COVID-19 Response ECHO for Oregon Clinicians Session 6 March 18, 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19 Response ECHO for Oregon Clinicians Session 6 March 18, 2021

Introduction to COVID-19 ECHO
• Everyone is muted
• Use the Chat Box to submit questions/comments/share links & resources
• We will strive to select questions directly relevant to the presentations for asking during the session,
but will not be able to address all questions. Questions not directly answered will be collated and
used in the planning of future sessions
• All sessions will be recorded and available for viewing after the session within 24
hours
• Resources and transcript of today’s chat box, PowerPoint slides, and video
recording will be posted on our ECHO Network website at
www.connect.oregonechonetwork.org (where you registered)
• PLEASE fill out the post-session survey that you’ll receive by email today
2
COVID-19 ECHO Faculty
Facilitator: Eric Wiser, M.D. (OHSU Gabriel Park)
Supporting Faculty:
Holly Tse, M.D. (Legacy Health, Medical Director of Medical Home)
Jay Richards, D.O. (Aviva Health, Chief Medical Officer)
Shelby Lee Freed, M.S.N, F.N.P.-B.C. (OHSU Richmond Clinic)
Tom Jeanne, M.D., MPH (OHA, Deputy State Health Officer and Deputy State
Epidemiologist)
Program Support
Tuesday Graham, B.S. (OEN Project Manager)
Miriam Wolf, B.S. (OEN Program Coordinator)
3
Today’s Agenda
• OHA Update
• Brief Q & A for OHA
• Specialty Presentation: Testing – Yassmine Akkari, PhD, Legacy
Lab
• Brief Q & A for Yassmine Akkari
4
Oregon Health Authority
COVID-19 Update
March 18, 2021
Tom Jeanne, MD, MPH
Ariel Smits, MD
5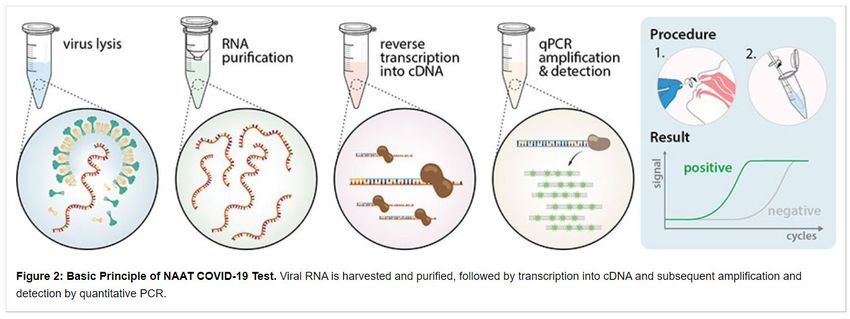
Oregon Health Authority
COVID-19 Update
March 18, 2021
Tom Jeanne, MD, MPH
Ariel Smits, MD, MPH
6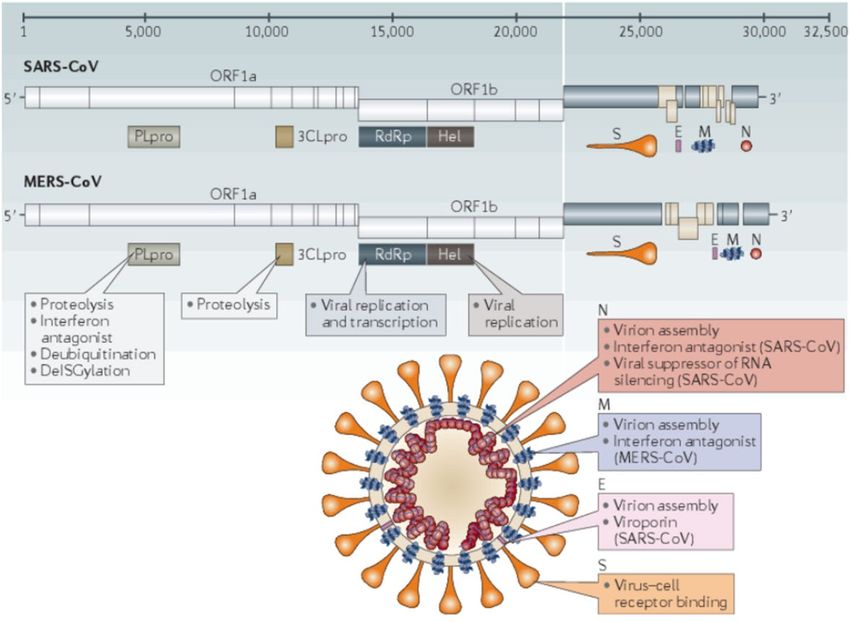
COVID-19 in Oregon
As of March 17:
• 160,259 total cases
• 8,945 hospitalized cases
• 2,349 deaths
7
Weekly COVID-19 Report
For the week of March 8–March 14
• 2,272 new cases were recorded, a 14% decrease from two weeks ago
• 130 new hospitalizations, a 21% decrease from two weeks ago
• 26 Oregonians died in association with COVID-19, a 54% decrease from
two weeks ago
From March 7–March 13
• 94,079 tests for COVID-19
• 3.6% of test results were positive last week
8
Declining Surge in Hospital COVID-19 Census 9 9
Vaccination Data Dashboard (https://covidvaccine.oregon.gov)
1011
Testing Update
12Testing Trends
From 2/28–3/6, estimated testing volume was 118,847 and percent
positivity was 2.1% (goal ≤ 5%)
13Testing Needs and Gap Analysis 14
Testing Strategy Updates
Expanding testing access with new federal funding:
1. Bridging exposed contacts to testing through mail-in testing resources
• OHA would cover cost for uninsured
2. Expanding CBO partnerships to plan and assist at testing events
• This work is currently being done voluntarily
• OHA would fund CBOs for their collaboration with this essential work
3. Expanding CBO partnerships to understanding testing barriers in
disproportionately impacted communities
• OHA would fund CBOs to gather detailed information that could inform public health efforts
4. Supporting targeted testing of disproportionately impacted populations
through regional framework
• Reimbursement for testing of uninsured populations
5. Supporting OHA mobile testing
15Regional Testing Framework Progress
190 low-barrier testing events to date and over 23,000 tested
MSFW H2A/B visa testing initiated
• Will be offered to all farms upon arrival of workers
Asked by HHS testing provider to function as a testing mentor to other states
Regional Testing Partners identified for all regions
• Region 1: OHSU
• Region 2: Santiam Hospital
• Region 3: McKenzie-Willamette
• Region 5: Asante
• Region 6: One Community Health
• Region 7: Sky Lakes
• Region 9: Grande Ronde
Mobile capacity
• OHSU received 3 vans: 1 operational, otherwise retrofitting
• OHA received 4 vans: retrofitting
• 3 CBO partners will receive vans
• HIV Alliance: Lane/Marion/Douglas/Josephine
• Neighborhood Health Care: Clackamas/Wash.
• White Bird Clinic: Lane
16Regional Testing Framework Progress
Distributed 750,000+ tests to partners statewide, including:
• Abbott BinaxNOW rapid point-of-care testing
• 402,600 BinaxNOW tests distributed to 246 testing partners including critical access,
primary care, LTCFs
• Strategic reserve for K-12 testing
• Abbott IDNOW rapid point-of-care testing
• 44 testing platforms and 70,000 tests distributed to testing partners
• Strategically distributed to areas of limited testing capacity and disproportionately affected
populations
• Thermofisher high-volume laboratory testing
• 8 testing platforms and 310,000 tests distributed to large healthcare testing partners
Building additional testing capacity in Oregon at UO, OSU, OHSU
17School Testing
School Testing
CDC issued new Operational Strategy for K-12 schools
• Recommends that all students and staff who develop symptoms at school or experience an
exposure be referred for testing
• Oregon could meet by mandating the K-12 testing project in all schools
• Oregon could meet by asking schools to refer out to community testing resources, but these do not
exist in all areas
• Access could be guaranteed through the first strategy, not through the second
• Screening may or may not be implemented
K-12 Testing in Oregon’s Schools project — over 800 registered
• Testing offered to all public and private K-12 schools
• Testing required under the following circumstances:
• K-12 schools operating in-person in counties above advisory metrics
• K-12 outdoor contact sports opening in High or Extreme levels
19School Testing in Oregon
A school testing administrator is assigned to perform and log all on-site
COVID-19 testing
• School nurse or trained medical professional if available
• Otherwise, anyone who is trained; does not need to be a medical
professional
• Must complete all required online training modules for the BinaxNOW
point-of-care antigen test and carefully review all training regarding PPE
• No CLIA-waiver application needed
20School Testing in Oregon
Oregon’s school testing program is currently for symptomatic and exposed
students and school staff only
• Screening using antigen testing is low-yield
• Sensitivity of antigen tests is low in asymptomatic people
• People more likely to be infected are less likely to participate
• Positive tests that subsequently have a negative molecular test are
confusing
Funding forthcoming ($10B) from HHS for surveillance testing in schools
using a regional framework
• Identifying laboratory partners now; no operational plan yet
21School Testing in Oregon
Oregon’s school testing program is currently for symptomatic and exposed students and
school staff only
• BinaxNOW antigen tests
• 84.6% sensitivity (90.6% for specimens with CtSchool Testing in Oregon
• See Healthcare Partner Resources page for resources on school testing
• https://healthoregon.org/coronavirushcp
23What is a Given Test’s Sensitivity and Specificity?
• How to look up manufacturer-reported performance characteristics of any
COVID-19 test with FDA EUA
• https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-
emergency-use-authorizations-medical-devices/vitro-diagnostics-euas
• Find the right table
• Search in search box for test name
• Click the IFU link. Clinical performance section is typically near bottom
• Be sure to note the comparator used (usually PCR, which is not a perfect
gold standard!)
24SARS-CoV-2 Sequencing
SARS-CoV-2 Sequencing in Oregon
• Sequencing can inform public health response; unknown clinical
significance
• Academic laboratories in Oregon are doing sequencing
• The Oregon State Public Health Laboratory (OSPHL) will offer whole
genome sequencing for COVID-19 beginning in March 2021
• All labs that are sequencing are to submit results to GISAID open-source
repository
26Forthcoming Guidance from OHA
Criteria for requesting COVID-19 sequencing at OSPHL
• No cost at OSPHL, but must meet one or more of these criteria:
• Individual with history of international travel in the 14 days prior to the onset of COVID-19
• Individual meeting CDC vaccine breakthrough case definition
• Specimen with result on the Thermo Fisher TaqPath and Linea COVID-19 Assay Kit with spike
gene target failure
• Specimen criteria
• Received at OSPHL within 7 days of collection
• For specimens tested with PCR, only specimens with a cycle threshold (Ct) value ≤ 28
should be submitted for sequencing
• For specimens which have been tested using a method which does not report Ct values,
submit original material if acceptable for testing at OSPHL
• If no residual sample is available, submit the extract if available or collect a second specimen
for sequencing
27Variant case counts in Oregon
As of March 17, 2021 CDC’s new variant categories:
Variants of concern Variant of Interest
• Currently B.1.526, B.1.525, P.2
• B.1.1.7 (UK): 17
• P.1. (Brazil/Japan): 1 Variant of Concern
• Currently B.1.1.7,
P.1, B.1.351,
• B.1.351 (South Africa): 0 B.1.427, B.1.429
• B.1.427 (California): 0 Variant of High Consequence
• B.1.429 (California): 0 • None in the U.S. right now
28COVID-19 Literature Updates
BinaxNOW Rapid Antigen Testing
Prince-Guerra et al; January 22, 2021 MMWR Evaluation of Abbott
BinaxNOW Rapid Antigen Test for SARS-CoV-2 Infection at Two
Community-Based Testing Sites — Pima County, Arizona, November 3–17,
2020.
• Sensitivity of the BinaxNOW antigen test, compared with polymerase chain reaction
testing, was lower when used to test specimens from asymptomatic (35.8%) than
from symptomatic (64.2%) persons
• Near 100% specificity for both asymptomatic and symptomatic
• Advantages:
• Results in 15-30 minutes
• Lower requirement for resources
• High specificity and high PPV in settings of high pretest probability (e.g., providing testing
to symptomatic persons, to persons with a known COVID-19 exposure or where
community transmission is high).
30BinaxNOW Rapid Antigen Testing
Disadvantage: Low sensitivity
• Community testing strategies focused on preventing transmission using antigen
testing should consider serial testing to improve sensitivity.
• When the pretest probability for receiving positive SARS-CoV-2 test results is
elevated (e.g. for symptomatic persons or for persons with a known COVID-19
exposure), a negative antigen test result should be confirmed by NAAT.
• Asymptomatic persons who receive a positive BinaxNOW antigen test result in a
setting with a high risk for adverse consequences resulting from false-positive results
(e.g. in long-term care facilities) should also receive confirmatory testing by NAAT.
Unknown performance with viral variants
31Questions & Answers
Questions Moderated by Jay Richards, D.O.
Covid-19 Testing at Legacy Health:
March 2021 Updates
Yassmine Akkari, PhD, FACMG
Scientific Director, Cytogenetics and Molecular PathologyFacts about Viruses
All viruses mutate
Genetic changes in the viral genome happen as the virus makes new
copies of itself to spread and thrive. Most are inconsequential, few can
even be harmful to the virus' survival, but some can make it more
infectious or threatening to its host.
Long latency periods, increased viral load, and extended sickness
duration allows for viruses to mutate more readily
Safety measures to decrease transmission are
effective in reducing the mutation rates of viruses
March 19, 2021 LEGACY HEALTH 353/19/2021 LEGACY HEALTH 36
SARS-CoV-2 Around the World
The WHO uses information from reported unusual/adverse case trends to continually
sequence the COVID-19 viral genome and tracking increased transmissibility [Global
Initiative on Sharing All Influenza Database (GISAID)]
December 2019: first variant in China
February 2020: A D614G mutation emerged in early February, and by June 2020, it was
the main circulating strain globally.
> While the D614G variant had increased transmissibility, it did not cause more severe illness or alter the effectiveness
of existing laboratory diagnostics, therapeutics, vaccines, or public health preventive measures
August 2020: “Cluster 5” was in identified in North Jutland, Denmark. It has a combination
of mutations not previously observed.
> To date, following extensive investigation and surveillance, Danish authorities have identified only 12 human cases
of the Cluster 5 variant in September 2020, and it does not appear to have spread widely
December 2020: the SARS-CoV-2 VOC 202012/01 (Variant of Concern, year 2020, month
12, variant 01) emerged in South East England. This variant contains 23 nucleotide
substitutions. B.1.1.7
> Preliminary epidemiologic, modelling, phylogenetic and clinical findings suggest that SARS-CoV-2 VOC 202012/01
has increased transmissibility but no change in disease severity
December 18th, 2020: South Africa reports the emergence of 501Y.V2, because of a
N501Y mutation
> It is was shown to be associated with a higher viral load, which may suggest potential for increased transmissibility.
No clear evidence of the new variant being associated with more severe disease or worse outcomes
3/19/2021 LEGACY HEALTH 37How does the occurrence of these
variants affect our testing methodology?
3/19/2021 LEGACY HEALTH
38LLS Reported LLS Reported
FDA EUA SARS CoV-2 SARS CoV-2 TAT
Acceptable Sensitivity Specificity
Method Platform Reagent Test Components Specimen
(Manufacturer's Type
Package Insert) (Received testing Lab
to Resulted)
NP swab, 100.0% 100.0%
Molecular PCR Cepheid Flu A, Flu B, RSV,
4 in 1 Symptomatic nasal wash/Testing Methodology 3/19/2021 LEGACY HEALTH 40
Testing Methodology:
RT-PCR
3/19/2021 LEGACY HEALTH 41Legacy Laboratory Services: COVID-19 Testing
Roche 6800 Platform
ORF1a gene
Altona Diagnostics
Roche MagNA Pure 96
Roche MagNA Pure LC
Roche cobas z 480
S Gene
3/19/2021 LEGACY HEALTH 42COVID-19 Testing at Hospital Sites:
Xpert® Xpress SARS-CoV-2
Cepheid
> Emergency departments
> Inpatients
> 1 hour turnaround time
3/19/2021 LEGACY HEALTH 43“Analytical” Versus “Clinical” Sensitivity
Analytical Sensitivity:
> Ability of an assay to detect pathogen when present in a clinical
specimen
Clinical Sensitivity:
> Ability of a test to identify a patient’s overall infected status
> reflects various other factors that include the specimen-site and
method of collection, in conjunction with the burden of organism as a
function of anatomic location, disease severity, and time symptomatic
(and variability of these factors from individual to individual).
3/19/2021 LEGACY HEALTH 44Analytical Sensitivity: Legacy Results
Reference material purchased from Exact Diagnostics
Standard and 12 COVID-19 blind specimens (OSPHL Method Evaluation
Panel for nCoV-2019 RT-PCR) sent from the Oregon State Health Lab
5 positive samples obtained from the University of Washington (UW)
Virology laboratory
Patient and contrived samples (30 positives and 41 negatives)
100% Concordance
3/19/2021 LEGACY HEALTH 45Limit of Detection for the PCR Test
Roche 6800: 100 viral copies/ml
Cepheid: 250 Copies/ml
3/19/2021 LEGACY HEALTH 46Cross-Reactivity (Specificity)
• 1 Bordetella parapertussis positive
• 1 RSV positive
• 1 RSV/Influenza A H1 2009 positive
• 1 Coronavirus HKU1
• 2 Coronavirus OC43
• 1 Coronavirus NL63
• 5 Human Metapneumovirus
• 2 Coronavirus not typed
• 1 adenovirus/Coronavirus (not typed)/Human Metapneumovirus
No cross-reactivity observed
3/19/2021 LEGACY HEALTH 47Legacy Molecular Diagnostics Covid-19 Tests
139,100 patients; 5.05%
Roche 6800: Live Test
> ORF1a gene
> Vendor Communication: No sequences, including the UK variants, have been identified that have mutations in both
target regions; therefore, no impact on the performance of any cobas® SARS-CoV-2 test is anticipated.
altona/z480: Live Test
> S gene
> Vendor Communication: We are aware of the SARS-CoV-2 variant under investigation (VUI-202012/01, England,
United Kingdom) which is defined by variant spike protein mutations: deletion 69-70, deletion 144, N501Y, A570D, D614G,
P681H, T716I, S982A, D1118H. These mutations do not impact the performance of the S gene detection system.
Thermofisher: Validation in Progress
> ORF1a/b, N, and S genes
> Vendor Communication: If only the S gene drops out, the test is still positive. Report to the State
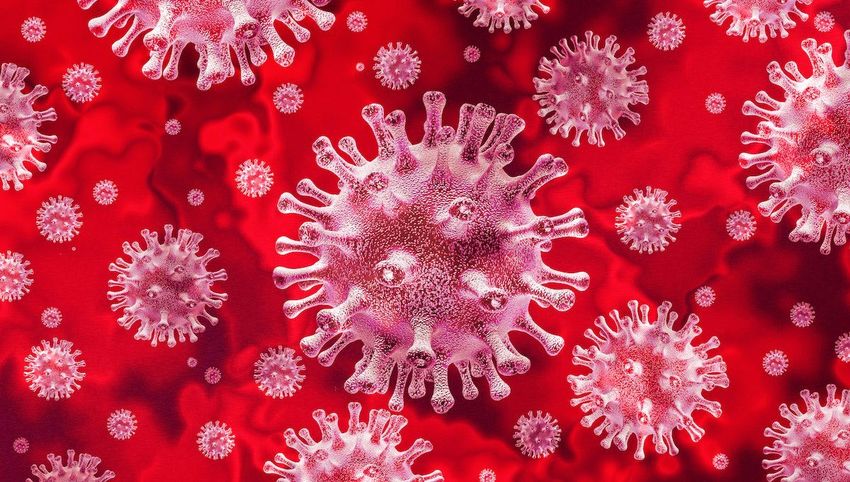
3/19/2021 LEGACY HEALTH 48Older Variant
Successful amplification
and extension
New Variant
5’ 3’
TACTAGTCCTAGGAG
No amplification
X “S gene drop out”
GATACTC
3’ 5’
For illustration purposes only
3/19/2021 LEGACY HEALTH 49Tracking “Inconclusive” Results Daily
3 Total runs (280 patients reported) = 3 Cobas 6800 runs, 0 Altona
runs
# COBAS Inconclusive results: 2
# Altona Inconclusive results: 0
# COBAS 6800 Positives: 22
# Altona Positives: 0
New Positives: 22
New Positivity %: 7.9%
Cumulative Test Performed: 112,422
Cumulative Positives: 5,966
Cumulative Positivity %: 5.3%
3/19/2021 LEGACY HEALTH 50Thinking Ahead..
90-day post infection and vaccine escape patients:
> Asymptomatic; tested as pre-op; positive test; CT values
> Symptomatic; sequencing to detect possible variants
3/19/2021 LEGACY HEALTH 51The use of SARS-CoV-2 PCR cycle threshold (Ct) values for
clinical decision-making
Definition: The Ct value refers to the number of PCR
cycles required to amplify the targeted viral nucleic acid
to a detectable level that is discernable from
background
In general, low Ct values indicate a higher viral density
and high Ct values generally indicate a lower viral
density
Growing interest in using Ct values as a surrogate
measure of viral copies in clinical specimens
3/19/2021 https://www.idsociety.org/globalassets/idsa/public-health/covid-19/idsa-amp-statement LEGACY HEALTH 52CAVEATS
> Definitive data to support the predictive value of Ct values in
these situations are lacking
> Ct values generated by qualitative PCR assays do not reliably
correspond to specific RNA concentrations
> Ct values generated by qualitative PCR assays are not
consistent across platforms
> multiple factors other than viral load are known to affect Ct values
> Qualitative test Ct values are not normalized to standardized
controls of known concentration
> respiratory specimen types are less amendable to quantitative
PCR testing
3/19/2021 LEGACY HEALTH 53Thank you!! Thank you!
Serology/Antibody Test at LCL
Beckman Dxl
Diasorin Liaison
Clinical utility:
> Detection of PCR-negative cases, especially for patients who present
late with a very low viral load below the detection limit of RT-PCR
assays, or when lower respiratory tract sampling is not possible
> Identification of convalescent plasma donors
> Epidemiologic studies of disease prevalence in the community
> Verification of vaccine response once antibody correlate(s) of
protection identified
> Drawbacks: false negative (early in disease course or mild disease)
and false positive with cross-reactivity with other Coronaviruses
3/19/2021 LEGACY HEALTH 55Questions Moderated by Shelby Lee Freed, FNP
Important Reminder
Next COVID-19 Response ECHO for Oregon
Clinicians:
Thursday, April 1 at noon: “VAERS Reporting
System”oregonechonetwork.org
58You can also read