CHALLENGES AND ISSUES FOR INTERNATIONAL RESEARCH ADDRESSING THE LIFE CONTINUUM FROM MILITARY SERVICE TO TRANSITION - A C MCFARLANE PROFESSOR OF ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Challenges and issues for international
research addressing the life continuum
from military service to transition
A C McFarlane
Professor of Psychiatry
Centre for Traumatic Stress Studies
The University of Adelaide

The Delayed Impact of Military Service Manifests after Transition The issue of time and longitudinal interactions » Cumulative trauma exposures » Multiple deployments » Subsyndromal symptoms » Age Optimal timing and opportunities for early intervention

“Exit Wounds” MAJ GEN John Cantwell
Major General John Cantwell, AO,
Four Corners, ABC, 2010
Yes, we ask an inordinate amount from our people and Australia
needs to understand that. We are placing young men and
women in some of the most dangerous, difficult and life-changing
situations you can imagine.
And those who are wounded, those who are killed, [and] their
families face equal challenges. We cannot underestimate the
damage that we might be doing to our people through constant
stress. We must do everything we can to help them out
psychologically, with medical care, with everything. These
people are putting their lives on the line, they do this without
question. They don’t flinch and when they’re hurt, when they’re
hurting as they will down the years, we’ve got to keep stepping
up as a society and look after them.
Erich Maria Remarque - All Quiet on the Western Front “One thing I do know: everything is sinking into us like a stone now, while we are in the war, will rise up again when the war is over, and that’s when the real life-and- death struggle will start.” (p101)
Erich Maria Remarque: The Road Back
“We look at one another. - What do we want?
yes, if it were so easy a thing to say in a
sentence. A vague, urgent sense of it we
have. - But for words? We have no words for it
yet. But perhaps later we shall have.”
(p 126)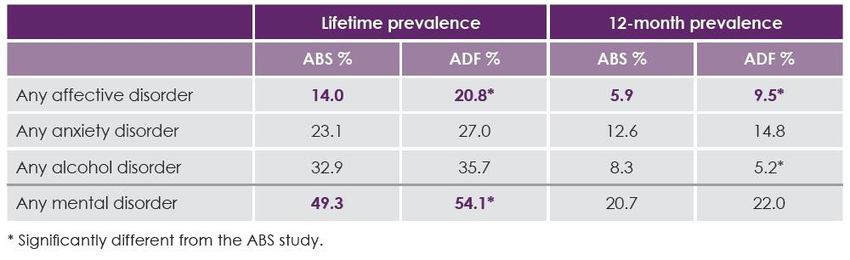
The importance of delayed onset
PTSD and transition
Maximal distress and rates of disorder
are not manifest during military service
– the critical issue of time
Pre, post- deployment and Long- term follow up
2003-2014
Cooperative Studies Program
Vasterling Am J Epi, 2016National Vietnam Veterans
Longitudinal Study
25 year follow up of NVVRS sample
Longitudinal course in combat zone veterans
» 16% report an increase in symptoms
» 7.6% report a decrease
» Era veterans current 10.8% life-time 26.2%
271,000 veterans have current PTSD or
subsyndromal PTSD 40 or more years after
the end of the war
(Marmar et al JAMA Psychiatry, 2015)Millennium Cohort Study: Pre/Post Deployment Samples 3393 with single deployment 4394 with multiple deployment Predeployment and 3 year follow up Latent growth mixture modelling » Banonno et al Brit J Psychiatry 2012
Factors associated with persistent posttraumatic
stress disorder among U.S. military service
members and veterans 2001-2013
older age
deployment with high combat exposure
enlisted rank
initial PTSD severity
Depression
history of physical assault
disabling injury/illness
somatic symptoms.
Armenta et al, 2018 BMC Psychiatry 18:48Post-traumatic stress symptoms 5 years after
military deployment to Afghanistan: an
observational cohort study
1007 Dutch military personnel
First assessed 1 month before and
1month after deployment
5 year follow up
identified an increase in PTSD
symptoms 6 months after deployment
long-term effect increase in symptoms 5
years after deployment
(Eekhout et al Lancet Psychiatry 2016)Latent Trajectories in PTSD
symptomsOther National Studies UK -46% delayed onset cases » subsyndromal symptoms were a significant predictor (Goodwin et al, JNMD, 2012;200:429-437) Canada, nationally representative military sample » related to child trauma, » cumulative trauma exposure and land based troops (Fikretoglu and Liu ,Soc Psychiatry and Pscyh Epi, 2012)
Transition relates to age and
accumulating morbodity
Particular context of duration of Middle
Eastern Area of Operations – period of
particular riskThe Importance of Longitudinal
Neurobiological Research
The identification of biomarkers of risk
and possible mechanisms of disorder
The relationship between mTBI and
PTSD
The need to improve treatment
outcomes
The mechanisms sensitization and
kindlingRepeated hits from multiple
stressors
Sensitization Loss of
reactivity and
increased
physiological response
physiological
load
normal adaptive response
TimeThe challenge of assessing military mental
health and comparing with the civilian
community in the context of transition
How do we assess the stresses and
determinants of transition?Canadian Armed Forces Studies 2002 and 2013 waves of data collection by Stats Canada using CIDI Value of same measures across time Increased prevalence of PTSD, GAD and Panic Disorder Due to burden of Afghanistan and humanitarian deployments, in context of improved health care Increased rates of major depression, GAD, alcohol dependence and suicide attempts compared to the general population
Canadian Armed Forces Studies Demonstrated greater attributed risk of child abuse (29.6%) than Afghanistan deployment (9.6%) to any disorder PTSD 31.5% attributed risk to Afghanistan deployment The healthy worker effect versus provided opportunities for disadvantaged individuals Healthy survivors remain in the military Did not measure the rates of disorder in those who have transitioned
• Regular Force Veterans who released from service during1998- 2007 had worse health, disability and determinants of health status than the general Canadian population.
Civilian Populations
Birth Death
Mental Health
• Risk factors
• Socio-
demographics
• Health
Immigration Emmigration
systemsMilitary Populations
Currently
serving
-Deployments Ex-serving
-Health services and
-Training accidents
-Occupational
veterans
stresses population
New
recruits
Healthy worker effectTransition from military service
Transition from military service reflects a
complex matrix of individual motivations
1. the success or otherwise of military career
2. ongoing health and fitness for military service
3. demands and aspirations of the family unit
4. opportunities within the civilian community
Transition may represent
- failure and disgrace
- quiet mediocrity
- a sense of pride and achievementReasons for transition Medical discharges » Physical » psychiatric Disciplinary and administrative discharges Life changes – family demands and children Career development and opportunities Retirement Struggling to adapt to military life Impact of ageing in lower ranks
Transition of Military Personnel
Symptomatic
Distress
Transition
Stress
Role Integration
strains Into civilian
roles
During Military Service Post DischargeADF Transition Research Program
Middle East Area of Operations (MEAO) Health
StudiesADF Transition Research Program MEAO Census Study n=26,915 2010 ADF Mental Health Prevalence and Wellbeing Study n=50,049 – response rate 48.9% Compared with the 2007 National Mental Health Prevalence and Wellbeing Study Enriched sample for CIDI interviews then weighted to the population
12-month Mental Disorder in the ADF compared to
the Australian CommunityHighest Rates in the Younger Veterans – leave not detected
PTSD and multiple trauma exposure
Impact of childhood trauma and disorder in
the ADF compared to the civilian population
Higher rates of non
interpersonal childhood
traumas in ADF than the
civilian population
Only significant traumas in
childhood associated with adult
disorder are interpersonal ones
The effects are mediated
through childhood anxiety
disorders
These interact with adult
Syed et al under review traumasMilitary Populations
Currently
serving
-Deployments Ex-serving
-Health services and
-Training accidents
-Occupational
veterans
stresses population
New
recruitsTransition Wellbeing Research
Program 2015
Follow up all who have transitioned from
the ADF from 2010 to 2014 (18% of
n=23,974)
Follow previous responders who remain
in the ADF (42% of n= 20,231)
Combat Study following up n=1871 who
were in MEAO Prospective StudyMilitary Populations
Currently
serving
-Deployments Ex-serving
-Health services and
-Training accidents
-Occupational
veterans
stresses population
New
recruitsDemographics
Transition Characteristics in Transitioned ADF
Reservists (53.83%) compared to ex-serving (45.88%).
Medically Fit 73.29%
12.35 years of regular service
» 36.6% in the 4-7.9 years
» 23.15% 20+ years.
Discharged at own request (53.58%),
20.38% medically discharged (N=5082)
non-voluntary discharge – administrative (3%, N=757)
Main reason for transition: impact of service life on family
(10.21%)
3.42% not living in stable housing in last 2 months (N=853)
2.99% (N=746) arrested since transition,
Slide 39 » 2% (N=516) convicted, only 17 people imprisoned.
68% employed12mth ICD-10 in Transitioned ADF
Transitioned ADF
ICD-10 12 mth
(N=24932)
N % 95% CI
12 month ICD-10 Anxiety Disorder (incl. PTSD) 9232 37 32.6, 41.7
12 month ICD-10 Affective Disorder 5755 23.1 19.2, 27.5
12 month ICD-10 Alcohol Disorder
3219 12.9 9.8, 16.9
12 month ICD-10 Mental Disorder
11558 46.4 41.7, 51.1
12 month ICD-10 PTSD 4408 17.7 14.5, 21.3
The prevalence of disorder in the transition sample is 46.4% - more than
double the rate in the ADF Mental Health Prevalence and Wellbeing (MHPWS)
study in 2010.12mth ICD-10 Anxiety Disorder
in Transitioned ADF
ICD-10 Anxiety
Transitioned ADF (N=24932)
Disorder
N % 95% CI
Panic Attack 4244 17 13.8, 20.8
Panic Disorder 1344 5.4 3.6, 8.0
Agoraphobia 2975 11.9 9.1, 15.5
Social Phobia 2738 11 8.4, 14.3
Specific Phobia 1936 7.8 5.8, 10.3
Generalised Anxiety
917 3.7 2.2, 6.0
Disorder
Obsessive
1029 4.1 2.6, 6.6
Compulsive Disorder
Posttraumatic Stress
4408 17.7 14.5, 21.3
Disorder
Any Anxiety Disorder 9232 37 32.6, 41.7
• The prevalence rate of PTSD of 17.7% is more the double the rate in the 2010 ADF
MHPWS Study.
• High rates of agoraphobia and social phobia suggest degree of social isolation and
withdrawal12 month ICD-10 Disorder and Suicidality:
Transition Predictors
• ICD-10 Disorder but tends to increase with time since
discharge particularly for PTSD
• ADF members who transitioned less than 1 year ago reported
the lowest level of psychological distress
• 1 year post-transition is where psychological distress, anger,
generalised anxiety, and depression first develops .
• PTSD symptoms, depression, suicidality, anxiety and both
types of drug use tend to peak around the 3 year mark.
• Overall, alcohol use and problem drinking showed no
association with years since transition.
Slide 42Treatment Seeking Seeking assistance within one year of concern onset of those with a mental health concern » 45% within 3 months » another 25% between three months and a year » 18% waited three or more years. Approx 65% of both current and ex-serving endorsed one or more stigma item
Military Populations
Currently
serving
-Deployments Ex-serving
-Health services and
-Training accidents
-Occupational
veterans
stresses population
New
recruits
22% 46.4%Nature of discharge
Full time Active
service Reserve
Inactive
Reserve
Fully discharged
-Veteran
-Ex-servingHow effective are the evidence based
treatments?Meta Analysis of Treatment in
Military Populations
Approximately 66% of patients receiving CPT and
PE retained their PTSD diagnosis after treatment
(range 60-72%)
Despite 49-70% having clinically meaningful
improvement
Prolonged exposure marginally superior compared
to non-trauma focused psychotherapies
Need to improve existing treatments and test novel
evidence based treatments
– Steenkamp et al JAMA 2015, 314;489-500The Issue of Severity and Stage as a predictor of treatment response
Curve of effect size versus symptom severity for psychotherapy for PTSD
What about pharmacological
treatments?
Importance of personalized approachThe need for new biologically based
treatment approaches supported by
evidence
The chronicity and disability
associated with PTSDCRP predeployment predicts PTSD
symptoms 3 months post deployment
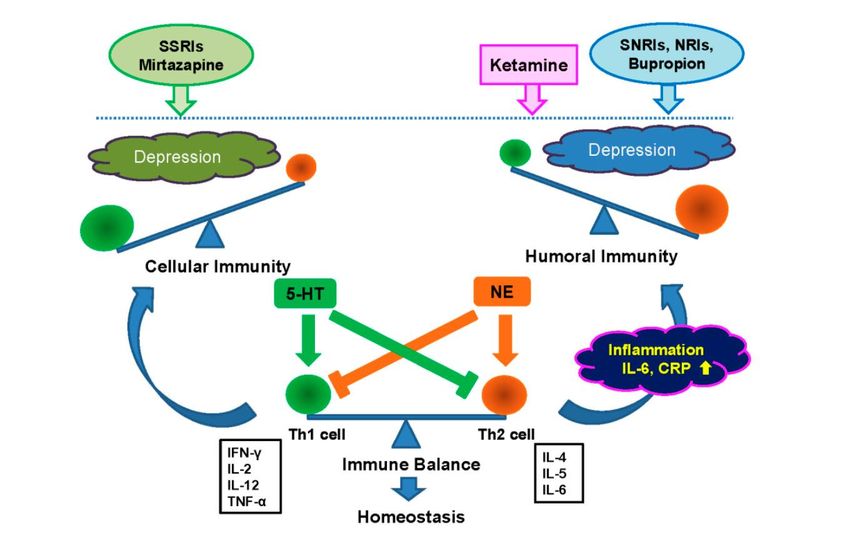
JAMA Psychiatry 2014Antidepressants act on peripheral
inflammation
Hashimoto Int J Mol Sci 2015CRP Predicts Differential Response to
SSRI vs. SSRI+Bupropion
Jah MK et al. Psychoneuroendocrinol 2017; 78: 105-13Is PTSD a systemic illness rather
than a psychological disorder?
Is this a critical question for developing
better treatments, particularly in the
biological domain?PTSD as Systemic Disease Extent of comorbidity of with physical disorder Decreased life expectancy Somatic symptoms are an integral part of the disorder Underpinned by systemic dysregulation of immune function and autonomic function
Mortality of Australian Troops
After World War 1
The Burnt Out Soldier – 13% greater mortality
if had fought on the Western Front. This
represented a decreased life expectancy of 4
years – Butler “The War Damaged Soldier”
1933 CensusMedical Comorbidities of PTSD
Controlling for sociodemographics and psychiatric illnesses,
PTSD was associated with significantly higher odds of having
» asthma
» chronic obstructive pulmonary disease
» chronic fatigue syndrome,
» Rheumatoid Arthritis
» fibromyalgia,
» migraine headaches,
» Cancer
» Cardiovascular – hypertension and high incidence of MI and CVD mortality
» Gastrointestinal
» pain disorders
» Epilepsy
» Renal and autoimmune disorders
McLeay et al MJA 2017Somatic Comorbidities of PTSD Meta-analysis of 9,673 individuals in middle age with PTSD and 6852 general population controls (Rosenbaum et al, Metabolism 2015) » Metabolic syndrome 38.7% (RR=1.82 CI1.7-1.9) » Hypertension 76.9% (Sumner et al 2016) » Hyperglycaemia 36.1% (Vaccario et al 2014) Lohr et al (2015) -PTSD should be conceputalised as a systemic disorder due to premature mortality
Possible causal pathways
PTSD
Biological
Dysregulation
Physical
DisorderThe need for clinical staging in
PTSD
Different phenotypes that need to be
addressed in treatment
Staging is a method for clarifying the
issue of longitudinal course and the
changing neurobiology
McFarlane et al Clinical Psychiatric Reports 2017Staging model of PTSD
0. Trauma exposed no symptoms but at
greater risk with further exposure
1a. Minor symptoms
1b. Subsyndromal PTSD – similar to PTSD
2. First episode of brief duration
3. More enduring or relapsing disorder
following treatment
4. Chronic, severe and treatment unresponsiveJAMA Psychiatry 2018
Erich Maria Remarque - All Quiet on the Western Front “Because one thing has become clear to me: you can cope with all the horror as long as you simply duck thinking about it - but it will kill you if you try to come to terms with it.” (p100)
The Farmer Remembers The Somme
I have returned to these:
The farm, and the kindly Bush, and the young calves
lowing;
But all that my mind sees
Is a quaking bog in a mist - stark, snapped trees,
And the dark Somme flowing
- Vance PalmerThank you Questions
You can also read

















































