolescents with autism spectrum Disabil Res. 2010;54(3):266–280 with autism spectrum disorders:
disorder. Clin Psychol Sci Pract. systematic review and discussion.
34. Cassidy A, McConkey R, Kennedy-
2014;21(1):18–31 Sleep Med Rev. 2011;15(6):379–387
Truesdale M, Slevin E. Preschoolers
27. Lidstone J, Uljarević M, Sullivan J, et with autism spectrum disorders: the 41. Nguyen M, Tharani S, Rahmani M,
al. Relations among restricted and impact on families and the supports Shapiro M. A review of the use of
repetitive behaviors, anxiety and available to them. Early Child Dev Care. clonidine as a sleep aid in the child
sensory features in children with 2008;178(2):115–128 and adolescent population. Clin Pediatr
autism spectrum disorders. Res 35. Ung D, Selles R, Small BJ, Storch (Phila). 2014;53(3):211–216
Autism Spectr Disord. 2014;8(2): EA. A systematic review and meta- 42. Ji N, Findling RL. An update on
82–92 analysis of cognitive-behavioral pharmacotherapy for autism
28. Buie T, Campbell DB, Fuchs GJ III, et al. therapy for anxiety in youth with spectrum disorder in children and
Evaluation, diagnosis, and treatment high-functioning autism spectrum adolescents. Curr Opin Psychiatry.
of gastrointestinal disorders in disorders. Child Psychiatry Hum Dev. 2015;28(2):91–101
individuals with ASDs: a consensus 2015;46(4):533–547
43. Politte LC, Henry CA, McDougle CJ.
report. Pediatrics. 2010;125(1 suppl 36. Lickel A, MacLean WE Jr, Blakeley- Psychopharmacological interventions
1):S1–S18 Smith A, Hepburn S. Assessment of in autism spectrum disorder. Harv Rev
the prerequisite skills for cognitive Psychiatry. 2014;22(2):76–92
29. Kotagal S, Broomall E. Sleep in
behavioral therapy in children
children with autism spectrum 44. Mahajan R, Bernal MP, Panzer R, et
with and without autism spectrum
disorder. Pediatr Neurol. al; Autism Speaks Autism Treatment
disorders. J Autism Dev Disord.
2012;47(4):242–251 Network Psychopharmacology
2012;42(6):992–1000
Committee. Clinical practice pathways
30. Thompson SA, Duncan JS, 37. Hagopian LP, Jennett HK. Behavioral for evaluation and medication choice
Smith SJ. Partial seizures assessment and treatment for anxiety for attention-deficit/hyperactivity
presenting as panic attacks. BMJ. for those with autism spectrum disorder symptoms in autism
2000;321(7267):1002–1003 disorder. In: Davis TE, White SW, spectrum disorders. Pediatrics.
Ollendick TH, eds. Handbook of Autism 2012;130(2 suppl 2):S125–S138
31. Ashburner J, Ziviani J, Rodger S.
and Anxiety. Basel, Switzerland:
Surviving in the mainstream: capacity 45. McGuire K, Fung LK, Hagopian L, et
Springer International Publishing;
of children with autism spectrum al. Irritability and problem behaviors
2014:155–169
disorders to perform academically and in the child with autism spectrum
regulate their emotions and behavior 38. Hsia Y, Wong AY, Murphy DG, disorder: a practice pathway for
at school. Res Autism Spectr Disord. Simonoff E, Buitelaar JK, Wong IC. pediatric primary care. Pediatrics.
2010;4(1):18–27 Psychopharmacological prescriptions 2016;137(suppl 2)e20152851L
Downloaded from www.aappublications.org/news by guest on January 25, 2020
PEDIATRICS Volume 137, number S2, February 2016 S123Assessment and Treatment of Anxiety in Youth With Autism Spectrum
Disorders
Roma A. Vasa, Micah O. Mazurek, Rajneesh Mahajan, Amanda E. Bennett, Maria
Pilar Bernal, Alixandra A. Nozzolillo, L. Eugene Arnold and Daniel L. Coury
Pediatrics 2016;137;S115
DOI: 10.1542/peds.2015-2851J
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/137/Supplement_2/S115
References This article cites 40 articles, 4 of which you can access for free at:
http://pediatrics.aappublications.org/content/137/Supplement_2/S115
#BIBL
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on January 25, 2020Assessment and Treatment of Anxiety in Youth With Autism Spectrum
Disorders
Roma A. Vasa, Micah O. Mazurek, Rajneesh Mahajan, Amanda E. Bennett, Maria
Pilar Bernal, Alixandra A. Nozzolillo, L. Eugene Arnold and Daniel L. Coury
Pediatrics 2016;137;S115
DOI: 10.1542/peds.2015-2851J
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/137/Supplement_2/S115
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,
60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print ISSN:
1073-0397.
Downloaded from www.aappublications.org/news by guest on January 25, 2020You can also read