Building a future in which children survive and thrive - Linda M Richter DST-NRF Centre of Excellence in Human Development
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Building a future in which
children survive and thrive
Linda M Richter
DST-NRF Centre of Excellence in Human Development
Johannesburg 30 June – 2 July 2014
We are meeting in “the richest square mile
in Africa” – but close to one of the poorest
By way of illustration, how do South African children
survive and thrive?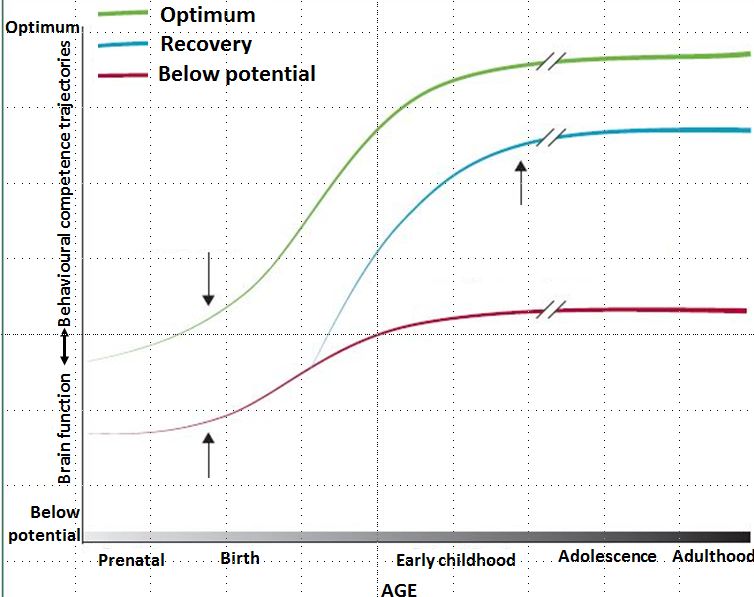
Of 10 children born in SA…
2 in 3 young people are unemployed or in informal work
50% who start
school do not
complete Matric
4 in 10 children fail
at least once in the
first 3y of school
3 in 10 children
What is happening?
• Disparities from
Where most previous
children should
generations are
and can be
evident at birth
Fulfilment
of human • These amplify as a
potential result of variations
in protection and
risks
• Differences “set”
over time
• Leading to poorer
Where too adult health and
many children human capital
end up
• That result in
Conception Birth 3 years 18 disparities at birth in
years the next generation
Age
of childrenSo, what does it mean “to thrive”? To thrive is to develop – to our potential ‒ those capacities that make us human • Vertical strength, mobility and speed • Fine-motor dexterity • Communication and language • Emotional understanding, empathy • Cognitive skills, faculties for maths, logic, etc. • And, MOST IMPORTANT, the ability to identify with and learn from other human beings (which is why the quality of caregiving is so critical)
Children survive and thrive when,
a.o. …
• Pregnancy is wanted, healthy and protected
• Birth is safe
• Women have education and autonomy
• And they have the support of partners and family
• Families have the means to afford necessities
• They are protected from disease and violence
• And they can access health and other services
• Children have opportunities and are encouraged to learn
Both survival and development are under
threat when risks substantially outweigh
protectionProtection needs to outweigh risks
Protection >
risks
Protection increases and
risks decline through early
intervention
Risks >
protectionThe importance of early intervention
Important to intervene early
because …
• Young children’s development is extremely rapid
• Genetic capacities adapt to the foetal and infant
environment
• Development is hierarchical with complex capacities built
on basic abilities
• Emerging brain and other organ systems are vulnerable to
impairment
• Brain plasticity and the ability to change behaviour
decrease over time
• Disadvantages emerge early and differences widen
• We have effective interventions, and
• There is a high cost associated with inactionExtremely rapid development …
E.g., brain development E.g., synaptic development
from conception to birth from birth to 6y
Neurogenesis, neuronal
migration, differentiation,
apoptosis, arborization,
synaptogenesis, synaptic
sculpting, myelinationDisadvantages emerge early, and grow…
1200
Cumulative Vocabulary
Children of College
Educated
1000
Children of
(Words)
800 Lower Middle
Class
Children
600 of Parents
in Poverty
400
200
16 24 36
Source: Hart &
Risley 1995
mos. mos.
Child’s Age (Months) mos.Effective interventions
to promote survival,
growth, health and
developmentWe have effective interventions • Reviewed in, amongst others: – Child survival (Lancet 2003) – Child survival, growth & development (WHO 2004) – Maternal survival (Lancet 2006) – Child development (Lancet 2007, 2011) – Maternal, newborn and child care (Lancet 2007) – Maternal and child nutrition (Lancet 2008, 2013) – Countdown to 2015 (Lancet 2013) – Women deliver (Lancet 2013) – Every newborn (Lancet 2014) • Interventions to promote child survival, health and growth also promote child development – but not usually with intention
We have effective interventions that
promote child development and are/can
be integrated into child survival, growth
and health programmes
Including
• Facility, home and community programmes to:
– Promote child nutrition and development
– Provide opportunities for young children to learn
– Address maternal depression and promote mental
healthInterventions to promote child
wellbeing (growth and development)
• Low & middle income
countries
• 11 RCTs, 2non-RCT trials,
8 program evaluations
• Stimulation programs benefit
children’s development
• Nutrition programs benefit
children’s nutrition
• Combining stimulation and
2014 nutrition is importantOpportunities for children to learn
The Lancet
17 June 2014
• Adapted WHO/UNICEF
Care for Child
Development
• Integrated into the Lady
Health Worker Programme
in Pakistan
• Children in the ‘responsive
stimulation’ condition had
significantly higher motor,
cognitive and language
scores at 2yAddress maternal depression
• Prevalence around 30% in LMICs1
• Maternal depression associated with:
– Threats to maternal and child health (LBW,
substance use, access to services, chronic
conditions)2
– Poor growth among children3, behaviour problems
and delayed development1
• Successfully treated by:
– Social support (Taiwan, Pakistan)
– Group therapy (Uganda)
– Home visits by CHWs (Jamaica)
– Improving mother-infant interaction (South Africa)1,2Early interventions can have long-
term benefits in LMICs ‒ nutrition
The Lancet, 2008, 371
• Children who received a nutrition supplement
before 3y – but not after
• Controlling for a variety of potential family and
socioeconomic confounders
• At age 30y, were earning 46% more than
average wages in the sampleEarly interventions can have long-
term benefits in LMICs ‒ stimulation
Science, 2014, 344
The Lancet, 2008, 371
• Stunted children in Jamaica who received 2-weekly
home visits from CHWs for 2y
• Which taught parents to stimulate and support
children’s cognitive & socio-emotional
development
• 20 years later, had caught up with non-stunted
peers, earning 25% more than the control groupThe high cost of
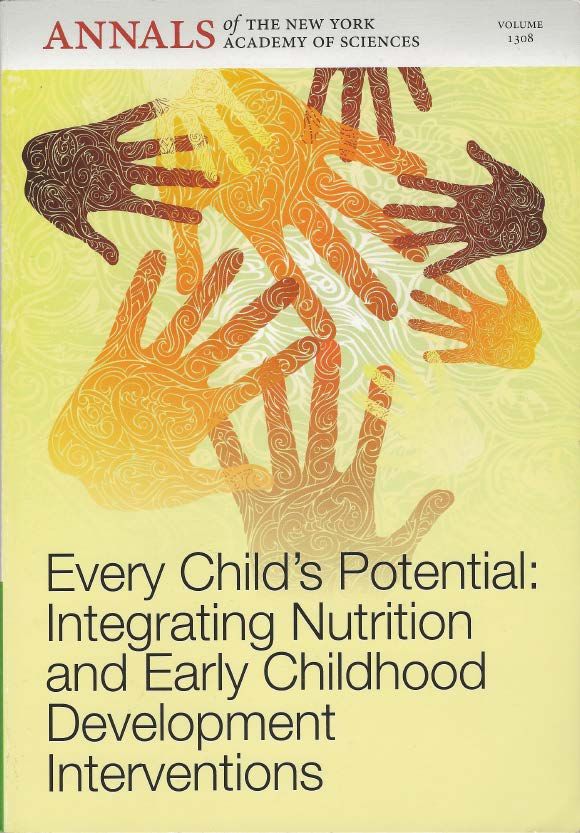
inactionThe high cost of inaction • 200 million children under 5y of age fail to reach their developmental potential • This is 20 times the number of children who die before their 5th birthday and roughly 1/3 of all children of this age in the world • The vast majority of these children live in low and middle income countries • There is a very high cost to our inaction – For individuals and their families – And for the societies in which they live
High costs of poor development for
individual and families
• Scarcity and stress during foetal and infant
development have long-term consequences.
• Many are associated with poverty, and
include:
– Undernutrition, nutritional deficiency
– Exposure to toxins, injury
– Experience of violence, parental ill-health
– Neglect, abuse
– Lack of affection, care and opportunities to learnKnown adverse impacts on long-
term health, wellbeing and human
capital
• Health, including cardiovascular and
metabolic disease1
• Motor, sensory and cognitive disability2
• Poor mental health and social wellbeing3
• Loss of education (up to 1 grade of
schooling)4
• Lower earnings5
• Lower birthweight of offspring6High social costs of poor early
child development
• Without interventions to protect young children,
the burden of morbidity and poor development
rise as infant mortality drops, with severe costs
to individuals and societies (‘mortality selection’)
• Early interventions are critically needed
because countries, especially low and middle
income countries, cannot grow economically
with an increased burden of ill health and poor
capacity in adulthoodSocial costs
• The aggregation of individual costs
• Impact on GDP – The Cost of Hunger Study
• Costs of child undernutrition and knock-on
effects on education, work capacity and
earnings
– Egypt: 20.3 billion Egyptian pounds (EGP), s equivalent to
1.9% of GDP
– Uganda: 1.8 trillion Uganda shilling (UGX), equivalent to
5.6% of GDP
– Ethiopia: Ethiopian birr (ETB) 55.5 billion, equivalent to
16.5% of GDP.Systems thinking for post-2015 • Call by Evan Russel & others in 21 June Lancet • “Current and emerging global health challenges require action that embraces interdisciplinary and intersectoral approaches to development” • We need to move away from vertical interventions • Adopt systems thinking; the perspective and an acknowledgement that the whole is greater than the sum of the parts
Integrated interventions – an example Evidence that social protection cash transfer programmes for poor households can improve: • Child survival (increased vaccination, decreased infectious disease) • Household food security, child nutrition and growth1,2,3 • Child development (Mexico Opportunidades3, South Africa’s Child Support Grant)2
Thank you
You can also read