Behinderung und internationale Entwicklung Disability and International Development - Frühkindliche Entwicklung und Inklusion Early Child ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
27. JAHRGANG AUSGABE 1/2016
27ND YEAR ISSUE 1/2016
Behinderung und internationale Entwicklung
Disability and
International Development
Frühkindliche Entwicklung und Inklusion
Early Child Development and InclusionInhaltsverzeichnis Impressum/Masthead
Table of Contents Behinderung und internationale Entwicklung
Disability and International Development
Herausgeber/Editor
Behinderung und Entwicklungszusammenarbeit e.V./
Disability and Development Cooperation
Anschrift/Address
Wandastr. 9, 45136 Essen
Editorial .......................................................................3 Tel.: +49 (0)201/17 89 123
Fax: +49 (0)201/17 89 026
E-Mail: info@inie-inid.org
Schwerpunkt/Focus Internet: www.zbdw.de
Frühkindliche Entwicklung und Inklusion Für blinde und sehbehinderte Menschen ist die Zeit-
Early Child Development and Inclusion
schrift im Internet erhältlich./For persons with visual im-
pairment, an electronic version of the journal is
Early Intervention (EI) for Children with available at www.zbdw.de
Deafblindness in India: Barriers and Enablers Redaktionsgruppe/Editorial Board
Akhil S. Paul/Biju Mathew/Uttam Kumar/Sachin Rizal/ Isabella Bertmann, Christine Bruker, Anne Ernst,
Atul Jaiswal ....................................................................4
Dr. Thorsten Hinz, Jana Offergeld,
Prof. Dr. Sabine Schäper, Gabriele Weigt
Women, Motherhood, Children and Disabled Schriftleitung/Editorship
Persons – Mainstreaming Disability in Development in Gabriele Weigt
Pakistan Redaktionsassistenz/Editorial Assistance
Kozue Nagata...............................................................12 Katharina Silter
Gestaltung/Layout
Amund Schmidt
Needs of Families Impacted by Disability: Druck/Print
A Scoping Review
Druckerei Nolte, Iserlohn
Reshma Parvin Nuri/Heather Michelle Aldersey ..............20
Bankverbindung/Bank Details
Bank für Sozialwirtschaft
BIC: BFSWDE33XXX
Kurzmeldungen/Notes..............................................29 IBAN: DE19 3702 0500 0008 0407 02
Die Zeitschrift Behinderung und internationale Entwick-
lung ist eine Pubilikation des Instituts für inklusive Ent-
Literatur/Reviews .....................................................34 wicklung. Das Institut wird getragen von Behinderung
und Entwicklungszusammenarbeit e.V.
The journal Disability and International Development is a
publication of the Institute for Inclusive Development. The
Veranstaltungen/Events............................................38
Institut ist part of Disability and Development Caoperation.
Hinweis: Für den Inhalt der Artikel sind die AutorInnen
verantwortlich. Veröffentlichte Artikel stellen nicht un-
bedingt die Meinung der Redaktion dar. Die Veröffentli-
chung von Beiträgen aus der Zeitschrift in anderen Pub-
likationen ist möglich, wenn dies unter vollständiger
Quellenangabe geschieht und ein Belegexemplar über-
sandt wird.
Please note that the authors are responsible for the
content of the articles. Published articles do not neces-
sarily reflect the opinion of the editorial board. Papers
published in the journal Disability and International De-
velopment may be reprinted in other publications if cor-
rectly cited and if a copy is forwarded to the contact
provided above.
ISSN 2191-6888 (Print)
ISSN 2199-7306 (Internet)
2 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentEDITORIAL
Editorial
Liebe Leserinnen und Leser, Dear Readers,
die besonderen Risiken für die frühkindliche Entwick- living in the Global South implicates special risks for
lung, die mit dem Aufwachsen im Globalen Süden a child's development. Worldwide, more than 200
verbunden sind, sind seit langem bekannt. Weltweit million children under the age of 5 live in conditions
leben mehr als 200 Millionen Kinder unter Bedingun- of poverty, health risks, and malnutrition. The lack of
gen von Armut, gesundheitlichen Risiken, Unter- und equal access to health care and pedagogical sup-
Fehlernährung. Die medizinische Versorgung und port in many low income countries negatively influ-
pädagogische Unterstützung, die sie für eine gesunde ences early cognitive and socio-emotional develop-
Entwicklung brauchen, bleiben ihnen vielfach vorent- ment. Identifying special needs as early as possible
halten. Dieses Schwerpunktheft bietet drei Beiträge zu and providing adequate support are crucial aspects
diesem Themenbereich: for growing-up and healthy development.
Akhil S. Paul, Biju Mathew, Uttam Kumar, Sachin Rizal Akhil S. Paul, Biju Mathew, Uttam Kumar, Sachin Ri-
und Atul Jaiswal stellen die Situation von Menschen in zal, and Atul Jaiswal focus on the situation of people
Indien vor, die von Taubblindheit betroffen sind, und living with deafblindness in India and describe barri-
zeigen die Chancen auf, die frühe Hilfen für Kinder ers and enablers in providing early intervention pro-
und ihre Familien beinhalten. Kozue Nagata öffnet grams for this special group. Kozue Nagata opens
die Perspektive in Richtung des Diskurses um Intersek- the view into the discussion on intersectionality by
tionalität. Basierend auf vorliegenden Forschungser- focusing on gender, motherhood and disability as
kenntnissen und einer Befragung von Frauen mit Be- closely interrelated factors of social exclusion. The
hinderungen in Pakistan werden Aspekte von Gender, presented research project analysed available statis-
Mutterschaft und Behinderung in ihren Wechselwir- tics and studies, and assessed the voices of Pakistani
kungen als Faktoren sozialer Ausgrenzung diskutiert. women with disabilities, drawing attention to the
Der dritte Beitrag von Reshma Parvin Nuri und Heat- connection of disability and development from a
her Michelle Aldersey widmet sich den Unterstütz- gender perspective. The third article reviews needs
ungsbedarfen von Familien, die Behinderungserfah- of families with disability experiences. Reshma Parvin
rungen haben. Durch eine systematische Literatur- Nuri and Heather Michelle Aldersey conducted a sys-
analyse wurden die zentralen Bedürfnisse dieser Fa- tematic analysis of literature to identify families'
milien herausgearbeitet. Sie beziehen sich auf Infor- needs regarding information and service provision
mationsbedarfe und die Gestaltung von Unterstütz- as well as everyday life challenges of the families.
ungsarrangements, zugleich aber auch auf Anforde-
rungen an die alltägliche Lebensgestaltung als Famili- These three articles demonstrate that early child-
en mit Angehörigen mit Behinderungen. Die Beiträge hood intervention can contribute to individual devel-
unterstreichen die Bedeutung früher Unterstützung, opment as well as to enabling families to envision a
um Familien zu stärken und zu befähigen, positive positive future with their children with disabilities.
Zukunftsperspektiven zu entwickeln.
We wish you a good reading.
Wir wünschen eine anregende Lektüre.
Your editorial board
Ihr Redaktionsteam
Behinderung und internationale Entwicklung 1/2016 3
Disability and International DevelopmentARTIKEL/ARTICLE
Early Intervention (EI) for Children with Deafblindness in India:
Barriers and Enablers
Akhil S. Paul/Biju Mathew/Uttam Kumar/Sachin Rizal/Atul Jaiswal
Research on early intervention programs meeting sensory disabilities is very limited in India and at a global
level. Sense International India (SII) as a national level organisation developed a model of EI services speci-
fied for persons with deafblindness in 2012. This paper uses the SII-EI model as a case study to highlight the
barriers and enablers in providing EI services for children with deafblindness in India.
Introduction
could be more than 500,000 persons with
Deafblindness is a disability involving a combi- deafblindness in India (Sense International In-
nation of varying degrees of hearing and visual dia 2015). Overall, India is home to 26.8 mil-
impairment causing difficulties with communi- lion persons with disabilities (PwDs) (Census
cation, access to information, and mobility 2011). Despite having progressive disability
(Sense International India n.d.). It is a hetero- policies, people with disabilities in India are
geneous disorder also referred to as “dual sen- subject to multiple deprivations and limited op-
sory loss” (Dammeyer 2014) encompassing a portunities in several dimensions of their lives
spectrum from mild loss in hearing and vision and have limited awareness of entitlements
to total deafness and blindness depending and services available by law for people with
upon its varied combinations. It could be con- disabilities (Menon/Parish/Rose 2014). World
genital or acquired and varies with regard to Bank report in 2009 reveals that persons with
medical aetiology, age of onset, severity of vi- disabilities are excluded from exercising their
sion and hearing loss, and presence of associ- human rights and achieving higher levels of hu-
ated medical conditions. Aetiology includes man development (O'Keefe 2009). They often
pre-, peri- and postnatal causes, as well as ge- face barriers to information and services due to
netic and chromosomal disorders. Prenatal the ignorance and negative attitudes of society
causes include infections of the foetus with ru- and individuals (Barnes/Mercer 2003). Among
bella or cytomegalovirus. Perinatal causes in- this population, children with disabilities are the
clude low birth weight and postnatal causes in- most vulnerable groups who need proper and
clude intoxication and infections, such as men- timely interventions to avert their disability and/
ingitis. This peculiar combination of hearing or its impact on their lives. The United Nations
and vision loss under the ambit of dual sensory Children's Emergency Fund (UNICEF) and the
loss results in a unique condition that is more Institute for Statistics’ (UIS) South and East
disabling than the sum of its impairments Asian Regional Report highlighted that approxi-
(Dammeyer 2014). mately 11.9 million children with disabilities are
It is a low incidence disability, however, given out of school in India (UNICEF-UIS 2014).
the morbidity pattern in most low/middle in- Within this larger population of children with
come countries due to advancement in medical disabilities who are still underserved and ex-
services, it is estimated that the incidence of cluded are also children with deafblindness.
deafblindness is significant and likely to in- India ratified the United Nations Convention
crease. Earlier children born with complex on the Rights of Persons with Disabilities
medical conditions could not survive due to lack (UNCRPD) in 2007 and is trying to harmonise
of advance medical services in less developed the laws and policies with the convention. One
cities in India. However, medical services have key step towards this harmonisation is revamp-
improved and has resulted into their survival of ing the older welfare -law The Persons with Dis-
these children with complex medical conditions, abilities Act 1995 into the newer rights-based
however, most often they have conditions with The Rights of Persons with Disabilities Bill 2014
developmental delay and other sensory issues (EPW 2014). Deafblindness has not been recog-
such as in deafblindness. nised as a separate category of disability in the
There is an estimation of 2.5 million people current disability law The Persons with Disabili-
with deafblindness worldwide and the majority ties Act 1995 in India. Due to the non-recogni-
of them experience high levels of poverty and tion, they are deprived of government schemes
social exclusion with limited access to resources and social security benefits. Once enacted by
(Source n.d.). Estimates indicate that there legislature of India, the newly drafted bill would
4 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentARTIKEL/ARTICLE
replace the current disability act, and cover 19 Methods
specific impairments including deafblindness
(PRS 2015). This paper uses the SII-EI Model as a case study
Because 95 % of what one learns about the to highlight the barriers and enablers in provid-
world comes through sight and hearing, chal- ing EI services for children with deafblindness in
lenges in communication, mobility and access- India. The paper relies on a review of literature
ing information makes deafblindness one of the on EI for deafblindness, EI project reports and
most isolating impairments and affects the documents of Sense India to highlight barriers
whole development of the child. Identification and enablers in EI services. Online database
at an early age and access to need-based EI sources of CINAHL, MEDLINE, PubMed and
plays a vital role in the development of each Google Scholar were used for secondary litera-
child with deafblindness. EI services for young ture review. The keywords used to retrieve the
children (aged 0-6 years) through hearing relevant articles included early intervention,
screening, visual testing, multisensory stimula- deafblindness, deaf-blind, children, India, bar-
tion, functional visual training, speech therapy riers, enablers or facilitators. Relevant reports of
and developmental therapeutic interventions the World Health Organisation (WHO), the
enhances the chances of reaching maximum United Nations Development Fund (UNDP), the
potential for children with deafblindness signifi- United Nations Children's Emergency Fund
cantly (Sense International India n.d.). (UNICEF) and the UNESCO Institute for Statis-
Sense International India (SII) is the first and tics (UIS) are also used along with the SII publi-
only national level organisation working with cations.
deafblind people across India since 1997. SII is The article is divided into three main sec-
working in 23 states of India through a network tions. The first section gives a brief introduction
of 57 partner organisations, supporting over on the development of EI services and their sig-
71,500 persons with deafblindness in some of nificance for children with deafblindness in the
the poorest areas of the country for the last 18 Indian context. In the second section, SII-EI
years (Sense International India 2015). The SII model for children with deafblindness will be
theory of change imbibes two main principles – introduced and in the third section, barriers and
partnership with local grassroots organisations enablers for deafblind specific EI services are
and capacity building to transfer skills and described and suggestions on how EI programs
knowledge to partner organisations and profes- can be planned and implemented effectively
sionals, so that they can work with the and efficiently are mentioned. It is acknowl-
deafblind population. SII has been involved in edged that there is a range of project manage-
early identification and intervention since 1998 ment challenges as in any project, however, for
and has worked on community based rehabili- the purposes of this article, the discussion will
tation (CBR) approaches to EI, in order to en- exclusively focus on the barriers and enablers in
sure children with deafblindness get the best EI services specific to children with deafblind-
possible start towards achieving their potential. ness.
Based on the learning and experience, SII de-
veloped its model of EI service delivery in 2012. Early Intervention and its Significance for
This was done in partnership with hospitals and the Deafblind Population
partner organisations. Hospitals were involved Research in the field of deafblindness is limited
to ensure early screening of at-risk new-born (Dammeyer 2014, Danermark/Moller 2008)
children with dual sensory loss and timely inter- and is further limited in the context of EI for
vention to minimise the impact of dual sensory children with deafblindness (Murdoch 2004).
loss. Deafblindness can have many different causes
including poor nutrition or trauma during preg-
Research Question nancy; as a result of the mother having rubella
leading to Congenital Rubella Syndrome; Usher
The paper is guided by the following research Syndrome; or due to an illness such as menin-
question: “What were the barriers and enablers gitis or following premature birth. Effective
in early intervention services for children with early identification & EI services directly influ-
deafblindness in India?” This article will reflect ence the impact of underlying medical impair-
upon EI services for children with deafblindness ments turning into a disabling condition, and
in India and highlight barriers and enablers help to reduce the risks that children with sen-
identified, while implementing projects for EI sory impairments would otherwise face. Early
services following the SII-EI model. intervention also provides long-term benefits to
families and society by reducing mental distress
Behinderung und internationale Entwicklung 1/2016 5
Disability and International DevelopmentARTIKEL/ARTICLE
of families and the risk of the child requiring 2011. SII identified that while there are hospi-
more intensive care (services) later on. It helps tal-based identification programmes for chil-
in promoting parent-child bonding and en- dren with deafness and blindness separately,
hances the caregiving process for the child these programmes missed out on identifying
(Chen/Haney 1995). children with deafblindness. This was also due
One of the major challenges in the field of to the reason that there was lack of reliable
developing deafblind interventions in India are tools for identification of visual impairment and
ill-equipped public systems to identify and diag- hearing loss, especially when children have
nose children at risk of deafblindness at an multiple disabilities. In some cases, visual im-
early age and to provide them EI services in- pairment was diagnosed but the child’s hearing
stantly to avert their level of disabilities. These status remained unknown.
gaps in the public health service delivery in- The pilot programme was set-up in Patna,
clude a lack of neonatal screening and EI sup- Bihar in 2011 with the help of SII’s partner or-
port for children with deafblindness in their cru- ganisation that was already working in the
cial early years. The Government of India initi- state. A collaboration was built with the local
ated a National Child Health Programme hospital that helped in the early identification
Rashtriya Bal Swasthya Karyakram (RBSK) of at-risk new-born children with dual sensory
aimed to reduce child mortality and early iden- loss and timely intervention to minimise the im-
tification as well as intervention for children pact of sensory loss. Main objectives of the EI
from birth to 18 years to cover defects at birth, programme are:
deficiencies, diseases, and development delays i. To identify children at a high risk of
including disability (Ministry of Health and Fam- deafblindness in the age group of 0-6 years;
ily Welfare 2013). The programme was notified ii. To provide necessary support and interven-
in the year 2013, however, the country has not tion to overcome and/or reduce difficulties in
seen much progress in terms of establishing accessing information, communication, mo-
early identification and intervention systems for bility and orientation as early as possible;
children with disabilities. iii.To assist in providing comprehensive home-
The developmental consequences of based and/or centre-based services includ-
deafblindness indicate the need for EI involving ing assessment, and clinical and therapeutic
families, coordinated with specialist interven- services to the children with deafblindness
tion or services (Murdoch 2004). Early interven- including necessary aids and appliances;
tion services need to be set up in partnership iv. To provide support and counselling to the
with hospitals where infants from 0-6 years can families, helping them reduce the feelings of
be screened by doctors with follow-up through isolation, stress and frustration that families
one-to-one training by professionals. However, may experience;
most of the time, especially in rural or distant v. To provide training in motor, communication,
areas, services are practically non-existent or sensory, oro-motor, cognitive, social and ac-
insufficient for young children with deafblind- tivities of daily living (ADL) skills.
ness. Access seems to depend on where the In order to achieve these objectives, the fol-
child lives. This results in precious time being lowing main activities are undertaken:
lost as the first three years of life are the crucial i. Orientation and advanced skill training to
period when maximum learning and develop- educators and field workers in EI for young
ment takes place. infants with deafblindness;
ii. Developing an individualised education plan
The Sense International India Model of (IEP) for each child;
Early Intervention for Children with iii.Training and counselling of family members/
Deafblindness caregivers;
SII has been working with persons with iv. Production of information materials in local
deafblindness for over 18 years, and has languages;
adopted various models like home-based, cen- v. Awareness and sensitisation activities at re-
tre-based, and community-based rehabilitation gional and state level:
programs. Sense India will reach two decades vi. Sensitisation training of medical and para-
of unique service with the children and adults medical professionals.
with deafblindness across the states of India by Based on the learning and experience, the
the year 2017. A focussed EI service with the program was tested and validated and has now
aim of establishing a system of specialist, multi- been expanded in eight additional states
disciplinary support for deafblind babies & chil- (Andhra Pradesh, Goa, Gujarat, Karnataka,
dren and their families was initiated in the year Kerala, Madhya Pradesh, Maharashtra, and Ta-
6 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentARTIKEL/ARTICLE
mil Nadu) in India. The program is being man- females) were screened using the Otoacoustic
aged with the help of SII’s partner organisa- Emission (OAE) technique and 331 children
tions working in the states. The overall process (200 males and 131 females) were enrolled
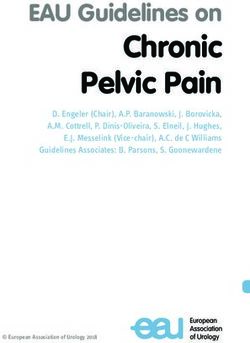
involves field surveys with the help of special into the EI programme to receive services
educators and CBR workers to identify children (Sense International India 2015).
with deafblindness or children at risk of devel- The guidelines are prepared for reference of
oping deafblindness in the community (see Fig- the partner organisations in undertaking the EI
ure 1). activities in their respective project areas (refer
Annexure 2). This also helps
the partner NGOs to follow
a standardised procedure
for undertaking the activity.
Regular onsite trainings and
mentoring support is being
provided by SII experts. The
programme is monitored
regularly with the help of
quantitative and qualitative
indicators like number of
babies assessed, number of
appointments held with EI
specialists, confidence level
of parents to follow the indi-
vidual development plan,
confidence level of EI spe-
cialists to follow the pro-
gress of a child against de-
velopmental milestones in
the individual development
plan. Participatory review
Figure 1: Process steps for the Early Intervention Model
workshops are organised
(Source: Sense International [India] Document on Early Intervention Model 2011)
annually where all the
This is followed by the referral of children stakeholders groups represent themselves. After
identified as at risk of developing deafblindness an agreed period of time, usually 1.5 to 3
to the partner hospital where assessment is car- years, an independent evaluation of the effec-
ried out by medical doctors. After identification tiveness of the pilot EI service is undertaken,
and referral, one-to-one training is provided by with learning shared amongst stakeholders and
qualified deafblind educators or experts. An ob- used to make improvements to the EI services.
servational checklist on visual and hearing be-
haviour is given to all parents that help families Barriers and Enablers
to monitor any deviation from normal develop- The most common challenge found in both re-
ment pattern (refer to Annexure 1). The range search and practice when working with
of services includes family counselling, needs- deafblind population is to communicate with
based training support by trained educators, them. Similarly, it becomes important to be
provision of necessary aids & appliances and aware of the consequences of dual sensory loss
continued medical support. In addition to this, in providing treatment (Southern/Drescher
services are provided to cater for the individual- 2005). The main goal of the SII-EI program is
ised need of each child identified with not merely development of a particular skill or
deafblindness. This includes audiology, family shaping behaviour but to encourage an in-
training, physiotherapy, occupational therapy, creased level of engagement with the world in
clinical psychologist services, nutrition services, general through exploring, imitating, turn tak-
counselling, home visits, assistive technology, ing, anticipation, mutual acceptance and role
speech language therapy, and special educa- modelling. Through the programme it became
tion training. Individualised plans and achieve- apparent that working with children with
ments are revisited periodically to ensure the deafblindness requires particular sets of skills,
individualised intervention plan is appropriate and many educators/professionals experience
and working. Between 2012-2015 (December), challenges in adapting their skills to best bene-
5433 new-born infants (2939 males and 2494 fit these children. Many special educators work-
Behinderung und internationale Entwicklung 1/2016 7
Disability and International DevelopmentARTIKEL/ARTICLE
ing within the EI project reported facing prob- tre. This is also associated with the economic
lems in planning EI services, along with how to situation of the parents. Sometimes the parents
assess; which areas should be given impor- of at risk babies from villages rely more on the
tance; what goal to take; how to and how long Tantriks and Gurus (religious/spiritual healers)
to teach the particular skills to children with than the medical interventions, which leads to
deafblindness. Keeping these factors in mind is the loss of crucial time for EI. Delays in accept-
crucial to the program and its success. The bar- ing their children with dual sensory loss or with
riers and enablers have been classified and de- development delay also add to barriers in pro-
scribed at three levels – community level, part- viding EI to the children. In many parts of the
ner organisation level, and hospital level. country, many people still consider disability as
medical issue, and during the early years, par-
At Community Level ents mostly focus on medical treatment rather
Deafblindness is not yet recognised as a sepa- than intervention. The lack of awareness and
rate disability in India. Lack of recognition of understanding among the parents of the inter-
deafblindness in current disability law deprives ventions such as sensory stimulation, gross-mo-
children with deafblindness in getting appropri- tor/ fine-motor training, activities of daily living
ate EI services for them in government hospi- training and other therapeutic interventions
tals. Moreover, government public health sys- hampers the process of EI. In addition, the ig-
tems are not equipped with skills to identify and norance by medical professionals about these
diagnose children at risk of deafblindness at an interventions also compounds the overall sce-
early age and to provide them EI services on nario.
time. There are hospital-based identification In contrast to the above mentioned barriers,
programmes for children with deafness and/or the enablers are increasing deafblindness
blindness, but these programmes miss out on awareness in the community and among key
identifying children with deafblindness. In addi- stakeholders such as medical and para-medical
tion to this, there is a lack of early reliable professionals. Specific to the SII, the network of
identification of visual and hearing loss in the partner organisations working across 23 states
same child, especially when children have mul- of the country helps in the process of reaching
tiple disabilities like deafblindness. out to the at-risk children through their commu-
In India, there is a cultural practice that a nity based rehabilitation programmes and en-
pregnant woman moves to her parents’ place rolling the child into the nearest available EI
for the delivery of the child, and goes back to programmes.
her husbands’ place after a few months. Due to
this practice, babies identified at risk loose fol- At Partner Organisation Level
low-up care and remain untraced after moving The major barriers faced by partner organisa-
to a different place. In case of weak or low birth tions included difficulty in creating partnerships
weight babies, parents happen to pay attention with hospitals for early screening of children,
to their child’s survival and other health issues and getting referrals from them to EI centre. In
for the first few years and hearing and vision is- addition, lack of man power trained in EI at
sues become evident later. Sometimes, getting partner organisation to provide need-specific EI
consent of the parents for visual/hearing testing services to the identified child is another major
on their new-born becomes difficult and re- barrier. Specific teaching learning materials are
quires counselling. In some places, the society required to be developed for the EI services and
and the family expect the EI services for the service providers need to be trained in develop-
child only from the female trainers due to so- ment of teaching learning materials. Another
cio-cultural issues. In India, there is still a situa- barrier is the lack of time as it takes long to
tion where women (mothers) mostly stay at adapt the environment according to the needs
home to take care of children and home, and of the child, and these children take long time
men go out to work. In this condition, women to show results of the training. However, only
prefer some women worker to come home limited time of services (might be ten hours a
when they are alone. Females are also pre- week or less) could be provided to the children
ferred over males while working with the new- with deafblindness due to constraints of re-
born in home based/CBR services because par- sources in terms of man power and funding.
ents feel females can provide better care to the Enablers at partner organisations’ level are
young baby. the on-going transfer of EI technical skills to
Lack of adequate public transport facilities, their staff and regular support through onsite
especially in rural and difficult terrain areas, mentoring and training on different skills and
make it difficult for parents to reach the EI cen- competencies of EI services. Rapport of the
8 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentARTIKEL/ARTICLE
partner organisations with the local hospitals mation of nearest EI centres.
and its visibility within the community through 3. Sensitisation on the aspects of screening, as-
community based rehabilitation programs also sessment on the needs of persons with
act as enabling factor in EI service delivery. deafblindness, and their referral to the EI
centres at the earliest.
At Hospital Level 4. Proper counselling sessions for the parents
Lack of availability of trained professionals in EI to make them understand the importance of
services directly affects the services. Only the neonatal screening and enhance the coop-
trained professionals are eligible to do OAE eration from parents for screening and later
screening, as neo-natal screening for in receiving intervention for the child.
deafblindness cannot be done like regular 5. Regular training sessions for parents and
screening for deafness or blindness. Other as- other family members to equip them with
sociated health issues like epilepsy in young in- skills and knowledge for providing services
fants affect the screening of vision and hearing at home.
impairment. In addition, costs of OAE machines 6. Ongoing knowledge upgradation of EI staff
and equipment for testing and maintenance members on EI techniques to equip them
are high, which acts as a barrier in delivery of with latest skills and knowledge to provide
EI services. In some cases, where a child is rec- quality level of services to the child.
ognised as having deafblindness and needs 7. Proper data management information sys-
surgery such as a cochlear implant, the costs tem at partner institution level for screened
are high for the family or for the partner or- children, at-risk children, and children who
ganisation and SII to support. Most of the time, have been diagnosed and referred to the
medical professionals are focussed on their nearest EI centre. Project implementers
subject, and tend to ignore the issues which are should take verified permanent address of
not in their domain. For example, an otolaryn- the children screened. This will help to track
gologist will not be much interested in visual the new-born and her/his overall develop-
behaviour or vision-related issues unless it is ment and rehabilitation outcomes from the
very evident. Similarly, the ophthalmologists are date of identification till the level they are
not concerned about hearing capacity. This im- ready for the school education.
pacts the identification at the early age and re-
ferral to the EI service or therapy centres. Limitations of the Study
Enabling factors are willingness of hospitals
and healthcare professionals for the training on The inherent conflict of interest in this paper is
deafblindness and deafblind specific EI services. that the article is written by the SII team based
Their cooperation to develop EI services within upon their own experiences of implementing EI
their hospital infrastructure creates a win-win projects in different parts of India. Worldwide
situation for all the stakeholders. In addition, research on deafblindness is sparse (Dammeyer
advancement in and use of health care technol- 2014, Danermark/Moller 2008) and is further
ogy within hospitals to screen the children at an limited in the context of India. Hence, the paper
early age has facilitated the process of screen- is primarily based on the field-based observa-
ing of children for any at-risk symptoms. tions and experiential learning of implementa-
Sustainability of the EI programs for this tion of EI projects by SII in eight states of India.
unique population is a major challenge at all
three levels. Providing EI services to at-risk in- Summary and Conclusions
fants or children with deafblindness and sup-
porting their families requires substantial in- Providing EI services to infants who are
vestment of efforts, time and resources. deafblind and their families is complicated. Not
The suggestions for developing effective and only do the age, abilities, and needs of each
efficient deafblind specific EI services are: child require an individualised approach, but
1. Awareness programmes for parents, espe- family priorities, local culture and language, lo-
cially new parents, and community members cation, program resources, and state policies
on early identification of developmental de- do also influence the nature of intervention
lay or sensory impairment will enable the services. These complexities emphasise the
parents to identify problems at an earlier need for EI services and the requirement to
age. work together to provide professional develop-
2. Development of Information, Education and ment activities for service providers and educa-
Communication (IEC) materials on early tional and networking opportunities for families
signs of at-risk of deafblindness and infor- of children who are deafblind. There is an ur-
Behinderung und internationale Entwicklung 1/2016 9
Disability and International DevelopmentARTIKEL/ARTICLE
gent need to initiate and reach out to the re- ontological security, and social recognition. Interna-
mote parts to ensure that every child with tional Journal of Audiology, Vol. 47, sup. 2, pp. S119-
deafblindness gets the required intervention on S123.
time. Moreover, children with deafblindness ECONOMIC AND POLITICAL WEEKLY (2014): Disabled
take long time to show results of their training by Lack of Political Will. Editorial- Vol XLIX, No. 2.
and education. Hence a continued and sus- Available at http://www.epw.in/journal/2014/2/edi-
tained program that would bring about trans- torials/disabled-lack-political-will.html. Visited on 07
formation in the lives of children with February 2016.
deafblindness is a must. It is therefore vital for MENON, N./PARISH, S. L./ROSE, R. A. (2014): The “state”
the rehabilitation professionals to be critically of persons with disabilities in India. Journal of Human
cognisant of the various interplaying factors Development and Capabilities, Vol. 15, No. 4, pp.
which act as barriers and enablers in EI services 391-412. Available at http://people.brandeis.edu/
received by children with deafblindness. There ~nmenon/JHDC_pub.pdf. Visited on 07 February
is a need for further research to explore the po- 2016.
tential for improvement in EI programmes. MINISTRY OF HEALTH AND FAMILY WELFARE. (2013):
This paper concludes that comprehensive re- Rashtriya Bal Swasthya Karyakram. National Health
habilitation of children with deafblindness can- Mission. Government of India. Available at http://
not be attained in isolation, but requires a nrhm.gov.in/images/pdf/programmes/RBSK/
multi-pronged approach and timely interven- For_more_information.pdf. Visited on 07 February
tions to facilitate the optimal development of 2016.
the child. It does require a planned approach MURDOCH, H. (2004): Early intervention for children
with tested models of service delivery in place who are deafblind. Educational and child psychology,
to ensure that no child at-risk is left out. There Vol. 21, No. 2, pp. 67. Available at http://
is a strong need for a conducive environment alice.nc.huji.ac.il/~dmitry/Reading/Data/Lesions/
where every at-risk child in need for EI services interesno.pdf. Visited on 07 February 2016.
gets access to quality services on time. The ap- O'KEEFE, P. (2009): People with disabilities in India: from
plication of the SII-EI model and insights re- commitments to outcomes. Washington, DC: World
lated to its implementation in India may serve Bank. Available at http://documents.worldbank.org/
as useful information for other organisations in curated/en/2009/07/11027298/people-disabilities-
developing EI models for children with india-commitments-outcomes. Visited on 07 February
deafblindness in other parts of the world. 2016.
PRS LEGISLATIVE RESEARCH (2015): Legislative Brief- The
Acknowledgements Rights of Persons with Disabilities Bill, 2014. New
The authors are grateful to Sense International Delhi. Available at http://www.prsindia.org/uploads/
(UK) for their support and guidance to Sense media/Person%20with%20Disabilities/Legisla-
International (India) in developing the model of tive%20Brief%20%20-%20Disabilities%202014.pdf.
EI for the deafblind population in India. The Visited on 07 February 2016.
authors would also like to acknowledge the SENSE INTERNATIONAL (INDIA) (2015): Annual Report.
support received from Sense India training Ahmedabad. Available at http://
team – Deepak Krishna Sharma, Srinivasan www.senseintindia.org/resources/annual-report. Vis-
Prasannan, Brahada Shanker, and Rashmikant ited on 07 February 2016.
Mishra. SENSE INTERNATIONAL (INDIA) (n.d.): What is deafblind-
ness. Available at http://www.senseintindia.org/
References about/deafblindness. Visited on 07 February 2016.
BARNES, C./MERCER, G. (2003): Disability: key concepts. SOURCE (n.d.): Deafblindness. Available at http://
Cambridge: Polity. www.asksource.info/topics/health-and-functional-re-
CENSUS OF INDIA (2011): Data on disability. Office of habilitation/deafblindness. Visited on 07 February
the Registrar General and Census Commissioner, In- 2016.
dia. SOUTHERN, N./DRESCHER, L. (2005): Technology and
CHEN, D./HANEY, M. (1995): An early intervention model the needs of deafblind people. International Congress
for infants who are deafblind. Journal of Visual Im- Series, Vol. 1282, pp. 997–1001. Available at http://
pairment and Blindness, Vol. 89, pp. 213-221. doi.org/10.1016/j.ics.2005.05.057. Visited on 07
DAMMEYER, J. (2014): Deafblindness: A review of the lit- February 2016.
erature. Scandinavian Journal of Public Health, Vol. UNICEF/UIS (2014): South Asia Regional Study. Covering
42, No. 7, pp. 554–562. Available at http://doi.org/ Bangladesh, India, Pakistan and Sri Lanka. Available
10.1177/1403494814544399. Visited on 07 Febru- at http://www.uis.unesco.org/Library/Documents/out-
ary 2016. of-school-children-south-asia-study-2014-en.pdf. Vis-
DANERMARK, B. D./MOLLER, K. (2008): Deafblindness, ited on 07 February 2016.
10 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentARTIKEL/ARTICLE
Zusammenfassung: Es gibt nur wenig Forschung zu Früh- Authors: Akhil S. Paul is the Director and Founder
förderprogrammen (EI) bei sensorischen Beeinträchtigun- member of Sense International India. He is the For-
gen in Indien und global. Sense International India (SII) hat mer Vice President of Deafblind International (DBI), a
2012 als nationale Organisation ein Model zur Frühförde- world association promoting services for deafblind
rung speziell für Menschen mit Taubblindheit entwickelt. people. He is also the Founder Member of the Board
Dieser Beitrag verwendet das SII-EI Model als Fallstudie, of the National Trust for Welfare of People with
um Barrieren und Förderfaktoren in der Bereitstellung von Autism, Cerebral Palsy, Mental Retardation and Multi-
Frühförderung für Kinder mit Taubblindheit in Indien aufzu- ple disabilities.
zeigen. Biju Mathew is the Associate Director of Sense Inter-
national India. He is a post graduate in Social Work
Résumé: La recherche sur les programmes d'intervention with more than 15 years of experience of working in
précoce répondant aux déficiences sensorielle est très limi- the field of deafblindness rehabilitation field.
tée en Inde et au niveau mondial. En tant qu'organisation Uttam Kumar is the Head of Programme Development
nationale, Sense International India (SII) a élaboré, en at Sense International India. He is a post graduate in
2012, un modèle de services IP spécifiquement prévues Psychology and has more than 12 years of experience
pour les personnes avec surdicécité. Ce document utilise le in the field of deafblindness rehabilitation.
modèle SII-IP comme une étude de cas pour mettre en évi- Sachin Rizal heads the training and research team at
dence les obstacles et les facilitateurs dans la fourniture de Sense International India. He holds a Diploma in Spe-
services IP pour les enfants avec surdicécité en Inde. cial education in Deafblindness along with his Master
in Social work and is working in field of deafblindness
Resumen: La investigación sobre los programas de inter- rehabilitation since 2007.
vención temprana (IT) con respecto a la discapacidad sen- Atul Jaiswal is a PhD scholar at Queens University,
sorial es muy limitada en la India, como a nivel mundial. Canada. He has worked for Sense International India
Sense Internacional India (SII), que es una organización a as Senior Programmes Officer for two years. His cur-
nivel nacional, desarrolló en 2012 un modelo de servicios rent doctoral research focuses on community based
de IT especificados para las personas con sordoceguera. rehabilitation services for people with deafblindness in
Este artículo utiliza el modelo de SII-IT como un estudio de India.
caso para poner en relieve las barreras y facilitadores en la Contact: Akhil Paul, Biju Mathew, Uttam Kumar and
prestación de servicios de intervención temprana para los Sachin Rizal: info@senseintindia.org
niños con sordoceguera en la India.
Behinderung und internationale Entwicklung 1/2016 11
Disability and International DevelopmentARTIKEL/ARTICLE
Women, Motherhood, Children and Disabled Persons –
Mainstreaming Disability in Development in Pakistan
Kozue Nagata
Women with disabilities in Pakistan do suffer from double or triple discrimination. Disability and gender is a
closely interrelated developmental issue. This paper aims at analysing highlights covering gender, mother-
hood and disability in Pakistan, based on available statistics and studies, and the voices of disabled Pakistani
women. The study gives insight into some causes and consequences of disability and development from the
gender perspective.
Introduction
in a series of focus groups and the author’s in-
Everywhere all over the world, women and girls formed observations during her three and a
are discriminated because they are women, half year official function in Pakistan. It looks
and more so in some countries. Having a dis- into some causes and consequences of disabil-
ability compounds this gender-based prejudice. ity and development (disability dynamics) from
Women with disabilities in Pakistan do suffer the gender perspective.
from this double discrimination. Disability and
gender is a closely interrelated developmental Disability Statistics
issue, as both disability and gender inequality
are a cause and a consequence of underdevel- In Pakistan, there are no updated statistics on
opment. Disabled women are often poor, thus, women and girls with disabilities. Disability has
poverty adds a new dimension to this double been included in the National Census. Accord-
discrimination. In Pakistan, the issue of disabil- ing to the National Population Census of the
ity has been neglected and ignored from all as- year 1998, 2.49 percent (3,286,630) of the to-
pects of development, which includes adminis- tal population in Pakistan lived with some kind
trative, financial and legal development. of disability. This is far less than the World
Women with disabilities are the most marginal- Health Organisation’s estimate of seven to ten
ised because they are not represented in the percent for developing countries and the world
country. They are invisible, hidden, and their average. It is most likely an underestimation.
voices are not heard. According to the highly medical model classi-
So far, there is no serious effort by the Gov- fication system of disability statistics in Pakistan,
ernment to conduct a comprehensive national the breakdown of disability was: 8.06 percent
survey to assess the socio-economic character- were blind, 7.43 percent deaf/mute, 18.93 per-
istics and problems of persons with disabilities. cent physically disabled defined as ‘crippled’ in
In the absence of national data, it is difficult to the National Population Census, 6.39 percent
estimate accurately the scale and magnitude of mentally ill defined as insane, 7.60 percent
problems being faced by women and girls with mentally challenged defined as mentally re-
disabilities. Thus, this paper aims at analysing a tarded, 8.23 percent having multiple disabilities
couple of highlights covering gender and dis- and 43.37 percent others1.
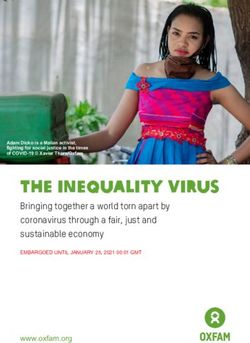
ability in Pakistan, based on available statistics The number of males (58%) with disabilities
and studies, the real voices of disabled women is significantly greater than females (42%). Sci-
Table 1: Population with disabilities by sex, nature of disability*
Sex Total Blind Deaf and Crippled Insane Mentally Multiple Others
mute retarded
Both sexes 3.286.630 264.762 244.254 622.025 210.129 249.823 270.381 1.425.256
Male 1.915.102 145.656 139.168 379.989 119.139 134.489 140.393 856.268
Female 1.371.528 119.106 105.086 242.036 90.990 115.334 129.988 568.988
Male 58,0 % 55,0 % 57,0 % 61,0 % 57,0 % 54,0 % 52,0 % 60,0 %
Female 42,0 % 45,0 % 43,0 % 39,0 % 43,0 % 46,0 % 48,0 % 40,0 %
Source: Population Census 1998, Government of Pakistan
* Terminology used in the national statistics are considered "not appropriate"; however, for absolute accuracy purpose,
the original terms are kept in this quoted table.
12 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentARTIKEL/ARTICLE
entifically and biologically speaking, similar to unit which is named UN Convention on the
the pattern of general population distribution, Rights of Persons with Disabilities (UNCRPD)
the men-women ratio of disability incidences Secretariat for the Implementation of the Con-
shall be close to one to one. This gender gap is vention. In addition, a Core Committee was
possibly because of disabled women being formulated to monitor/coordinate with the Fed-
non-visible and uncounted due to social shame, eral Ministries, Departments, and Provincial
and also possibly a higher incidence of selected Government Departments as well as NGOs/
female infanticides (of disabled girls) caused by DPOs for the implementation of the Conven-
discrimination. This represents deep-rooted tion5. But after the Devolution, these institu-
gender insensitivity within households. The tional mechanisms were naturally dissolved.
above-mentioned gender imbalance of disabil- Concerning childhood disability, Pakistan is also
ity may be caused also by higher mortality a signatory of the United Nations Convention
among disabled girls, due to social discrimina- on the Rights of the Child (CRC). Dating back to
tion, namely, preference for male children or 12th of November 1990, Pakistan ratified CRC
non-disabled girls within the same households. that recognises fully the rights of children with
Often, more resources are used in rearing a disabilities in its articles 2 and 236. These arti-
disabled boy than a disabled girl. A disabled cles shall apply to all children including girls.
girl child may receive less nutrition, less atten- A National Plan of Action (NPA) exists since
tion and mediocre health care, and thus die 2006 to implement the country’s National Pol-
young2. In either way, the statistics indicate that icy for Persons with Disabilities of 2002. The
disabled women are invisible and hidden sis- NPA identified 17 key areas of intervention,
ters. It is a total denial of the very existence of based on a comprehensive assessment of the
women with disabilities. problems in service delivery systems. Out of the
From the total disabled population, total 17 areas of key action, two goals were
2,173,999 (66 percent) were in rural areas and about children with disabilities. The first goal is
1,112,631 (34 percent) in urban areas. As gen- to strengthen special education for children
eral population distribution of Pakistan in 2014 with severe or multiple disabilities, those who
indicates that 62 percent live in rural areas, this often face difficulties in integrated or inclusive
is more or less similar to the national trend, but educational system. However, only less than
with slightly higher incidence in rural areas. one to two percent of children with disabilities
Concerning the provinces, the highest number have access to the existing special education
of persons with disabilities was reported in Pun- centres. Rural children have almost no access to
jab (1,826,623), followed by Sindh (929,400), them – it is just a dream for them and their
Khyber Pakhtunkhwa (375,448) and Baluchis- mothers. Another goal is to promote inclusive
tan (146,421) (Government of Pakistan 1998)3, education. However, as of today, most of the
following the general population distribution regular schools in Pakistan are not geared to
pattern in the country. accommodate children with special needs, ex-
cept a dozen of so-called pilot schools located
Institutional Framework in urban areas such as Islamabad or Punjab
Province.
International Human Rights Ratifications
On 12 March 1996, Pakistan ratified the Con- The Institutional Mechanisms
vention on the Elimination of all Forms of Dis- In result of the 18th Constitutional Amendment
crimination against Women (CEDAW). On 25 (Devolution) in 2010, the Federal Ministry of
October 1994, Pakistan ratified the ILO Voca- Social Welfare and Special Education was de-
tional Rehabilitation and Employment (Disabled volved, which had been responsible for coordi-
Persons) Convention of 1983 (No 159). How- nation with the concerned bodies and depart-
ever, there is little effort for enabling disabled ments in Pakistan for welfare, education, train-
persons to secure, retain and advance in decent ing and rehabilitation. After the 18th Amend-
employment. In August 2011, Pakistan ratified ment, the matters concerning disability have
the UN Convention on the Rights of Persons been devolved and transferred to local govern-
with Disabilities (UN CRPD) which recognises ments of the Federal State of Pakistan, namely
priority concerns of disabled people, including four provincial governments7; therefore, now
particular problems and rights of women and there is an urgent need to look into provincial
children with disability in Articles six and seven projects, programmes and plans of action
respectively4. In 2012, prior to the Devolution, mainly by provincial entities, together with dis-
the Directorate General Special Education and abled people.
Social Welfare (DGSE&SW) established a small Concerning the implementation of the UN
Behinderung und internationale Entwicklung 1/2016 13
Disability and International DevelopmentARTIKEL/ARTICLE
CRPD (human rights issue), the responsibilities issue in many communities and across the so-
have been transferred on paper to the Federal cial classes of Pakistan. Iron tablets, Vitamin A
Ministry of Human Rights, but its capacity and supplement and iodised salt are to be out-
funding is rather limited. About the status of reached. Poverty alleviation must be managed
women in general, the National Commission as a part of overall national development strat-
on the Status of Women is fully responsible for egy, and also to reduce disability incidences.
monitoring the rights of Pakistani women, as
well as mainstreaming the concerns and needs Insufficient Immunisation
of women with disabilities. After the Devolu- Some vaccination campaigns also face a seri-
tion, there has been great confusion and chaos ous challenge, particularly those related to po-
in the responsibilities and coordination between lio. For instance, polio virus can cause complete
provincial governments and the Federal Gov- or partial paralysis of infected children. The
ernment. Civil society is very active in Pakistan. world-wide polio rate has declined but today
There are a number of civil society organisa- the virus is active only in three countries of the
tions that have been working to promote the World, Afghanistan, Nigeria and Pakistan. Paki-
wellbeing of persons with disabilities (including stan counted about 85% of world polio infec-
disabled women) but their efforts are not well tions in 201412. Some religious and terrorists
coordinated and scattered. Some of these groups such as Pakistan Taliban (TTP) reject po-
NGOs are run by persons with disabilities; thus lio campaigns as a Western plot to sterilise, and
they are eligible as Disabled People’s Organi- a number of polio workers and mothers have
sations. As of today, however, there is no inde- been shot by them. In villages, many mothers
pendent and third party national monitoring refuse to have their children vaccinated be-
mechanism about the implementation of UN cause of fear and threats, in addition to their
CRPD. misunderstanding of religious grounds. Some
UN agencies such as WHO and UNICEF, to-
Causes of Impairment and Disability gether with provincial governments, are work-
ing hard, utilising female health workers, to
Disability prevention at the social, medical and eradiate polio in high risk areas such as the
policy levels have been identified as a priority North Waziristan area.
in every meeting and encounter that the author
has had with officials and PWDs in Pakistan be- Violence against Women Including
tween 2011 and 2014. Governments and civil Acid Attacks
society organisations in all provinces are deal- Violence against women in general is a cause
ing with the most direct causes of disability and of mortality and morbidity, including various
have been devising comprehensive policies to permanent physical damages, disfigurement
tackle them. One of the main tools in preven- and psychological traumas. Studies done by
tion is public awareness raising and mass me- several organisations indicate that an increase
dia public campaigns. in violence against women has been noted re-
cently. Honor killing, domestic violence, rape
Poverty and Malnutrition and gang rape, and forced marriages area
In poor rural and urban communities, poverty, among some of the violence against and viola-
insufficient level of pre-, neo- and post-natal tions of human rights of women and girls in
care, and the high illiteracy rate among moth- Pakistan. Among the victims, Malala Yousafzai
ers8, all contribute to the increase in impair- is a famous Pakistani girl and Nobel Prize win-
ment and exacerbate the conditions of disability ner who stood up for education of girls and was
among newborns/infants, children and young shot by the Pakistan Taliban. She has recovered
women. Harmful child marriage practice9 in well from the bullet injury and inspired many
some conservative villages is another cause of people of the world by sharing her terrifying ex-
impairment. Measures are being taken to in- periences and showing her courage. However,
crease the legal age for marriage and to pro- in the country, there are many more Malala-
vide mothers with health and nutrition knowl- girls, some of whom just died, or became per-
edge and training, particularly in rural areas manently disabled and continued to be op-
and poor urban slum communities. Having too pressed. There is also common and socially ac-
many children without proper spacing is also a cepted domestic violence (DV), in which hus-
gender-specific social issue as pregnant moth- bands may beat, kick, permanently disfigure, or
ers might be over a critical age by the time they disable their wives whenever they feel upset.
give birth to their last child10. Malnutrition in- Acid attack is worth being mentioned. Paki-
cluding the lack of micro-nutrients11 is still an stani women are also afraid of acid attacks,
14 Behinderung und internationale Entwicklung 1/2016
Disability and International DevelopmentYou can also read