Breast Feeding and Food Allergy - 4/20/2021 Summer E. Monforte MD, FAAAAI Pediatric Allergy, Asthma and Immunology Montana Children's Specialists ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Breast Feeding and Food Allergy 4/20/2021 Summer E. Monforte MD, FAAAAI Pediatric Allergy, Asthma and Immunology Montana Children’s Specialists

Disclosures None

Objectives (UPDATED) 1. Learn about the different types of food reactions and how to use the correct terminology regarding these reactions. 2. Gain familiarity with the most common types of food allergic reactions, how and when they present, and their natural histories. 3. Understand the risk factors associated with development of IgE mediated food allergy. 4. Gain familiarity with the current state of the evidence regarding breast feeding and the development of allergic disease and food allergy specifically.

First, What is Food Allergy?
Definitions- Allergy The term "food allergy" refers to an abnormal immunologic reaction to a food that results in the development of symptoms on exposure to that food [1].
Definitions- Sensitization The term "sensitization" is used to denote the presence of IgE directed against a specific antigen (a "positive" test). However, a patient who is sensitized to a food frequently may not be clinically reactive with actual exposure to the food [1].

Definitions- Intolerance The term “food intolerance” is a non-specific description of unpleasant symptoms associated with ingestion of a specific food which are not associated with an immunologic mechanism. These reactions cannot be proven or ruled out by allergy testing.

Types of Food Allergy

Type I Hypersensitivity
An IgE mediated reaction to a food where ingestion of a food rapidly
(generally within 1 hour) triggers symptoms that can progress to anaphylaxis
through abnormal activation of mast cells and basophils primarily.
Symptoms include:
Hives
Angioedema
Difficulty breathing
Decreased blood pressure
Repetitive Vomiting
LethargyAdditional Immunologically Mediated Food Reactions Milk Protein Induced Prococolitis FPIES (Food Protein-Induced Enterocolitis Sydrome) Eosinophilic Esophagitis
How Common is Food Allergy? It depends on how we measure it.
Prevalence- Parental Report The prevalence of parentally reported food allergy in children (aged 0 to 17 years) in the United States increased from 3.4 percent in 1997 to 1999, to 5.1 percent in 2009 to 2011 [2], and 6.2 percent in 2016 [3] according to the National Health Interview Survey. Parentally reported adverse food reactions in Norway were assessed by collecting questionnaires at six-month intervals. The cumulative incidence of adverse food reactions was 35 percent by age two years. [4,5,6]
Prevalence- Sensitization A German Multicenter Allergy Study followed the development of sensitization to common food allergens. Reactions to hen's egg and cow's milk were most common, with peak prevalence rates of approximately 6 percent at age one year, followed by wheat and soy.[7,8,9] A Danish study showed similar results, with approximately 6 percent sensitized to milk and/or egg at 1.5 years, rising to approximately 14 percent at 5 years.[10,11] In an Australian birth cohort, the prevalence of sensitization to peanut, egg, and sesame during the first year of life was 8.9, 16.5, and 2.5 percent. [12] In a European birth cohort, the prevalence of cow's milk sensitization during the first two years of life was 2.9 percent. [13]
Prevalence- Challenge Proven
In the same Australian cohort, prevalence of challenge-proven allergy to
these same foods was 3.0 (PN), 8.9(egg), and 0.8 percent sesame. [12]
In the European cohort, challenge-proven allergy to milk was 0.5 percent.
[13]
Just based on these 2 studies you can see that sensitization can be 3-5 times
more common than challenge confirmed allergy, and some studies actually
show that somewhere between 50-90% of positive skin tests are false positives,
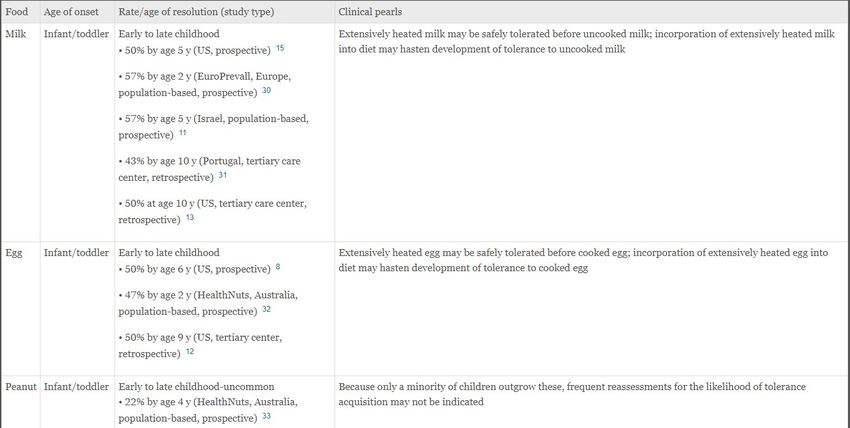
especially when the history is not consistent with an IgE mediated reaction. [14]Natural History The majority of IgE mediated food allergy presents in infancy or toddlerhood. [16] The age of resolution of food allergy can depend on the problem food with foods like milk and egg being commonly outgrown in the first 2 years of life, and foods like peanut and tree nut resolving more commonly in later childhood. [16]
Table I, Common allergenic foods with general age of onset of clinical allergy and resolution. Savage J, Sicherer S, Wood R. The Natural History of Food Allergy. J Allergy Clin Immunol Pract. 2016 Mar-Apr;4(2):196-203
Risk Factors for the Development of Food Allergy
Immutable Factors Causing Increased Risk [17] Sex (male sex in children) Race/ethnicity (increased among Asian and black children compared with white children) Genetics (familial associations, HLA, and specific genes)
Potentially Modifiable Risk Factors [17] Poorly controlled eczema Delayed oral introduction allowing for sensitization through the skin
Potentially Modifiable Risk Factors [17] Vitamin D insufficiency Inadequate consumption of omega-3-polyunsaturated fatty acids Inadequate consumption of antioxidants
Potentially Modifiable Risk Factors [17] Microbiome factors Use of antacids (reducing digestion of allergens) Obesity (being an inflammatory state)
What about breast feeding?
Is breastfeeding protective against food allergy? The short answer is that we are not sure. In general, breast feeding is thought to protect against allergic disease, but the evidence is not strong and is inconsistent.
Güngör et al: Infant milk-feeding practices and food allergies,
allergic rhinitis, atopic dermatitis, and asthma throughout the life span:
a systematic review. [19]
1) never, versus ever, being fed human milk is associated with higher risk of
childhood asthma (level of evidence moderate, mostly observational data)
2) among children and adolescents who were fed human milk as infants, shorter
durations of any human milk feeding are associated with higher risk of asthma.
(level of evidence moderate, mostly observational data)
However, only very limited evidence was available regarding the association
between ever being fed human milk and atopic dermatitis in childhood or the
duration of any human milk feeding and allergic rhinitis and atopic dermatitis in
childhood. The evidence that was available did not suggest an association.Halken et al: Prevention of allergic disease in childhood: clinical and epidemiological aspects of primary and secondary allergy prevention. [20] In a prospective cohort intervention study, it was found that infants who were exclusively breast fed for at least 4 months had a significantly reduced cumulative prevalence of cow’s milk allergy [3.6% (5/141) vs. 20%(15/75) in the control group] up to 5 yr. However, the exclusively breastfed infants were significantly less exposed to tobacco smoke and pets, had solid foods introduced later and belonged to higher social classes.
Matheson et al: Understanding the evidence for and against the role of breastfeeding in allergy prevention. [18] Current evidence is inconclusive regarding the effect of breastfeeding on the development of eczema, with the most recent systemic review reporting no protective effect. There is insufficient data regarding the effects of breastfeeding on objective measures of food allergy at any age. Studies show a paradoxical effect of breastfeeding on the prevention of asthma, with an apparent protective effect against early wheezing illness in the first years of life yet an increased risk of asthma in later life.
The Difficulties With the Evidence
There are huge variations in the study designs and definitions of disease. Also, many of the
confounding factors (especially household and other environmental factors) are incredibly
different to control for. [18]
Since randomized control trials in breast feeding research would be considered unethical,
the evidence remains limited to poorer quality observational studies where participation
and recall bias can severely affect the objectivity of the data collected. [18]
Some of the discrepancy among studies may be explained by differences in human milk
composition, which has not been accounted for in the broad definition of breastfeeding.
[21]
Gene-environment interaction have also been shown to affect protection. The association
between breastfeeding and food sensitization can change depending on the genotypes
of certain components of the immune system.
For example, breastfeeding increases the risk of food sensitization in children carrying the GG
genotype but decreases the risk in children carrying the GT/TT genotype of the IL-12 receptor
β1. [22]In my opinion…….. Breastfeeding should be encouraged for all infants due to its many health benefits. However, at this point the evidence is not strong enough to recommend breastfeeding specifically to decrease the risk of allergic disease.
IF breastfeeding were found to protect against allergic disease, what would the mechanism be?
What does human milk contain? [21] Macronutrient components Human milk oligosaccharides (HMOs) Immune cells Cytokines and chemokines Hormones Immunoglobulins Growth factors Active enzymes (including peroxidases and lysozymes) lactoferrin and additional secretory components Soluble CD14, TLR2, and tumor necrosis factor (TNF) Maternal diet-derived food antigens Its own microbiome made up of bacteria and viruses.
The Microbiome
In addition to prenatal environment, delivery mode, antibiotic treatment,
and diet, the infant microbiome composition is significantly influenced by
breastfeeding. [21]
The dominant microbes of breastfed infants (bifidobacteria , lactobacilli,
Enterobacteriaceae) are surpassed by Clostridium and Bacteroides species
after cessation of breast feeding.
Kourosh et al found that children with IgE mediated food allergy had
significantly different Clostridia species than control children. [23]Immune Components The immune cells, chemokines, cytokines and immunoglobulins present in milk interact with the immune cells lining the child’s GI tract and can help push inflammatory pathways in one direction or another to help protect against infection. It is possible that these same factors can help push the immune system towards tolerance instead of sensitization when it comes to food proteins. (there are mouse models that suggest this is true).[21]
Can food allergens in human milk cause food allergy? There is a lot of debate on this topic. Food proteins commonly associated with food allergy (ovalbumin, beta- lactoglobulin, gliadin, Ara h 2) are found in measurable concentrations of human milk after maternal ingestion. [21] Food allergen proteins present in human milk can induce allergic symptoms in sensitized infants, but certainly do not always. Most studies on this topic are small, and difficult to control. Results are mixed, some showing no association with food allergy, some showing a protective effect of food allergens in the maternal diet, and some showing increased risk. [21]
In my opinion…..
There is insufficient evidence to suggest that avoidance or purposeful
inclusion of allergenic foods in the maternal diet will have an impact on
development of food allergy in the infant………..
BUT, it makes no sense to me that breast feeding would not help. Allergy is due
to a poorly trained immune system, and breast feeding ABSOLUTELY helps train
an infant’s immune system.
I encourage well rounded, healthy diets in pregnant and lactating mothers
and they may include any and all common food allergens based on their
own preferences.What are signs of a food allergy in a
lactating infant?- Proctocolitis
Allergic proctocolitis is the type of food allergy has the potential to present
earliest in life.
Infants in their first 4 weeks of life can develop bloody stools after ingestion of a
specific food. The most common foods causing this presentation are milk and
soy.
This type of food allergy is almost always outgrown by the first year of life.
Allergy skin prick testing is not helpful to identify the culprit.What are signs of a food allergy in a
lactating infant?- FPIES
Another type of food allergy that can present while children are still breast-
feeding is FPIES, however this is much more likely to present once the child is
eating solid foods.
Symptoms of FPIES are delayed usually several hours after ingestion and consist
of profound vomiting and/or diarrhea that can lead to dehydration and shock.
The most common triggers of FPIES are milk, soy, rice, and chicken.
This type of allergy is almost always outgrown by age 2 or 3 years old.
Allergy skin prick testing is not helpful to identify the causative food.What are signs of a food allergy in a lactating infant?- Eosinophilic esophagitis Eosinophilic esophagitis (EoE) is a condition where allergic white blood cells invade the esophagus and cause thickening and inflammation. Primary symptoms include difficulty swallowing, food avoidance, and texture avoidance. Other symptoms that could present earlier are poor weight gain and vomiting, however EoE does not commonly present in infancy.
What are signs of a food allergy in a
lactating infant?- IgE mediated
IgE mediated food allergy can also present in very young infants but more
commonly present with introduction of solid foods.
Symptoms include hives, lip swelling, tongue swelling, facial swelling,
difficulty breathing, pallor, lethargy.
The most common food triggers are milk, egg, wheat, soy, peanut, tree
nuts, fish and shellfish.
Many children will outgrow this type of food allergy, but when they outgrow
it is quite variable.
Allergy testing is helpful to identify culprit foods.In Summary: Food allergy is becoming more common, but there are far more cases of reported food allergy than cases of allergy that are appropriated confirmed. There are many different factors that go into determining if a child is at higher risk for food allergy. Some can potentially be modified and others cannot. Breastfeeding has not been proven to reduce the risk of food allergy, but is extremely unlikely to increase the risk. Immunomodulatory effects of human milk could lead to overall decreased risk of atopy through helping establish a healthy gut microbiome and providing healthy stimulation to the infant’s developing immune system. It is possible for babies to have allergic reactions to food proteins in their mother’s milk but is very uncommon. There is insufficient evidence to recommend empiric limitation of the mother’s diet.
Questions?
References
1. Food allergy in children: Prevalence, natural history, and monitoring for resolution, Up To Date, Authors: Corinne Keet, MD, PhD, Robert A Wood, MD,
Section Editor: Scott H Sicherer, MD, FAAAAI Deputy Editor: Elizabeth TePas, MD, MS.Literature review current through: Mar 2021.
2. Trends in Allergic Conditions Among Children: United States, 1997–2011. http://www.cdc.gov/nchs/data/databriefs/db121.pdf (Accessed on June 20,
2013).
3. Age-adjusted percentages (with standard errors) of hay fever, respiratory allergies, food allergies, and skin allergies in the past 12 months for children
under age 18 years, by selected characteristics: United States, 2016. National Health Interview Survey, 2016.
https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2016_SHS_Table_C-2.pdf (Accessed on June 04, 2018).
4. Prevalence of parentally perceived adverse reactions to food in young children. EggesbøM, Halvorsen R, Tambs K, Botten G Pediatr Allergy
Immunol. 1999;10(2):122.
5. The prevalence of CMA/CMPI in young children: the validity of parentally perceived reactions in a population-based study. EggesbøM, Botten G,
Halvorsen R, Magnus P Allergy. 2001;56(5):393.
6. The prevalence of allergy to egg: a population-based study in young children. EggesbøM, Botten G, Halvorsen R, Magnus P Allergy. 2001;56(5):403.
7. Sensitization to hen's egg at the age of twelve months is predictive for allergic sensitization to common indoor and outdoor allergens at the age of
three years. Nickel R, Kulig M, Forster J, Bergmann R, Bauer CP, Lau S, Guggenmoos-Holzmann I, Wahn U J Allergy Clin Immunol. 1997;99(5):613.
8. Prediction of sensitization to inhalant allergens in childhood: evaluating family history, atopic dermatitis and sensitization to food allergens. The MAS
Study Group. Multicentre Allergy Study. Kulig M, Bergmann R, Niggemann B, Burow G, Wahn U Clin Exp Allergy. 1998;28(11):1397.
9. Natural course of sensitization to food and inhalant allergens during the first 6 years of life. Kulig M, Bergmann R, Klettke U, Wahn V, Tacke U, Wahn U
J Allergy Clin Immunol. 1999;103(6):1173.
10. The natural course of sensitization and allergic diseases from childhood to adulthood. Nissen SP, Kjaer HF, Høst A, Nielsen J, Halken S Pediatr Allergy
Immunol. 2013;24(6):549. Epub 2013 Jul 31.
11. Prevalence and longitudinal trends of food allergy during childhood and adolescence: Results of the Isle of Wight Birth Cohort study.
Venkataraman D, Erlewyn-Lajeunesse M, Kurukulaaratchy RJ, Potter S, Roberts G, Matthews S, Arshad SH Clin Exp Allergy. 2018;48(4):394. Epub 2018
Feb 8.References
12. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants.
Osborne NJ, Koplin JJ, Martin PE, Gurrin LC, Lowe AJ, Matheson MC, Ponsonby AL, Wake M, Tang ML, Dharmage SC, Allen KJ, HealthNuts Investigators
J Allergy Clin Immunol. 2011;127(3):668.
13. Schoemaker AA, Sprikkelman AB, Grimshaw KE, et al. Incidence and natural history of challenge-proven cow's milk allergy in European children--
EuroPrevall birth cohort. Allergy 2015; 70:963.
14. Willits EK, Park MA, Hartz MF, et al. Food Allergy: A Comprehensive Population-Based Cohort Study. Mayo Clin Proc 2018; 93:1423.
15. American College of Allergy, Asthma, & Immunology. Food allergy: a practice parameter. Ann Allergy Asthma Immunol 2006; 96:S1.
16. The Natural History of Food Allergy Jessica Savage MD, MHS, Scott Sicherer MD and Robert Wood MD Journal of Allergy and Clinical Immunology:
In Practice, 2016-03-01, Volume 4, Issue 2, Pages 196-203.https://pubmed.ncbi.nlm.nih.gov/26968958/
17. Scott H. Sicherer, Hugh A. Sampson, Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management,
Journal of Allergy and Clinical Immunology, Volume 141, Issue 1, 2018, Pages 41-58, ISSN 0091-6749,
18 Matheson MC, Allen KJ, Tang ML. Understanding the evidence for and against the role of breastfeeding in allergy prevention. Clin Exp Allergy. 2012
Jun;42(6):827-51. doi: 10.1111/j.1365-2222.2011.03925.x. PMID: 22276526.
19. Güngör D, Nadaud P, LaPergola CC, Dreibelbis C, Wong YP, Terry N, Abrams SA, Beker L, Jacobovits T, Järvinen KM, Nommsen-Rivers LA, O'Brien KO,
Oken E, Pérez-Escamilla R, Ziegler EE, Spahn JM. Infant milk-feeding practices and food allergies, allergic rhinitis, atopic dermatitis, and asthma
throughout the life span: a systematic review. Am J Clin Nutr. 2019 Mar 1;109(Suppl_7):772S-799S. doi: 10.1093/ajcn/nqy283. Erratum in: Am J Clin Nutr.
2019 Oct 1;110(4):1041. PMID: 30982870; PMCID: PMC6500928.
20. Halken S. Prevention of allergic disease in childhood: clinical and epidemiological aspects of primary and secondary allergy prevention. Pediatr
Allergy Immunol. 2004 Jun;15 Suppl 16:4-5, 9-32. doi: 10.1111/j.1399-3038.2004.0148b.x. PMID: 15125698.
21. Järvinen KM, Martin H, Oyoshi MK. Immunomodulatory effects of breast milk on food allergy. Ann Allergy Asthma Immunol. 2019 Aug;123(2):133-143.
doi: 10.1016/j.anai.2019.04.022. Epub 2019 Apr 29. PMID: 31048004; PMCID: PMC6693634.
22. Hong X., Wang G., Liu X., et. al.: Gene polymorphisms, breast-feeding, and development of food sensitization in early childhood. J Allergy Clin
Immunol 2011; 128: pp. 374-381 e372.
23. Kourosh A., Luna R.A., Balderas M., et. al.: Fecal microbiome signatures are different in food-allergic children compared to siblings and healthy
children. Pediatr Allergy Immunol 2018; 29: pp. 545-554.Contact
You can also read