Clinical Monthly 198th Edition
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

198th Edition Clinical Monthly

The Clinical Monthly Team
Abi Peck
Editor
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: Hands and spinal pathology, netball rehab
Joe Russell
News of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: Persistent pain and tendons
Josh Featherstone
Fracture of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: I love rehab
Scott Rowbotham
Podcast of the Month
Qualified: BSc (Hons) Physiotherapy
Clinical Interests: climbing and improving physical activity for children and
adults with long term disabilities
Lee Platt
Journal of the Month
Qualified: MSc (Hons) Physiotherapy
Clinical Interests: all areas in MSK
2
News of the Month
#NewsOfTheMonth by Joe Russell
MSK guidelines summary
https://bjsm.bmj.com/content/early/2019/03/02/bjsports-2018-099878
This month I would like to focus on a single piece of research that has been published.
This is a systematic review followed by a critical appraisal of best practice guidelines
across the MSK field. This has been conducted by some well known authors in the field.
The conclusion of the paper can be summarised in 2 tables which summarise some of
the common issues in MSK at the moment and propose consistent clinical recommen-
dations. Some of these are ingrained in our clinical practice such as patient centred
care and carrying out a physical assessment. Some, however, are more challenging to
some of our or our colleagues’ beliefs.
My question here is how appropriate is it to compare and assess clinical practice guide-
lines across a whole field. They considered guidelines on spinal, hip, knee and shoulder
pain as they identify these as the most common presentations and excluded guidelines
on trauma, single treatment modalities and complimentary therapies. They assessed
this using a validated standardised tool with multiple assessors. They combined experts
from across a range of fields within MSK. They identified recommendations into ‘Should
do’, ‘Could do’, ‘Do Not Do’ and ‘Uncertain’ with a narrative summary. As such they
have considered an effective spread of information and used experts to appraise it us-
ing their expertise and a validated assessment tool.
Implications for us in practice. Aside from the 11 statements in the box included here I
would strongly advise you all to read this paper and make up your own minds. It is a pa-
per which will probably be used significantly to influence the future shape of MSK ser-
vices at clinical, commissioning and national policy level.
3
News of the Month
#NewsOfTheMonth by Joe Russell
4
News of the Month
#NewsOfTheMonth by Joe Russell
5
Differentials of the Month
Shoulder Differentials by Josh Featherstone
Subjective: 50 year old female presented to clinic with 4 month history of shoulder pain that is
Last months idiopathic in onset.
Clinical case Objective: Reduced AROM and PROM. 5/5 strength.
The working diagnosis of last issues ‘differential diagnosis’ case study is frozen shoulder.
Patho-aetiology.
Primary frozen shoulder is an idiopathic onset of shoulder stiffness and pain, secondary to an inflammatory contrac-
ture of the shoulder capsule (Tamai et al 2014). Increased collagen and capsular fibrosis are documented illustrating an
inflammatory process and synovitis (Ibid 2014).
Frozen shoulder symptoms and subjective history taking usually involves a story of gradual onset of pain in the arm;
idiopathic in onset. Sleep problems especially when laying on the affected side; an observed reduction in shoulder
joint ROM secondary to stiffness and a reduction in passive glenohumeral joint ROM especially into external rotation
with normal radiographs (Lewis 2015).
In the context of our case study, only primary frozen shoulder will be discussed, but it is important to understand that
frozen shoulder can be categorised into two sub groups. These are primary frozen shoulder (idiopathic onset of capsu-
lar stiffness and pain), and secondary frozen shoulder (possible associated aetiology to reason the capsular stiffness
and pain).
Secondary frozen shoulder can be further sub-categorised into:
Intrinsic factors such as tendinopathies of the shoulder.
Extrinsic contributors consisting of frozen shoulder onset following trauma, cervical radiculopathy and iatro-
genic onset secondary to surgery such as ipsilateral breast surgery.
Systemic factors such as diabetes, hypothyroidism.
(Tamai et al 2014, Lewis 2015).
Frozen shoulder onset is between the age of 45-60 (Kelley et al 2013). The mean age of onset for primary frozen shoul-
der is fifty and in China and Japan it is known as the ‘fifty-year-old shoulder’ (Lewis 2015). It is considered that three
stages occur in frozen shoulder. These are known as the freezing, frozen and thawing stages and that the average du-
ration of symptoms range between 12-42 months (Kelley et al 2013, Lewis 2015). The most important message to re-
lay to our patient is that it will get better naturally, eventually (Jones et al 2013). In fact, a qualitative study found that
key themes regarding frozen shoulder from a patient’s perspective included; anxiety regarding what it is and the need
for a definitive diagnosis and prognosis (Jones et al 2013). Jones et al therefore suggests that to address these patient
concerns, a working diagnosis should be quickly established for most patients if frozen shoulder is suspected and edu-
cation/management about the pathology (Ibid 2013).
Management and treatment options.
There is weak supporting evidence for physiotherapy interventions including joint mobilisations, soft tissue mas-
sage and joint stretches to name a few to improve primary frozen shoulder however, these may provide a patient
transient improvement in their symptoms short term.
Given the duration for symptoms to last, resolution or reduction in symptoms sooner is an understandable ex-
pectation from patients therefore the shoulder pathway for Frozen shoulder patients in East Suffolk enables a
smooth transition from an outpatient physiotherapy assessment and diagnosis to onward referral to the muscu-
loskeletal assessment service at Ipswich Hospital.
It is there where decisions will be made to manage patients pain better through a range of treatments. Most
commonly a hydrodistension procedure will occur. This is an injection of high-volume sodium chloride into the
glenohumeral joint to increase the capsular volume, distend the capsule and hopefully improve joint
ROM/symptoms. (Lewis 2015).
6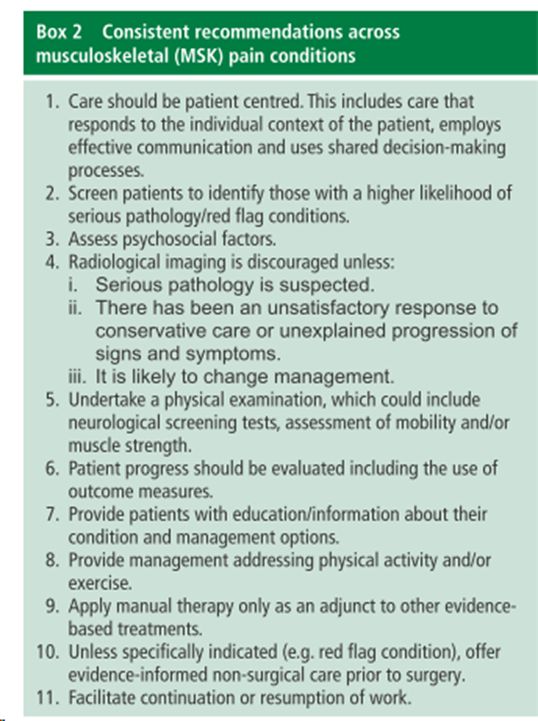
Differentials of the Month
Shoulder Differentials by Josh Featherstone
Last months differential diagnosis has been revealed as a frozen shoulder .
This months differential diagnosis is detailed below, lets see how well you can do!
Clinical case
Differential diagnosis
Subjective Ax:
A 75-year-old male attended clinic reporting 1) GHJ OA
an idiopathic onset of shoulder pain.
Sleeping on the affected side is difficult and he
finds that reaching across his body to put on
his seat belt or drying his opposing shoulder 2) ACJ pain/OA
to be very symptomatic.
Objective Ax:
3) Rotator cuff pathology
On assessment he has relatively good active
neck and shoulder ROM but reports discom-
fort into the top of his shoulder at his end of
range shoulder abduction and elevation.
He has good passive glenohumeral joint ROM
with no recreation of pain other than the feel-
ing of tightness toward his end or ranges.
Resisted testing of the shoulder shows no true
weakness other than discomfort on resisted
shoulder abduction.
References from previous slide:
Jones S, Hanchard N, Hamilton S, Rangan A. 'A qualitative study of patients perceptions and priorities when living with primary frozen shoulder' BMJ
Open, 3 (9): 1 - 9
Kelley MJ, Shaffer MA, Kuhn JE, Michener LA, Seitz AL, Uhl TL, Godges JJ, McClure PW (2013) ‘shoulder pain and mobility deficits: Adhesive Capsulitis.
Clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American
physical therapy association’ J orthop sports phys ther 43 (5): A1-A31
Lewis J (2015) ‘Frozen shoulder contracture syndrome - Aetiology, diagnosis and management’ Manual Therapy 20: 2-9
Tamai K, Akutsu M, Yano Y (2014) ‘Primary frozen shoulder: brief reiveiw of pathology and imaging abnormalities’ J Orthop Sci 19: 1-5
7
Podcast of the Month
# Podcasts by Scott
Last months podcast revealed
The Physio Matters Podcast Session 62 –
A Helping Hand with Sarah Mee and Debs Stanton
1) What are the key subjective and objective findings in hand assessment?
Listen to their entire “journey” without interruption. You will understand
A finger goniometer is crucial for accurate measurement and understanding of
progression or regression with rehabilitation
Grip testing is useful for motivation and compliance
Differences between active and passive range of movement vital. Distraction and
gliding of carpus can be informative for diagnosis
Consider metabolic causes – diabetic neuropathies, poor blood sugar control can
have an effect on nerve irritations
Do not forget to assess more proximally. Shoulder and trunk weakness will exac-
erbate any hand symptoms due to inefficient movements and overstressing of the
distal limb due to proximal weakness.
Carpal tunnel testing has poor sensitivity and specificity with phalens and reverse
phalens therefore consider referral on for nerve conduction studies; in particular if
false negative but subjective picture fits.
Be vigilent with skin colour changes, mottling and swelling. Discolouration of the
nail is a red flag and shouldn’t be ignored.
Asymmetry also is a concerning sign.
2) What are the key differential diagnosis princi-
ples?
Always check the neck! Need to exclude any
brachialgia
Past medial history is vital; diabetes (if poor-
ly controlled blood glucose levels) and epi-
lepsy due to medical management effects
peripheral circulation
Acutely tender nails and psoriasis will lead
you to rheumatological causes rather than
mechanical.
8
Podcast of the Month
# Podcasts by Scott
Gout and septic arthritis cause chronic low levels of inflammation that will not be
obvious on clinical examination. If suspecting inflammatory cause you should
have a low threshold for referral to ultrasound.
Ganglions are cosmetic and should disappear. Giant cell benign lumps will let light
pass through, destructive heberden’s nodes will not – need surgical opinion as ini-
tially painful, is a sign of arthritis.
3) What is the best practice for hand management?
Repetitive strain is a 24 hour problem. It is not just at the workplace. If a person is
very irritable effective changes need to be made at home and in daily life also.
Regular changing of position will avoid any overstressing or repetitive task.
Phased return is vital; largely attempting to change position or rest every 20
minutes wherever possible.
The thumb is most functional and stable in a slightly abducted position. Any ad-
ducted used e.g. phone will place extra demand on the CMC joint.
Stabilisation tripod grip with thumb abducted holding a piece of paper and other
hand ripping the paper is an excellent low level isometric activity for thumb
Splinting for sustained periods is very poor for management due to associated at-
rophy therefore low level isometrics and limited range strengthening should be
incorporated wherever clinically safe to maintain strength and function
Step down to neoprene or taping to maintain neuromuscular connections ASAP
“Arnold shoulder press” is an excellent activity to include due to isometric activity
at wrist, full supination to pronation and proximal limb strengthening
Night splinting for carpal tunnel MUST be done in 30 degrees extension due to a
neutral position is provocative for carpal tunnel.
Carpal tunnel exercises need to include gliding exercises for flexor digitorum pro-
fundus, superficialis and longus aswell as a median nerve glide exercise.
Next months podcast:
PT Inquest Episode 153: Lumbar Spine Injuries In Athletes
1) What types of lumbar spine injuries are there in sport?
2) What are the key points to note? i.e. severity and precautions with continued partici-
pation in sport
3) What is the best management for these types of injuries ? Conservative or surgical??
9
Journal of the Month
#Journal club by Lee Platt
Is combining gait retraining or an exercise programme with education better than
education alone in treating runners with patellofemoral pain? A randomised clinical
trial.
Esculier et al (2017)
Section A: Are the results of the trial valid?
1) Did the trial address a clearly focused issue? Yes – whether exercises or gait re-
training offer additional benefits in reducing symptoms of runners with PFJ pain
over education alone.
2) Was the assignment of patients to treatments randomised? Yes.
3) Were all of the patients who entered the trial properly accounted for at its con-
clusion? Yes 69 runners were recruited, 7 dropped out before the 8 week measure
and another 3 failed to return their follow up questionnaire at week 20.
4) Were patients, health workers and study personnel ‘blind’ to treatment? Run-
ners were not blind to their group however they were unaware of the other treat-
ment groups. The same evaluator performed all assessments. The physiotherapists
delivering the treatment sessions were independent to the study however it does
not state their level of knowledge regarding the trial.
5) Were the groups similar at the start of the trial? Yes they were all aged between
18 and 45, had PFJ pain for at least 3 months, minimum pain of 3/10 on VAS during
running and three additional tasks (stairs, kneeling, squatting or resisted knee ex-
tension) and had a score of 85/100 on the Knee Outcome Survey of the Activities of
Daily Living scale (KOS-ADLS).
Aside from the experimental intervention, were the groups treated equally? Yes all
3 groups were provided with the same education regarding load management and
advice with self-modifying their running.
Section B: What are the results?
1) What was the outcome of the study? All 3 groups showed significant improve-
ments in outcomes, however adding exercises or gait retraining did not provide ad-
ditional benefits compared with education alone.
2) How large was the treatment effect? The treatment effect was statistically signifi-
cant in all treatment groups however there were no statistically significant differ-
ences between the treatment groups.
10Journal of the Month
#Journal club by Lee Platt
Section C: Will the results help locally
1) Can the results be applied to the local population, or in your context? Yes – PFJ
pain is a common presentation seen in the running population and for many of the
patients we see therefore appropriate education on symptoms and management of
training loads should be included as a primary component of treatment. The au-
thors are keen to add that the results should not discourage clinicians from pre-
scribing gait retraining and exercises if judged necessary to target specific mecha-
nisms, especially as improvements were found in running mechanics and strength.
2) Were all clinically important outcomes considered? A ‘no treatment’ group was
not included therefore it is difficult to know the effects of spontaneous recovery
over the treatment duration or the placebo effect due to the clinician-patient inter-
action.
3) Are the benefits worth the harms and costs? There were no significant harms or
costs.
Next article: Blood flow restriction training in clinical
musculoskeletal rehabilitation: a systematic review
and meta-analysis (2017)
Luke Hughes, Bruce Paton, Ben Rosenblatt, Conor
Gissane,and Stephen David Patterson
Questions:
Section A: Are the results of the review valid?
1. Did the review address a clearly focused question?
2. Did the authors look for the right type of papers?
3. Do you think all the important, relevant studies were included?
4. Did the review’s authors do enough to assess quality of the included studies?
5. If the results of the review have been combined, was it reasonable to do so?
Section B: What are the results?
6. What are the overall results of the review?
7. How precise are the results?
Section C: Will the results help locally?
8. Can the results be applied to the local population?
9. Were all important outcomes considered?
10. Are the benefits worth the harms and costs?
11Find us on social media
‘Leading the way towards healthier, happier lives’
www.ahpsuffolk.co.uk
12You can also read