ALL THINGS DERMATOLOGY - Dr Aravind Chandran Dermatologist
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ALL THINGS
DERMATOLOGY
Dr Aravind Chandran
Dermatologist
Auckland District Health Board and Skin Specialist Centre
Honorary Lecturer
University of Auckland
∧
ALL THINGS
DERMATOLOGY
PITFALLS & PRACTICAL TIPS
Dr Aravind Chandran
Dermatologist
Auckland District Health Board and Skin Specialist Centre
Honorary Lecturer
University of Auckland
Outline ■ Pitfalls and practical tips in managing skin conditions Use of Steroids Liquid Nitrogen/Cryotherapy Diagnosing Pigmented lesions Clinical Photography
Steroids in dermatology

Steroids in dermatology – Topical ■ Formulations – ointment , cream, lotions, gel, foam ■ Combinations : antifungals, antimicrobial, antibacterial ■ Compounded – Oral ■ “Standard” course ■ Slow taper ■ Mini-pulse – Intra-lesional – Intramuscular – Intravenous

Topical Steroids in Dermatology ■ “Pillar” of skin therapeutics – Ease of use – Less systemic effects – Safe in pregnancy ( class I –III) ■ Potency and steroid step ladder

Topical Steroids - Pitfalls
■ Suboptimal medication use
– Wrong potency –
■ scalp vs vs hands and feet vs face vs body vs flexures
– Improper formulation
■ Insufficient dosage
– Steroid phobia – patient and practitioner
– Under use more common than overuse
■ Lack of patient adherence as a result of inadequate patient education or adverse drug
events
■ The use of combination steroid/antifungal formulations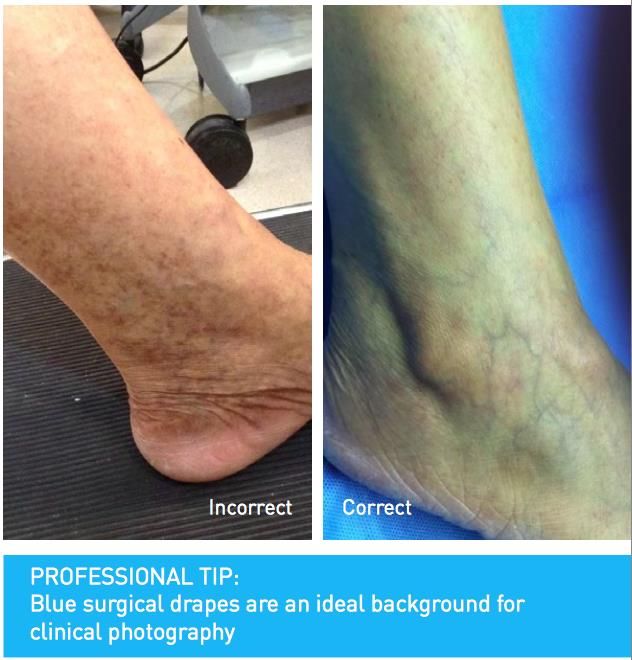
Topical Steroids
■ Practical Tips:
– Familiarize topical steroids potencies
– Finger tip units FTU
– Consider formulation
■ Location
■ weeping?
■ Contact sensitivity
– Occlusion
– Wet wraps
– Tachyphylaxis
– “Weekend” therapy - for prevention frequent flares
– Patient education, written plans, information leaflets
ORAL Steroids
■ Used for inflammatory skin disease
– Often over prescribed
■ Long-term use associated with significant side effects
■ PITFALLS
– No formal diagnosis
– Repeated course – short and sharp
– Lack of bone protection and immunization in longer term use
■ TIPS:
- Establish a diagnosis before committing to treatment course
- Slower taper and supplementing with potent topical to prevent rebound
- Plan for early switch to steroid sparing agents
- AVOID in psoriasis – may de-stabilise and result in erythroderma or pustular
psoriasis
- Medical alert bracelets
- Bone protection
Intramuscular steroids
■ Under utilised
■ IM vs PO steroids
– Equally effective
– Better compliance especially with need for long tapering doses
■ Greater efficacy and safety
– Lower total dose when used long-term – fewer side effects
– Adverse effects (as per oral ) PLUS
■ IM can result in lipoatrophy at injection site
■ Dysmenorrhea in femalesLIQUID NTROGEN CRYOTHERAPY
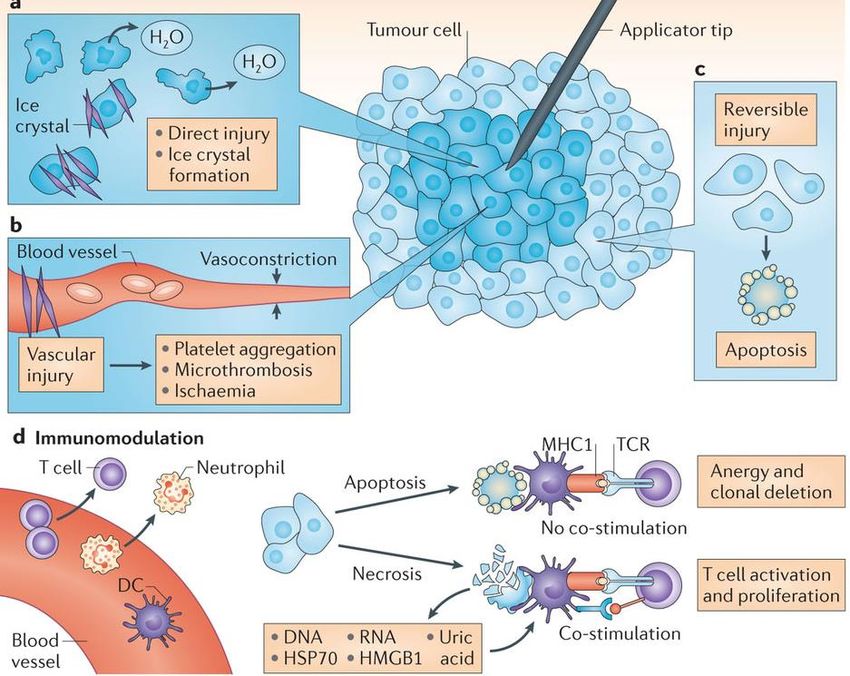
LN - Cryotherapy ■ Effective, simple and inexpensive treatment ■ Suitable for outpatient setting and poor surgical candidates ■ most commonly used – actinic keratoses – warts, molluscum – benign, premalignant lesions – malignant (superficial) lesions ■ Destruction of benign lesions requires temperatures of −20°C to −30°C ■ Effective removal of malignant tissue often requires temperatures of −40°C to −50°C.
Mechanism of action
Cryotherapy - PITFALLS ■ Treating undiagnosed lesions – Avoid in pigmented lesions – If unsure biopsy first ■ Do not treat thickened or raised lesion ■ Under treating malignant lesions ■ Poor cosmetic results in exposed sites ■ Single/long cycles – Swelling, blistering, ulceration ■ Caution on special sites: – Pretibial lesions – prone to ulceration – Eyelids- swelling, haemorrhage – Hair-bearing skin – may result in scarring and alopecia
CRYOTHERAPY- TIPS
Medscape image
– Cone tip
■ Reduces contamination and
focuses treatment
– Feathering at edged to avoid abrupt
cut off
– Overlapping treatment areas for large
areas
– De-bulking hyperkeratotic areas
– Use nozzles and attachments
– In malignant lesion
■ Draw a margin
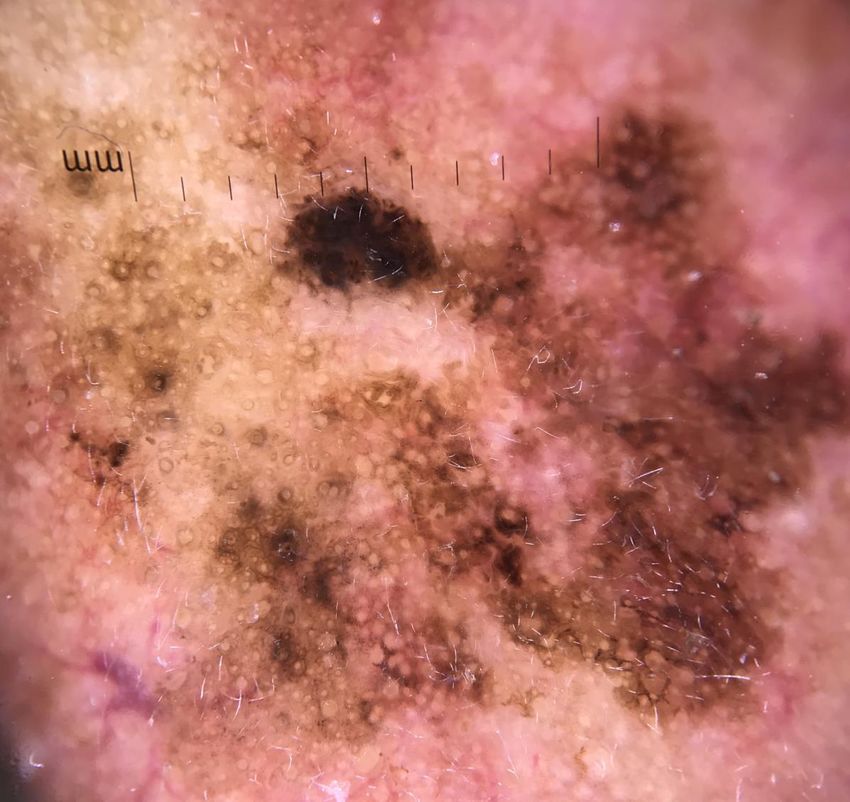
■ Repeated ‘freeze – thaw’ cyclesPIGMENTED LESIONS -
DIAGNOSISBiopsy of pigmented skin lesions
■ 2010 NZMA Audit by Rademaker et al
■ 37% of cases referred had no useful clinical information
■ OUTPUT results = INPUT of information provided
■ 40% of lesions where a melanoma was considered, and 32.5% of lesions identified as pigmented
lesions, were punch biopsied
■ 2470 patients with melanoma, punch and shave biopsy significantly increased the odds of
misdiagnosis by 16.6- and 2.6-fold respectively, compared to excisional biopsy. Punch biopsy
increased the risk of a misdiagnosis with adverse outcome by 20-fold (p < 0.001).
■ Smaller the percentage of lesion removed by biopsy, the greater the degree of inaccuracy was
likely to occur
■ Whole lesion if possible
■ Serial punch or representative incisional bx – not single punch biopsyCLINICAL PHOTOGRAPHY
Clinical Photography ■ Documentation – rash, lesions, cosmetic procedures ■ Treatment progress ■ Monitoring/Self observation with “selfies” ■ Professional development/learning ■ Medico-legal ■ Referrals ■ Tele-dermatology opinions
Pitfalls and TIPS ■ Consents – informed consent - verbal or written ■ Patient identification or de-identification in with facial photos ■ Lesion observation Macro +/- Dermoscopy (not ONLY dermoscopic images) – Location/distribution shot – waist up/down/front back/arms and legs – Close-up macro – Dermoscopy if available ■ Taking the photograph – Get to know your equipment – Composition ■ Storage and handling of images – patient privacy
Lighting
©AppwoRxPOSITIONING
©AppwoRxBACKGROUND
©AppwoRxClinical Photography apps ■ Picsafe ■ Epitomyze capture ■ Rx Photo
END enquiry@skinspecialistcentre.co.nz
You can also read