Covid-19, MIS-C and Return to Play; Lessons Learned from the Pandemic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Covid-19, MIS-C and
Return to Play; Lessons
Learned from the Pandemic
Jon F. Lucas, MD- Chief of Pediatric Cardiology, Prisma Health Upstate
Andrew M. Atz, MD – Chair of Pediatric, MUSC
Jodi A. Dingle, MD Chief of Pediatric Rheumatology, Prisma Health Midlands
Moderator: C. Osborne Shuler, MD- Chief of Pediatric Cardiology, Prisma Health
MidlandsLearning Objectives • Be able to identify the pediatric patients who have had a COVID-19 infection who might need restriction on their activity and cardiac evaluation • Be able to list the potential long term effects of MIS-C diagnosis
Learning Objectives • Be able to identify the pediatric patients who have had a COVID-19 infection who might need restriction on their activity and cardiac evaluation • Be able to list the potential long term effects of MIS-C diagnosis • Be able to identify post COVID-19 mRNA vaccine myopericarditis
AAP •COVID-19 Interim Guidance: Return to Sports and Physical Activity •June 4, 2021
Evaluation for Resumption of Physical Activity/Sports Activity for Children and Adolescents with COVID-19 • Recent literature has reported a much lower incidence of myocarditis, 0.5% to 3%, than earlier in the pandemic. Children and adolescents who were found to have myocarditis were in the asymptomatic or mildly symptomatic category. Therefore, the phone/telemedicine visit should include appropriate questions about chest pain, shortness of breath out of proportion for upper respiratory tract infection, new-onset palpitations, or syncope. Any child or adolescent who reports these signs/symptoms should have an in- office visit that includes a complete physical examination, and consideration for an EKG should be given prior to clearance to return to physical activity.
Evaluation for Resumption of Physical Activity/Sports Activity for Children and Adolescents with COVID-19 • For those with moderate symptoms of COVID-19 (≥4 days of fever >100.4°F, ≥1 week of myalgia, chills, or lethargy, or a non-ICU hospital stay and no evidence of multisystem inflammatory syndrome in children [MIS-C]), an evaluation by their primary care physician (PCP) is recommended. People who test positive for SARS-CoV-2 should not exercise until they are cleared by a physician. PCP evaluation is currently recommended after symptom resolution and completion of quarantine. The PCP will review the American Heart Association 14-element screening evaluation with special emphasis on cardiac symptoms including chest pain, shortness of breath out of proportion for upper respiratory tract infection, new-onset palpitations, or syncope and perform a complete physical examination and an EKG. If cardiac workup is negative, gradual return to physical activity may be initiated after 10 days have passed from the date of the positive test result, and a minimum of 10 days of symptom resolution has occurred off fever- reducing medicine. If cardiac sign/symptom screening is positive or EKG is abnormal, referral to a cardiologist is recommended. The cardiologist may consider ordering a troponin test and an echocardiogram at the time of acute infection. Depending on the patient’s symptoms and their duration, additional testing including a Holter monitor, exercise stress testing, or cardiac magnetic resonance imaging (MRI) may be considered. If cardiac workup is negative, gradual return to physical activity may be allowed after 10 days have passed from the date of the positive test result, and a minimum of 10 days of symptom resolution has occurred off fever-reducing medicine.
Evaluation for Resumption of Physical Activity/Sports Activity for Children and Adolescents with COVID-19 • For children and adolescents with severe COVID-19 symptoms (ICU stay and/or intubation) or MIS-C, it is recommended they be restricted from exercise for a minimum of 3 to 6 months and obtain cardiology clearance prior to resuming training or competition. Coordination of follow-up cardiology care should be arranged prior to hospital discharge. Other testing may be ordered based on the child or adolescent’s sign and symptoms.
Post-vaccination myopericarditis case • 16 y/o, previously healthy, no antecedent URI Sx • Developed chest pain 48 hours after second Pfizer vaccination • Outlying ED evaluation demonstrated elevated troponin and ST elevations consistent with pericarditis • Rapid resolution of symptoms with anti-inflammatories • No arrhythmias or myocardial dysfunction • Troponin level returned to normal within 2 weeks of onset of Sx • ECG normal 48 hours after initial symptoms
Returning To Play After Coronavirus Infection: Pediatric Cardiologists' Perspective Jul 14, 2020 | Peter N Dean, MD, FACC; Lanier Burns Jackson, MD; Stephen M. Paridon, MD
MIS-C Case
MIS-C Overview
What is MIS-C?
• Multisystem Inflammatory Syndrome in Children associated with
COVID-19
• Similarities to Kawasaki Disease, but does appear to be phenotypically
distinct
• Case Definition (CDC):
• Individual 2 organ
involvement
• No plausible alternative diagnosis
• + for current or recent SARS-CoV-2 infection by PCR, serology, or antigen test,
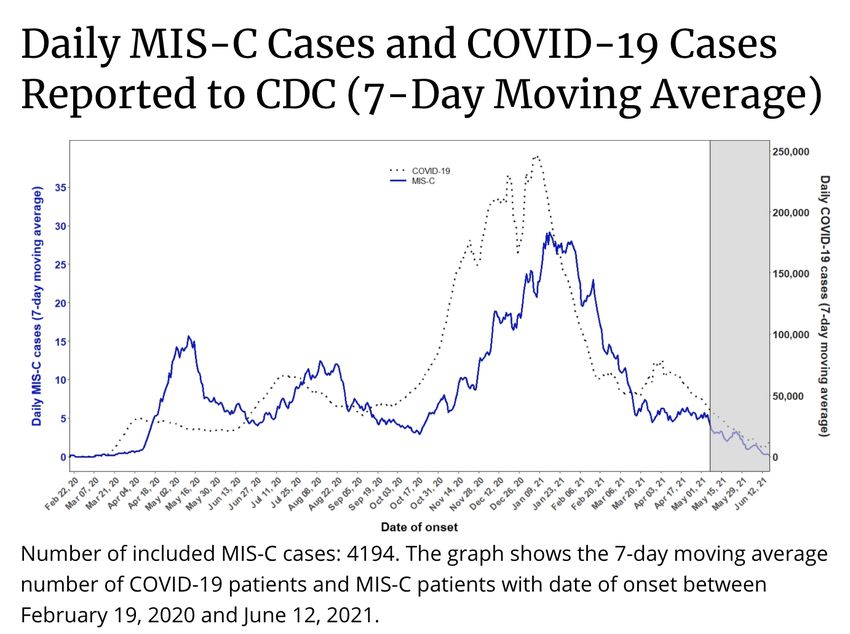
or exposure to confirmed COVID-19 case within the 4 weeks priorDemographics • As of June 28, 2021, there have been 4196 cases in the US with 37 deaths • Median age of patients with MIS-C is 9 years • 62% of patients are Hispanic/Latino or Black • 60% of reported cases are male
Evaluation and Treatment
• Laboratory evaluation for signs • Fluid resuscitation
of inflammation • IVIG and Steroids
• Elevated CRP, ESR, fibrinogen, • Anakinra for refractory/severe
procalcitonin, d-dimer, ferritin, cases
LDH, elevated neutrophils,
reduced lymphocytes, low • Aspirin
albumin
• Inotropic and respiratory
• BNP and Troponin
support if needed
• Echocardiogram • Thrombotic prophylaxis if
• SARS-CoV2 PCR or antigen indicated
testing and serologyCardiac Manifestations of COVID • Myocarditis can occur with acute COVID • Minimal cases of this in children in our combined experience • Cardiac involvement in MIS-C • Significantly depressed EF and hypotension • Post- COVID vaccination myocarditis
Post-vaccination myopericarditis case • 16 y/o, previously healthy, no antecedent URI Sx • Developed chest pain 48 hours after second Pfizer vaccination • Outlying ED evaluation demonstrated elevated troponin and ST elevations consistent with pericarditis • Rapid resolution of symptoms with anti-inflammatories • No arrhythmias or myocardial dysfunction • Troponin level returned to normal within 2 weeks of onset of Sx • ECG normal 48 hours after initial symptoms
Symptomatic Acute Myocarditis in Seven Adolescents
Following Pfizer-BioNTech COVID- 19 Vaccination
Mayme Marshalla, MD, Ian D. Fergusonb, MD, Paul Lewisa, MD, MPH, Preeti
Jaggic, MD, Christina Gagliardod,e, MD, James Stewart Collinsf, MD, Robin
Shaughnessya, MD, Rachel Carona, BA, Cristina Fussa, MD, Kathleen Jo E.
Corbinb, MD, MHS, Leonard Emurenb, MBBS, PhD, Erin Fahertyb, MD, E.
Kevin Hallb, MD, Cecilia Di Pentimad,e, MD, MPH, Matthew E. Osterc, MD,
MPH, Elijah Paintsilb, MD, Saira Siddiquid, MD, Donna M. Timchakd,g, MD,
Judith A. Guzman-Cottrilla, DO
Affiliations: aOregon Health and Science University School of Medicine,
Portland, Oregon; bYale University School of Medicine, New Haven,
Connecticut; cEmory University School of Medicine and Children’s Healthcare
of Atlanta, Georgia; d Goryeb Children's Hospital, Atlantic Health System,
Morristown, New Jersey; e Thomas Jefferson University, Philadelphia,
Pennsylvania; fSpectrum Health, Grand Rapids, Michigan; gColumbia
University Irving Medical Center, New York, New York
June 4, 2021•More than 177 million people have received at least one dose of COVID-19 vaccine in the United States, and
CDC continues to monitor the safety of COVID-19 vaccines for any health problems that happen after
vaccination.
•Since April 2021, there have been more than a thousand reports to the Vaccine Adverse Event Reporting
System (VAERS) of cases of inflammation of the heart—called myocarditis and pericarditis—happening after
mRNA COVID-19 vaccination (i.e., Pfizer-BioNTech, Moderna) in the United States.
•These reports are rare, given the hundreds of millions of vaccine doses administered, and have been
reported after mRNA COVID-19 vaccination, particularly in adolescents and young adults. View the latest
information.
•CDC and its partners are actively monitoring these reports, by reviewing data and medical records, to learn
more about what happened and to understand any relationship to COVID-19 vaccination.
•Most patients who received care responded well to treatment and rest and quickly felt better.
•Confirmed cases have occurred:
• Mostly in male adolescents and young adults age 16 years or older
• More often after getting the second dose than after the first dose of one of these two mRNA COVID-
19 vaccines
• Typically within several days after COVID-19 vaccination
•Patients can usually return to their normal daily activities after their symptoms improve. They should speak
with their doctor about return to exercise or sports.
•CDC continues to recommend COVID-19 vaccination for everyone 12 years of age and older, given the risk
of COVID-19 illness and related, possibly severe complications.
•Getting vaccinated is the best way to help protect yourself and your family from COVID-19.
CDC, June 23, 2021You can also read