Behavioral Symptoms in Dementia - Trey Bateman, MD, MPH Assistant Professor of Neurology, WFSOM Staff Behavioral Neurologist, Salisbury VAMC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Behavioral Symptoms in Dementia Trey Bateman, MD, MPH Assistant Professor of Neurology, WFSOM Staff Behavioral Neurologist, Salisbury VAMC
Overview
• Common language
• MCI and dementia, specific syndromes, behavioral symptoms
• Different syndromes, different symptoms
• Meds can (and often are) part of the problem
• What we can treat and how
• When to seek physician help
• Monitoring medication response and working as a team
2/3/202
3
1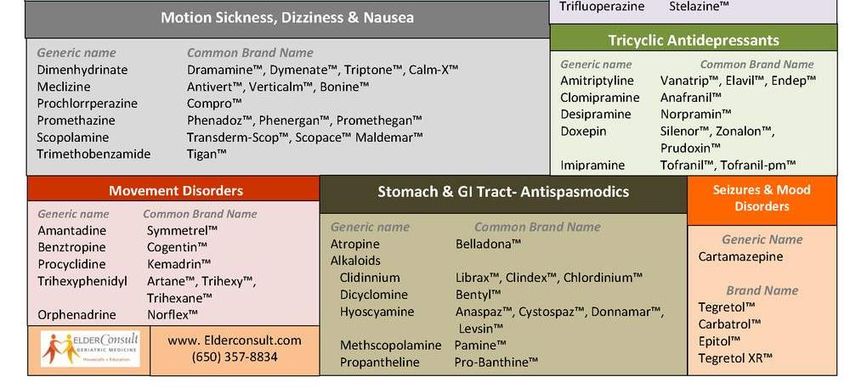
Cognitive Decline
Cognitive Decline
MCI Mild Instrumental ADLs impacted (independent
- Cognitive changes living): driving, cooking, cleaning, finances
concerning to
patient / others
Basic ADLs impacted (physical needs): feeding,
- Low scores on tests Moderate dressing, personal hygiene
- No major decline in
daily activities
Dementia
- Cognitive changes concerning to Severe Fully dependent
patient / others
- Low scores on tests
- Decline in daily activities
Time (years)
2/3/202
4
1
Behavior is what we do that others can observe and measure – good and bad.
We are going to focus on “challenging behaviors”
Behaviors that keep people from successfully participating in their daily life
Behaviors often serve a purpose and can communicate a need.
I’m using the term “behavioral symptoms”
Common synonyms are
- Behavioral and psychological symptoms of dementia (BPSD)
- Neuropsychiatric symptoms (NPS)
2/3/202
5
1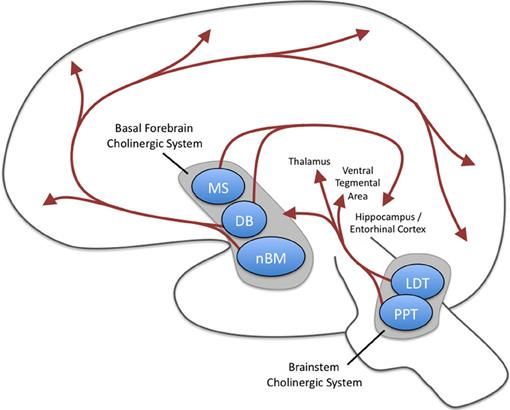
Depression Anxiety Elation Apathy
Agitation/ Motor
Irritability Disinhibition
Aggression Behaviors
Nighttime Appetite/
Delusions Hallucinations
Behaviors Eating
2/3/202
6
1Depression Anxiety Elation
Depression
- Down, depressed, hopeless
- Persistent, not just for a few hours
Anxiety
- Feeling excessively tense
- Excessive nervousness
- Excessive worry
Elation
- Appear to act or feel too good
- Excessively happy
Emotion dysregulation - Talks “big” or grandiose
- Childish, laughs inappropriately
2/3/202
7
1Apathy
Decreased interest / motivation
- Less interested in usual activities
- Less spontaneous
- Less likely to initiate conversation
- Can occur with or without depression
2/3/202
8
1Agitation Irritability
- Excessive motor activity, verbal - Cranky and impatient, difficulty coping with delays
or physical aggression - Rapid changes in mood
- Resistance to care - Bad temper, “flies off the handle” easily
Motor Behaviors
- Repetitive activities,
handling buttons,
Agitation/ Motor wrapping string
Irritability
Aggression Behaviors - Paces without purpose
Impulse Control
2/3/202
9
1Socially inappropriate / acting impulsively
- Excessively familiar with strangers Disinhibition
- Insensitive or hurtful remarks
- Talking openly of private matters
2/3/202
10
1Delusions Hallucinations
- Fixed, false beliefs - Hearing voices
- Stealing from them or planning them - Talks to people not there
harm in some way - Sees things not there
- Misidentifies spouse, child - Feels things not there
- Fears of abandonment - Smells things not there
- Can be simple (shadows) or
Psychosis complex (children)
- Can know they’re not real, or fully
believe they are
Delusions Hallucinations
2/3/202
11
1Too much, too little,
change in preferences
Too much, too little, acting out dreams
Nighttime Appetite/
Behaviors Eating
2/3/202
12
1Depression Anxiety Elation Apathy
Agitation/ Motor
Irritability Disinhibition
Aggression Behaviors
Nighttime Appetite/
Delusions Hallucinations
Behaviors Eating
2/3/202
13
1Behavioral Symptoms
• Many of these overlap
• Most helpful for medical people is just to get your description.
It’s our job to figure out…
• Delusion or false memory
• Anxiety or motor agitation
• Apathy…depressed or not?
• Measurement aided by standardized questionnaires
2/3/202
14
1Behavioral symptoms are a stronger predictor of
caregiver distress than cognition
61% of symptoms reported to be moderately to severely
distressing by caregivers
This, more than presence of a symptom, predicts future
placement outside of the home
2/3/202 Kaufer et al, J. Am. Geriatr. Soc, 1998;46:210-215, Kaufer et al, J. Am. Geriatr. Soc, 1998, Mittleman et al, JAMA, 1996
15
1Alzheimer’s disease and vascular
dementia
• Two most common causes of dementia, behavioral profiles similar
• Majority will experience a clinically significant symptom
• Early stages
• depression, anxiety, apathy, irritability, agitation predominate
• Moderate to severe stages
• delusions/hallucinations, sleep and appetite changes, agitation becomes very
common
2/3/202 Fuh J-L, Wang S-J, Cummings JL: Neuropsychiatric profiles in patients with Alzheimer’s disease and vascular dementia.
16
1 Journal of Neurology, Neurosurgery & Psychiatry 2005; 76:1337–1341Lewy Body Dementias
• 2nd most common
neurodegenerative dementia
• Terminology confusing
• LBD = PDD or DLB
• Behavioral presentations
COMMON
• Hallucinations, delusions,
anxiety, sleep, irritability, apathy
2/3/202 Galvin J: Lewy Body Dementia. Practical Neurology 2019; 67–71
1Frontotemporal Dementia
(FTD)
• More challenging behaviors early
on compared to Alzheimer’s
disease and vascular dementia
Behavioral variant Language variants
• Apathy *very* common (>75%)
• Appetite changes, disinhibition,
motor activity common, agitation, - Loss of - Two types
anxiety common (40-50%) sympathy - Each with
- Apathy prominent early
• Psychosis rare, but more likely in - Craving language
some genetic variants carbs/sweets changes
• Compared to DLB where common - Ritualistic - Less behavioral
behaviors
- Socially
inappropriate
2/3/202 1. Banks SJ, Weintraub S. J Geriatr Psychiatry Neurol. 2008;21:133–141. 2. Fuh J-L, Wang S-J, Cummings JL. Journal of
18
1 Neurology, Neurosurgery & Psychiatry. 2005;76:1337–1341.Verbal
Aggression
To Treat…or Not? Responsive to Not responsive
Medications to medication
• Not all behaviors need to be Pain
Unmet care
needs
treated
• Not harmful
• Infrequent Psychosis Boredom
• Easily re-directed
• Does not contribute to distress Depression Powerlessness
• Medications may not be
effective Overstimulation
Impulsivity
2/3/202
19
1First Things First
• Assess Safety
• Some things must be treated more promptly
• Consider physical causes
• Especially when changes are sudden
• Infection, pain/discomfort, sensory problems, poor sleep
• Medications
2/3/202
20
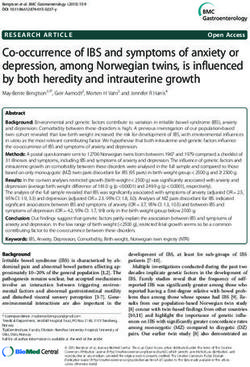
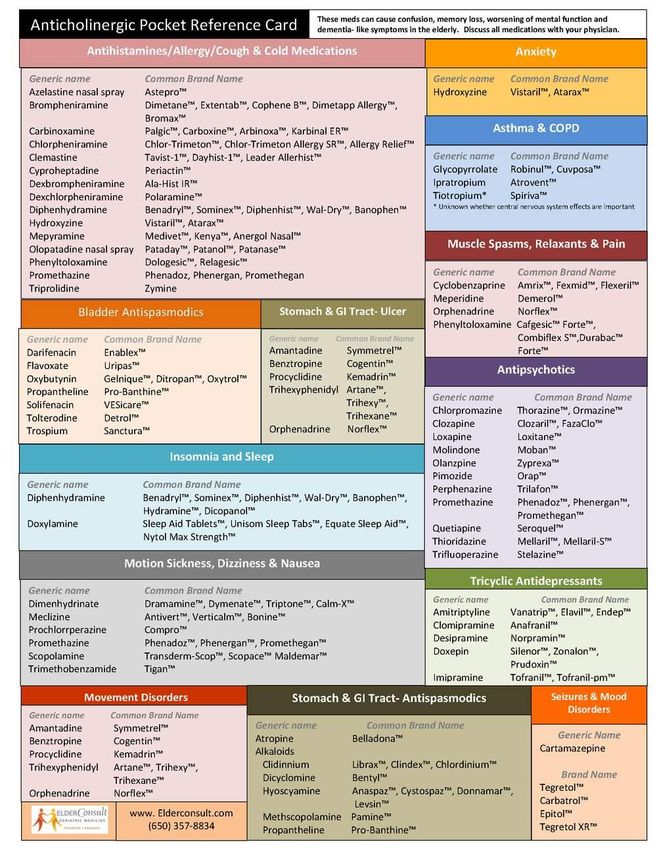
1“Anti-cholinergic”
medications
• Lots of drugs
• Sometimes benefit outweighs
harm, but always important to
consider
2/3/202
21
12/3/202 Figure from Newman et al. (2012). Cholinergic modulation of cognitive processing: Insights drawn from computational
22
1 models. Frontiers in behavioral neuroscience. 6. 24.2/3/202
23
12/3/202
24
12/3/202
25
12/3/202
26
12/3/202
27
12/3/202
28
1Worst offenders
Drug Use Better options
Benadryl, Nyquil, anything PM Sleep, allergies Trazodone (sleep), Claritin
(allergies)
Benzodiazepines Anxiety, sleep Buspar (buspirone; anxiety), SSRI
Oxybutinin Urinary incontinence Myrbetriq
Meclizine (antivert) and
Dimenhydrinate (meclizine)
Paxil (Paroxetine), TCA Depression, TCAs used off label Any SSRI other than Paxil
antidepressants (amitriptyline) for pain, headache, sleep
Muscle relaxers -- Heat, physical therapy
Hycosamine, dicyclomine Anti-spasmodics (stomach Dietary modification, good bowel
cramps) regimen
2/3/202
29
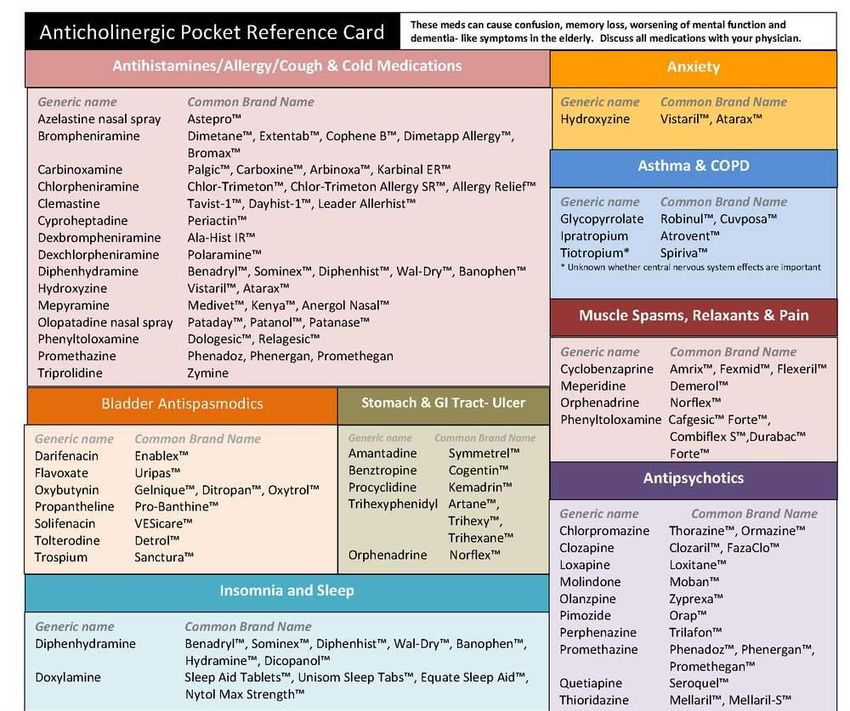
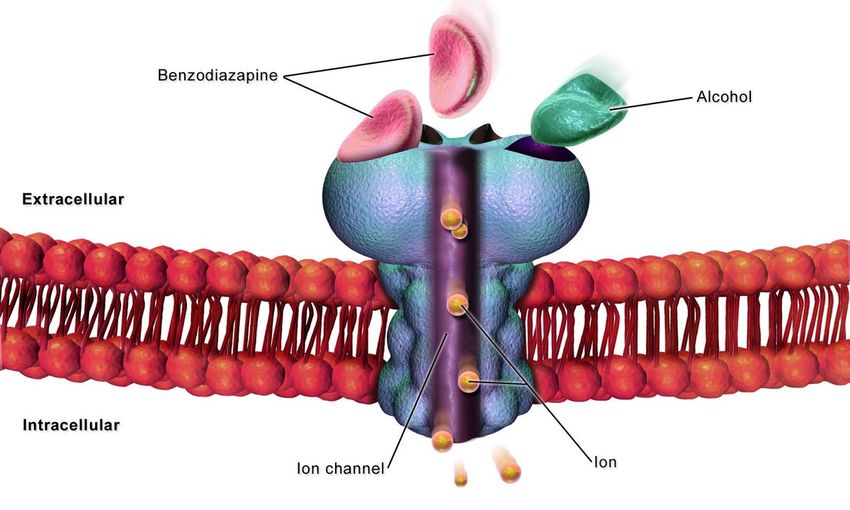
1Benzodiazepines and Ambien
(zolpidem)
• Almost always a bad idea
• Falls, cognitive worsening,
pneumonia
• Exceptions to every rule..
• Short-term crippling anxiety and
panic, severe REM behavior
disorder
• If chronic use, often takes a
long time to get off safely "File:Cell GABA Receptor.png" by BruceBlaus is licensed with CC BY-SA 4.0. To view a copy
of this license, visit https://creativecommons.org/licenses/by-sa/4.0
2/3/202 Rochon PA, Vozoris N, Gill SS. The harms of benzodiazepines for patients with dementia. CMAJ. 2017;189:E517–E518.
30
1Approach to treatment
• First: safety, determine if treatment necessary
• Second: reversible causes
• Third: medications
• Sometimes depends on the diagnosis
• LBD: AchE first line, sometimes may need to “break the rules” and use
medications like benzodiazepines, stimulants
• FTD: avoid AchE
• Often, management predicated on symptoms
2/3/202
31
1Psychosis
Anti-
depressants
Agitation
SSRIs
Aggression
- Sertraline (Zoloft)
- Citalopram (Celexa) Depression
- Escitalopram (Lexapro)
Anxiety
*SNRIs
- Venlafaxine (Effexor)
* Apathy
- Bupropion (Wellbutrin)
Insomnia
REM behavior disorder
2/3/202
32
1Psychosis
Agitation
Aggression
Anti-psychotics
Depression
Risperidone (Risperdal) Anxiety
Aripiprazole (Abilify)
Quetiapine (Seroquel)
Olanzapine (Zyprexa) Apathy
Insomnia
*LBD: sensitivity to antipsychotics, so often stick with
REM behavior disorder
Quetiapine (Seroquel), Pimavanserin (Nuplazid)
2/3/202
33
1Psychosis
Agitation
Aggression
Depression
Cholinesterase Anxiety
inhibitors
Apathy
Donepezil (Aricept) Insomnia
Rivastigmine (Exelon)
Galantamine (Razadyne) REM behavior disorder
2/3/202
34
1Psychosis
Agitation
Aggression
Depression
Anxiety
Apathy
Trazodone/ Insomnia
Mirtazapine
REM behavior disorder
Melatonin
2/3/202
35
1Psychosis
Namenda Agitation
(Memantine)
Aggression
Mixed evidence
Depression
May reduce escalation of anti-
psychotic dose Anxiety
Apathy
Insomnia
REM behavior disorder
2/3/202
36
1Psychosis
Agitation
Aggression
Depression
Benzodiazepines
Anxiety
Apathy
Insomnia
REM behavior disorder
2/3/202
37
1Psychosis
Agitation
Aggression
Depression
Anxiety
Stimulants Apathy
Insomnia
REM behavior disorder
LBD specific: severe daytime
somnolence without another cause
2/3/202
38
1Sexually inappropriate
behavior
• Two types
• Intimacy seeking
• Disinhibited
• Treatment: ethnical balance,
especially in residential care
• Non-pharm first: re-direct,
clothes that open in back,
alternative activity
2/3/202 Tucker I: Management of inappropriate sexual behaviors in dementia: a literature review. International Psychogeriatrics
39
1 2010; 22:683–92When can we help?
When the symptoms are disruptive in your life
or when you feel like you’re needing help
2/3/202
40
1Monitoring response
• Really depends on medication and target behavior
• Rely a lot on data outside of treating those with dementia
• E.g., Depression, sometimes 6-8 weeks in non-dementia trials
• At this point, the “gold standard” for outcomes ultimately boils
down to patient and informant report
2/3/202
41
1Partnering with clinicians
• The person with dementia is my patient, but you have to care
for the caregiver
• Put your own oxygen mask on first
• Sleep is really important…
• Shared decision making is important
• Education is key; some things we can’t treat well
• May take several medication trials to find effective combination
2/3/202
42
1Thank you
You can also read