Waveform Capnography Application for the prehospital provider - Maika Dang, MD CMTE University of Washington EMS Fellow
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Waveform Capnography
Application for the
prehospital provider
Maika Dang, MD CMTE
University of Washington EMS Fellow
Maika Dang, MD, CMTE
University of Washington EMS Fellow
Overview • Carbon Dioxide • Waveform Capnography • Physiology and Pathophysiology

“CO2 is the smoke from the
flames of metabolism”
- Raymond Fowler, MD
“Capnos” = Greek for smoke
Carbon dioxide byproduct of cellular metabolism Glucose + O2 → CO2 + H20

Carbon dioxide diffuses
into the blood
• Bicarbonate – 70%
• Bound to hemoglobin – 20%
• Dissolved in blood – 10%
Carbon dioxide is eliminated through the lungs

The Evolution of CO2 Detection Colorimetric Capnometry Capnography
Capnography • Continuous numerical and waveform measurement of exhaled CO2 concentration

[CO2]
Lets Get Oriented
ECG TRACING O2 SAT
CO2 QUANTITY CO2 TRACINGCapnography is not just for the ALS provider
Capnography
Most sensitive
for detecting
hypoventilation
Emergency Department
Airway Monitoring
AMS
Procedural Sedation
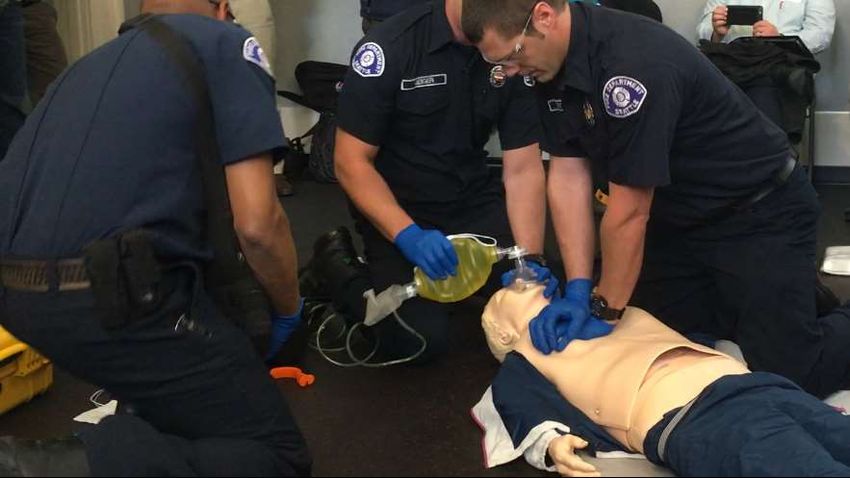
EtCO2 >>> RR or O2 sat…Let’s talk bagging
EtCO2
Two Hand
Technique
Effective BaggingEffective Bagging
Two person bagging better than one
• Jaw Thrust
• Face into the mask
• Light downward pressure with thumbs
• Bring face into mask with upward pressureEtCO2 • Quality of the mask seal • Current ventilator status • Potential EtCO2 target
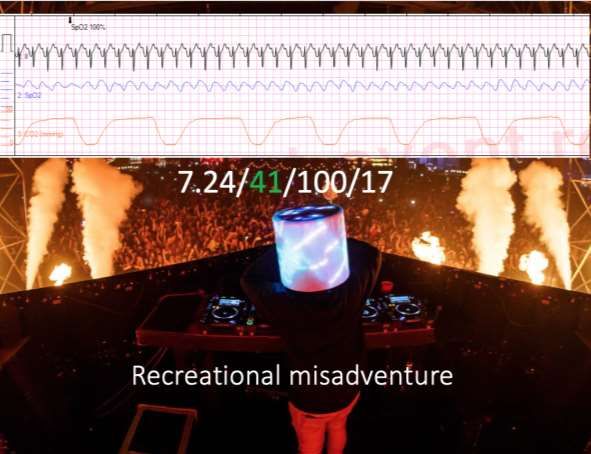
22 yo male reportedly took MDMA found seizing and hyperthermic
Requiring airway management
EXAMPLE USING EtCO2 with BVMPrior to intubation
End tidal ~ 25Intubation
Approximately 45 seconds no ventilations during intubation
End tidal ~ 70Arrival to hospital What do you think of this patient’s metabolic state? How to you want to ventilate this patient?
Lets do a case… • 34 yo male polysubstance overdose with respiratory depression. • RSI - ketamine & rocuronium
The Second
Attempt
• Second pass attempt a success!
• What is happening here?Cuff leak or hypopharyngeal ETT
Waveform prior inflating balloonRebreathing
Return of spontaneous respirations
Curare CleftThe sixth vital sign
EtCO2 25 mmHg DKA Sepsis
What is going on here?
Case of difficulty breathingBronchospasm
Changes with treatment
PaCO2 – EtCO2 gadient When the end tidal reading does not accurately reflect the arterial CO2
Normal PaCO2 – EtCO2 gradient is within 5 mmHg
EtCO2 accurately
reflects PaCO2 when
Normal perfusion state
(delivery)
AND
Normal ventilatory state
(gas exchange)This gradient is
invariable
positive
PaCO2 ≥ EtCO2The CO2 Gradient is determined at the level of the alveoli Atelectasis PE Mucus plug Reduced CO Pulmonary edema Shock Pneumonia Cardiac arrest Mainstem ETT ETC… ETC…
For example…
50 yo male s/p total knee arthroplasty 1 week c/o of shortness of breath, chest and
leg pain with swelling.
• HR 125
• BP 110/80
• RR 22
• O2 88% RA
And
as your are collecting his history he arrests in front of you…Post Intubation Initial EtCO2 10
Transported to emergency department with ongoing CPR
After 50 minutes of resuscitation
EtCO2 5-10
However, ABG pH 6.9 and PaCO2 135✓ Verification of ETT ✓ Visualization of ventilations ✓ Quality of chest compressions ✓ ROSC ✓ Prognostication
Ventricular Fibrillation
End tidal ~ 20-25
What do you do with this?Bring the lightning!
ROSC
End tidal ~ 50 (EtCO2 25 prior to defibrillation)
EtCO2 rise > 10 mmHg specific but not sensitive for ROSC
LOOK FOR TRENDSBicarb administration
Don’t be fooled…EtCO2 50
EtCO2 30
EtCO2 20
EtCO2 10
Another case with ROSC!Termination of resuscitation
EtCO2 ≤ 10 mmHg after 20 mins 100% mortality
”ACLS is for dentist”Last case: A fender bender…
Polytrauma + TBI = bad day
22 yo male MVC. Unresponsive, initial GCS 3 sluggish pupils.
Large hematoma right temple with bruising to chest and
abdomen and a right closed femur deformity.
Intubate with ketamine and rocuronium
• HR 125
• BP 90/60
• O2 95% BVM w/ RR 18 at 100 FiO2
How are you going to ventilate your patient if?
1. EtCO2 70
2. EtCO2 20CO2
&
Cerebral Blood FlowTrauma PaCO2-EtCO2 gradient
EtCO2 accurately
reflects PaCO2 when
Normal perfusion state
(delivery)
AND
Normal ventilatory state
(gas exchange)Polytrauma with TBI
How are you going to ventilate your patient if?
1. EtCO2 70
2. EtCO2 20
If EtCO2 is high → target eucapnia
If EtCO2 is low → “Let it go”Summary
Ventilation
Waveform capnography Perfusion
reflects Metabolism
Use it to guide ventilations
Waveform capnography Recognize common waveforms
is the 6th vital sign Guide therapeutics
Diagnostic utility
Understand the PaCO2-EtCO2 gradient and
how to apply to your patientReferences
• Abramo TJ, Wiebe RA, Scott S, Goto CS, McIntire DD. Noninvasive capnometry monitoring for respiratory status during pediatric seizures. Crit Care Med 1997;25:1242–6.
• Eberle, B., et al. “Checking the Carotid Pulse Check: Diagnostic Accuracy of First Responders in Patients with and without a Pulse.” Resuscitation, vol. 33, no. 2, 1996, pp. 107–116.,
doi:10.1016/s0300-9572(96)01016-7.
• Hunter CL, Silvestri S, Ralls G, et al. A prehospital screening tool utilizing end-tidal carbon dioxide predicts sepsis and severe sepsis. Am J Emerg Med 2016; 34:813.
• Kolar, M., Krizmaric, M., Klemen, P., and Grmec, S. Partial pressure of end-tidal carbon dioxide successful predicts cardiopulmonary resuscitation in the field: a prospective observational study. Crit
Care. 2008; 12: R115
• Levine, R.L., Wayne, M.A., and Miller, C.C. End-tidal carbon dioxide and outcome of out-of-hospital cardiac arrest. N Engl J Med. 1997; 337: 301–306
• Lee, Sung-Woo, et al. “Concordance of End-Tidal Carbon Dioxide and Arterial Carbon Dioxide in Severe Traumatic Brain Injury.” The Journal of Trauma: Injury, Infection, and Critical Care, vol. 67, no.
3, 2009, pp. 526–530., doi:10.1097/ta.0b013e3181866432.
• Mishra, Lal Dhar. “Cerebral Blood Flow and Anaesthesia : a Review.” (2005).
• Solmeinpur H, et al. Predictive Value of Capnography for Diagnosis in Patients with Suspected Diabetic Ketoacidosis in the Emergency Department. West J Emerg Med 2013;
(www.escholarship.org/uc/item/5qz744fv).
• Tat LC, Ming PK, Leung TK. Abrupt rise of end tidal carbon dioxide level was a specific but non sensitive marker of return of spontaneous circulation in patient with out-of-hospital cardiac arrest.
Resuscitation. 2016; 104:53–58.
• Tibballs, J., and P. Russell. “Reliability of Pulse Palpation by Healthcare Personnel to Diagnose Paediatric Cardiac Arrest.” Resuscitation, vol. 77, 2008, doi:10.1016/j.resuscitation.2008.03.098.You can also read