Critical Care Nephrology 2018 - Christoph Schwarz
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Critical Care Nephrology
2018
Christoph Schwarz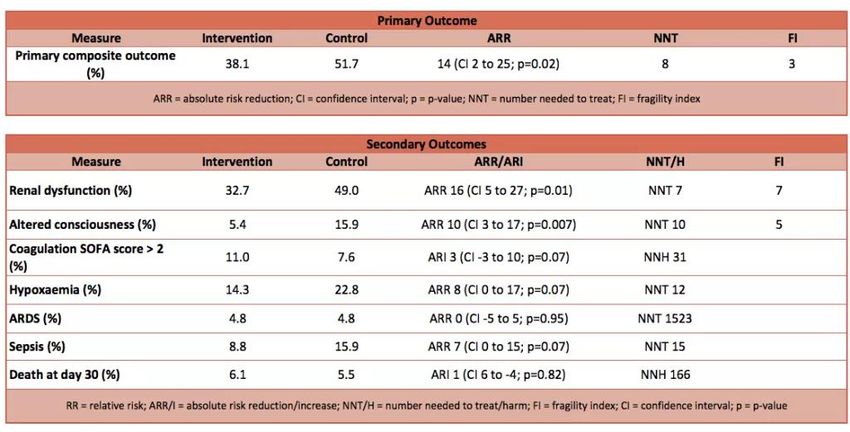
AGENDA 2018 • Diagnostic Tools – kinetic GFR • Hemodynamics 1: SPLIT-SALT-LICRA-SMART-SALT-ED • Hemodynamics 2: Selepressin – Angiotensin II • Kidney meets Liver • Acid-Base: Chloride and Gaps • GOMIC´s • News
Kinetic GFR - BASIC eGFR nur bei stabiler Nierenfunktion kGFR: Berechnung der GFR basierend auf Kreatininänderung über eine bestimmte Zeitperiode (inkl. geschätzte Krea-Generationsrate) Frage: Ist die kGFR den AKIN-Kriterien überlegen? Hat die kGFR einen anderen klinischen Nutzen?
Kinetic GFR vs. eGFR2
Bsp. Mann 70kg, 70 Jahre,
Kreatinin-Anstieg um:
0,1-1,9mg/dl in 24 Stunden
kGFR vs GFR2
80,0
70,0
GFR (ml/min)
60,0
50,0 AKIN 2
40,0
AKIN 3
30,0
20,0
10,0
AKIN 1
0,0
0 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9
KGFR CKD-MDRD 2
delta S-Kreatinin (mg/dl)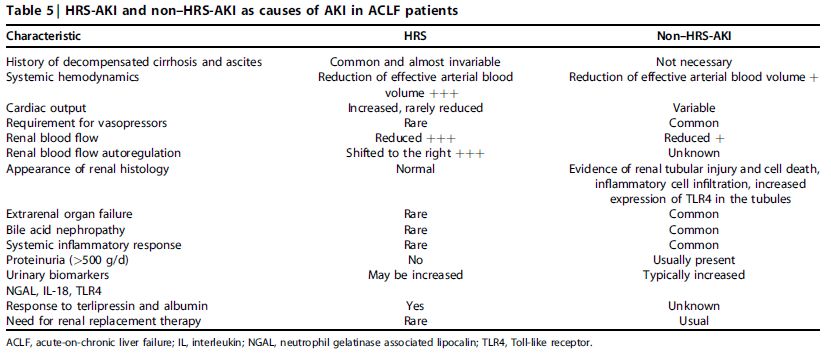
Kinetic GFR performs better than GFR-MDRD? Vergleich eGFR-MDRD(1) vs. kGFR kGFR
kGFR + AKIN = ?
Outcome bei baseline eGFR >70ml/min
kGFR < 30ml/min
additiv prädiktiven Wert für
Mortalität (unabh. AKIN)
und für Notwendigkeit einer
NET (bei AKIN3)
de Olivera Marques Critical Care 2017Hemodynamics - BASIC
Personalisierte Hämodynamik – Alter + Co-Morbiditäten
Was sollte gemessen werden?
– Blutdruck (MAP, DAP-CVP)
- Harnmenge
- Sono: Herz, Lunge, Pulswellenvariabilität,….
Wie sollte behandelt werden?
- Flüssigkeit
- Katechoamine
- Vasopressin, Angiotensin IIEffect of Individualized vs Standard Blood Pressure Management Strategies
on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing
Major Surgery (INPRESS)
Patienten= 298, >50 Jahre, medium-high risk Patienten
elektive abdominelle OP,
Randomisiert: RR±10% präoperativ vs. RR >80 mmHg systol.
Intervention: Noradrenalin
Primärer composite Endpunkt: SIRS oder 1 „Organversagen“
Futier E JAMA 2017Futier E JAMA 2017
Selepressin, a novel selective vasopressin V1A agonist, is an effective substitute for
norepinephrine in a phase IIa randomized, placebo-controlled trial in septic shock
patients
Selepressin selektiv V1a Rezeptor (kein Effekt auf renalen V2 Rezeptor)
53 Patienten mit septischen Schock unter Noradrenalintherapie erhalten
Selepressin vs.Placebo.
Russell JA Critical Care 2017
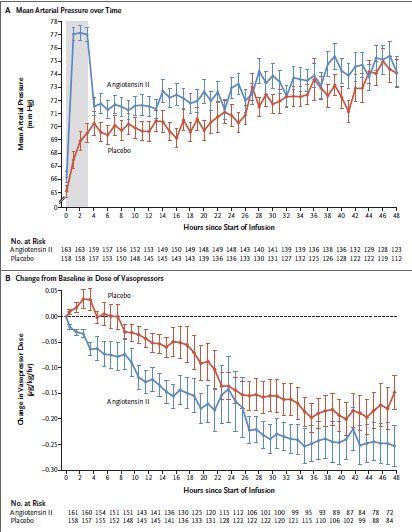
Endpoint: MAP > 60mmHg, beenden von NoradrenalinAngiotensin II in shock
ATHOS-3
Laurence William Busse KI reports 2017
Indikation: Septischer Schock
Therapie: Noradrenalin >2µg/kg/min + ATII vs. Placebo
Patienten: 344
Primärer Endpunkt: RR 3 Stunden nach Beginn der ATII Therapie
Ziel MAP: in ersten 3h 75 mmHg, danach >65 mmHg Khanna A NEJM 2017ATHOS-3 Endpunkt nach 3h:
Anstieg des RR > 10mmHg
oder MAP > 75mmHg:
AT II: 69%
Placebo: 23%
SAE: idem
AKIN:
4,9% (n=8) vs. 6,3% (n=11)
Khanna A NEJM 2017Volumentherapie SALINE vs. BALANCED SOLUTIONS
Chloride – Volume Therapy Volumentherapie mit NaCl 0,9% - negative Effekte in vielen retrospektiven (Observations)Studien Ära der randomisierten prospektiven Studien: 2016: SPLIT – kein Unterschied zwischen NaCl 0,9% und balanced solutions (Niere und Mortalität) 2017: LICRA und SALT 2018: SMART und SALT-ED 2019: PLUS-Trial
LICRA „Limiting I.V. Chloride to Reduce AKI“
1136 Patienten nach Herz-Chirurgischen Eingriffen
2 Perioden mit Infusion von NaCl 0,9%
2 Perioden mit Infusion von balancierten Lösungen (1xRLA, 1xPlasmalyte)
Endpunkt: delta Kreatinin, Rate an AKIN2 und AKIN3
Ergebnis: kein Unterschied im Outcome (Niere, Mortalität)
McIlroy D; Intensive Care Med 2017LICRA „Limiting i.v. Chloride to Reduce AKI“
ABER:
Intraoperativ: HLM – mit RLA gefüllt
ca. 50% der Patienten in der NaCl 0,9% Periode
erhielten intraoperativ balancierte Lösungen
Postoperativ: Volumengabe: ca. 1500ml
McIlroy D; Intensive Care Med 2017SALT – „isotonic Solution Administration Logistical Testing“
974 Patienten
– cluster randomized trial
NaCl 0,9% vs. balancierte Lösung
Infusionsmenge nach 7 Tagen:
ca.1300ml
Endpunkt:
MAKE30: kein Unterschied
Semler MW; Am J Respir Crit Care Med 2017MAKE 30 • In-hospital mortality = Death prior to hospital discharge • New receipt of RRT = Receipt of any modality of RRT prior to hospital discharge in a patient not known to have received RRT prior to ICU admission. • Persistent renal dysfunction = Final plasma creatinine value before hospital discharge ≥ 200% of the baseline plasma creatinine value in a patient not known to have received RRT prior to ICU admission.
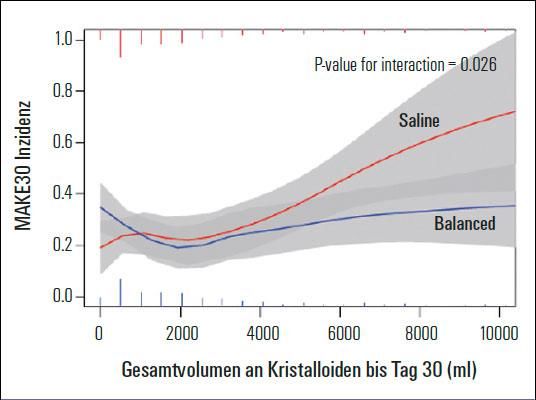
SMART - Balanced Crystalloids versus Saline in
Critically Ill Adults
15800 Patienten, NaCl0,9% vs. balanced solution
MAKE 30: Balanced crystalloid group:14.3% vs. saline group = 15.4%
(OR 0.91; 95% CI 0.84-0.99)
driven by mortality
NNT to avoid one MAKE 30 outcome is 94
Erhaltenes Volumen 1000ml (0-3300ml)
prespecified Subgruppenanalyse:
Sepsispatienten (NNT=20) und Patienten welche größere Mengen an
Flüssigkeit erhielten hatten einen größeren Benefit von balancierten
Lösungen
Semler MW NEJM 2018SALT-ED: Balanced Crystalloids versus Saline
in Noncritically Ill Adults
13347 Patienten, cross over trial, balanced solution vs. saline, unblinded,
Infusionsmenge: in Median 1079 ml
Prim. outcome kein Unterschied
MAKE30: balanced vs. saline: 4.7% vs. 5.6%; OR 0.82 (0.70-0.95 p=0.01)
NNT to avoid one MAKE30 =111
driven by AKI
Krea> 1,5mg/dl at admission: MAKE30: 28% vs. 37,6% (pAnother piece of un-physiology
0.9% saline resuscitation is associated with a higher need for vasopressor
therapy than a balanced crystalloid
n= 60, Infusionsmenge (beide Gruppen) = ca. 1700-4900ml (3300)
Normal saline versus a balanced crystalloid for
goal-directed perioperative fluid therapy in major
abdominal surgery: a double-blind randomised
controlled study. Pfortmüller CA British Journal of
Anaesthesia, 120 (2): 274e283 (2018)The SMART and SALT-ED trials are massive, multiple-crossover trials
which compare saline versus balanced crystalloids among critically ill
and non-critical patients. Both studies found a 1% increase in death or
renal failure with the use of saline.
The combination of physiology, animal studies, numerous RCTs,
SMART, and SALT-ED indicate that it's time to stop resuscitating with
saline.
Normal saline is only for metabolic alkalosis
Plasmalyte and RLA are less alkaline than Elomel isoton
https://emcrit.org/pulmcrit/smart/Chloride in ACID BASE
Kombinierte Störungen des SBHH Delta-Delta?
Chlorid: konstantes Verhältnis zu Na: Na-Cl = 36
Chlorid: inverses Verhältnis zu Bicarbonat: Na-Cl=HCO3 (+AG)
High Anion Gap Acidose:
Delta Bicarbonat – Delta AG = Na-Cl-36
>-6 = mixed high anion gap and normal anion gap metabolic acidosis
-6 to 6 = isolated high anion gap acidosis
>+ 6 = mixed high anion gap acidosis and metabolic alkalosis
Tsapenko, Oman medical journal 28.1 (2013): 73.Beispiel: Patient mit KADC BZ: 1368mg/dl, Na: 134 mmol/l, Cl 85 mmol/l, pH 7,31, HCO3: 13,4 mmol/l, pCO2: 27 mmHg PAG: 35,6 mmol/l – deltaAG: 23,6mmol/l deltaAG-deltaBic = 13 mmol/l Na-Cl -36= 134-(85+36)= 13mmol/l
Kidney meets Liver
Leber und Niere
CLF
Liver Decompensation mit/ohne
ALF Nierenversagen
Liver Decompensation
A-CLF
Type A
Type B
Type C
AKI-HRS AKI-non HRSAKI in Liver Failure
Davenport A Kidney Int 2017Serum copeptin at admission was significantly higher in patients with ACLF
compared with those without (33 (14–64) vs. 11 (4–26) pmol/L; p < 0.001)
Kerbert AJ Critical Care 2017Huelin P Clinical Gastroentereology and Hepatology 2017
547 akute Dekompensation
der Leberzirrhose
290 (53%) AKI 29% *acute on chronic
70% ACLF
AKIN 1 AKIN 2 AKIN 3
(n=197) (n=55) (n=38)
68% 19% 13%
Höhere Rate an Progression des AKIN
AKIN 1A AKIN 1B* Höhere Rate an NET
(n=58) (n=139) 90 day survival
Höhere Rate an ACLF
29% 71% Höheres Stadium ACLF AKIN 1A 84%
AKIN 1B 58%
AKIN 2 48%
renal recovery 90% renal recovery 50%
AKIN 3 43%Ist der Patient alt oder zu alt
für eine ICU?GOMIC´s- get out of my intensive care?
> 15% der ICU Patienten sind > 80 Jahre1
Hospital Mortality: 20% (vs. 13%)1
Frailty: erhöht das Mortalitätsrisiko (HR 1,54 CI1.38-1.73)2
Welcher ältere Patient soll auf die ICU?
Definierte Vorselektion von Patienten vs. übliche Prozedere:
61% vs. 34% Admission
Kein Einfluss auf Outcome – Hospital Mortality: 30 vs 20%3
1 Karakus A Intensive Care Medicine 2017
2 Flatten H Intensive Care Medicine 2017
3 Guidet B JAMA 2017Nutrition-News
Early goal-directed nutrition versus standard of care in adult intensive
care patients: The single-centre, randomised, outcome assessor-
blinded EAT-ICU trial.
Eine frühe, hochkalorische Ernährung ist obsolet.
Prof. W. Druml: Nutrition in ICU „early conservative – late liberal“
Allingstrup MJ Intensive Care Med 2017Pharmakinetic News
Caspofungin – keine Dosisanpassung bei CVVHD (Aguilar G CC 2017)
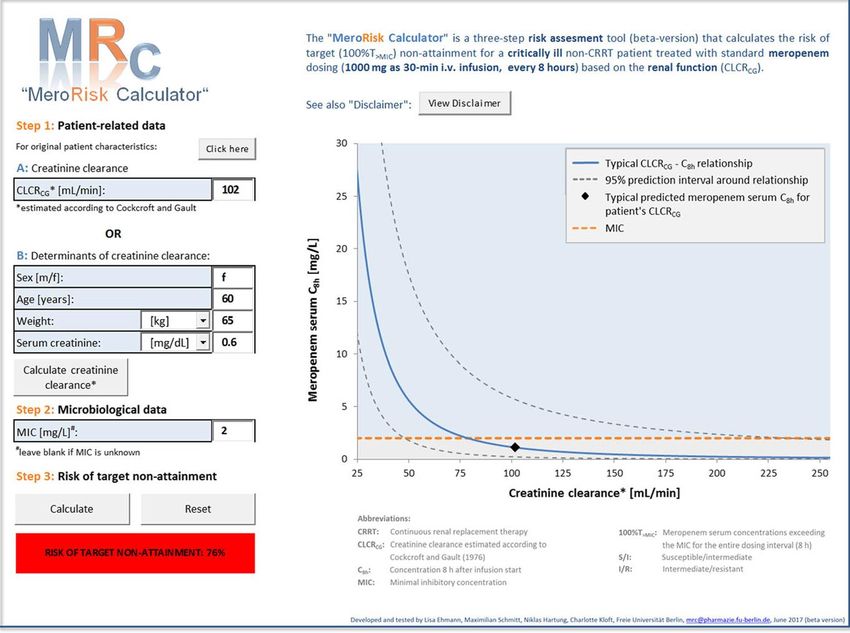
Meropenem: Bei Standarddosierung 3x1g i.v.:
100%T>MIC was 48.4% MIC values of 2 mg/L
100%T>MIC was 20.6% MIC values of 8 mg/L
Meropenemkonzentration steigt mit Reduktion der GFR.
Online Kalkulator zur Evaluierung wie hoch die Wahrscheinlichkeit ist,
das der behandelte Patient in Abhängigkeit von Nierenfunktion nicht im
Bereich der MIC liegt.
Ehmann L Crit Care 2017Ehmann L Crit Care 2017
You can also read