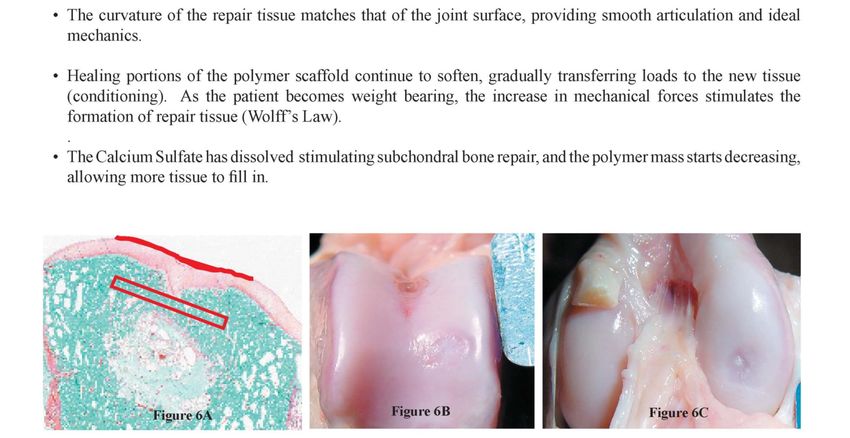
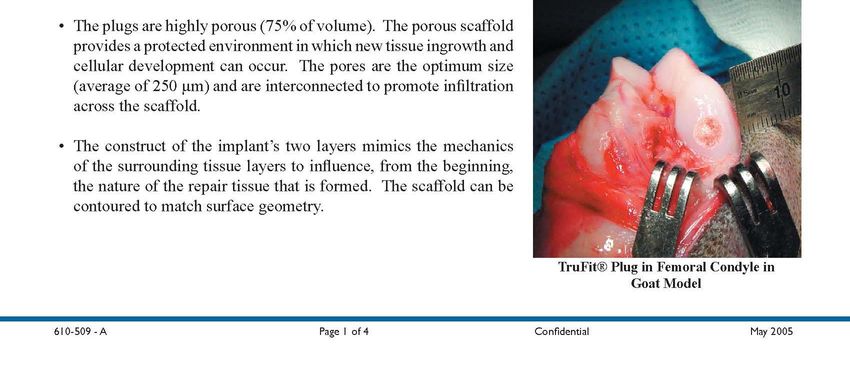
Cartilage Restoration of the Knee Gregory A. Woods, MD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cartilage Restoration of the Knee
Gregory A. Woods, MD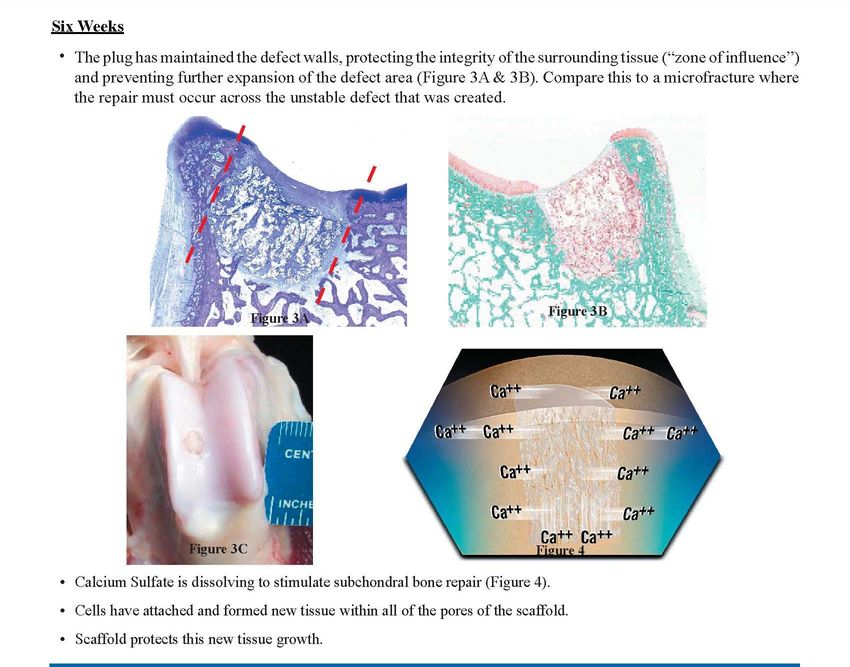
I have no financial interests, relationships, or potential conflicts of interest relative to this presentation
Jayhawk Doc
Team • We use a team
approach to care
of our athletes.
• Athletic trainers,
physicians,
physician
assistants,
physical
therapists,
occupational
therapists,
coaches.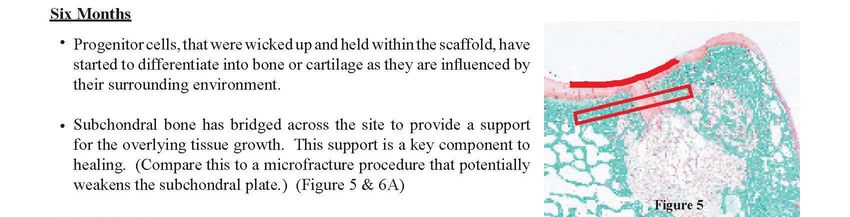
History of a twisting injury while playing basketball. C/O pain, swelling, and instability PE- guarded Lachman, pain medially and laterally, +McMurray’s
Case 2- 41 y/o Male
• X-ray showed
Case 2- 41 y/o Male
• MRI Showed
Case 2- 41 year old Male
Articular replacement
– Biological
• OATS-Ostoarticular Transfer
• OBI plugs
• ACI- Autologous Chondrocyte Implantation
• Microfracture/drilling
• Allograft- Fresh Frozen Osteoarticular
– Nonbiological-
• Focal replacement- Arthrosurface
• Compartmental replacement
– Oxford Mobile bearing Unicompartmental- medial
– Fixed bearing- lateral compartment
– Patellofemoral replacement
• Total Knee Replacement- TKRCase 2- 41 y/o male Problem: Femoral Articular Defect that is 1-2 cm2 in size Therapeutic Primary Options: – Debridement – Microfracture – Osteochondral Grafting – Autologous Chondrocyte Implantation – OBI plug
Osteochondral defect treatment
options Size 1-2 cm2
Debridement
– Advantages
• Cheap
• Quicker Rehab
• Decreases mechanical symptoms
• Decreases debris load into the joint
– Disadvantages
• Does not replace or repair the defect
• Poor load characteristics• Microfracture
– Mesenchymal Stem Cell stimulation
for repair
– Creates holes in the cortical bone
for marrow stimulation of repair of
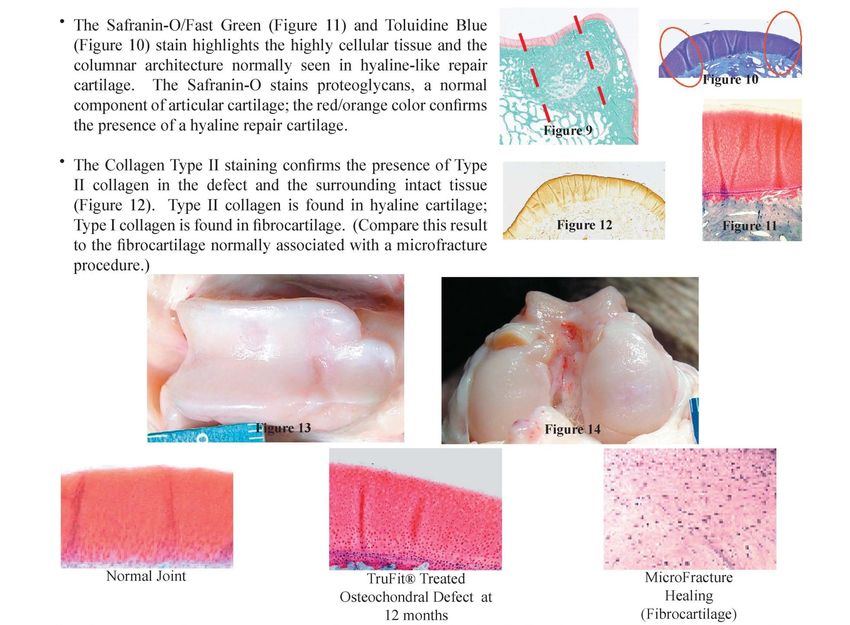
the defect.Microfracture
– Advantages
• Cheap
• Low complication rate
• Results-Steadman best results -80% better
– Range from 60%- 86% Improved symptoms
– Disadvantages
• Increased Rehab time (limited WB 4-6 weeks)
• Results probable won’t hold up over time
• “Repair” cartilage is mainly fibrocartilageOsteochondral defect treatment options Size 1-2 cm2
Osteochondral Grafting: Autologous
– Move a plug of Cartilage and bone from one area
of the knee to the damaged area.
– Multiple plugs→ mosaicplastyOsteochondral defect treatment options Size 1-2 cm2
Osteochondral grafting- OATS
– Advantages
• Cheap
• Can be done arthroscopically most of the time
• Only surgery that restores the height and shape of articulating
surface along with the composite autologous material
• Results better than Microfracture- 80- 100% G/E
– Disadvantages
• Limited in size due to limited number of host plugs
• Rob Peter to pay Paul
• Mismatch of cartilage curvature and thickness (especially when
grafting the patella)
• 4-6 weeks limited WB
• Cannot graft the tibiaOsteochondral defect treatment
options Size 1-2 cm2
Autologous Chondrocyte Implantation (ACI)
– Scope knee and harvest Cartilage
– Grow the cartilage in a lab (in vitro)
– Second operation to implant the cartilage using a
periosteal flapAutologous Chondrocyte Implantation (ACI)
Osteochondral defect treatment options Size 1-2 cm2
Autologous Chondrocyte Implantation (ACI)
– Advantages
• Do not have to rob Peter – much.
• Good long term results- 65%- 86% G/E
– Disadvantages
• Very Expensive (Total $15-25,000)
• Two operations
• Does not replace with 3 dimensional scaffold
• Protected WB for 6-12 weeks
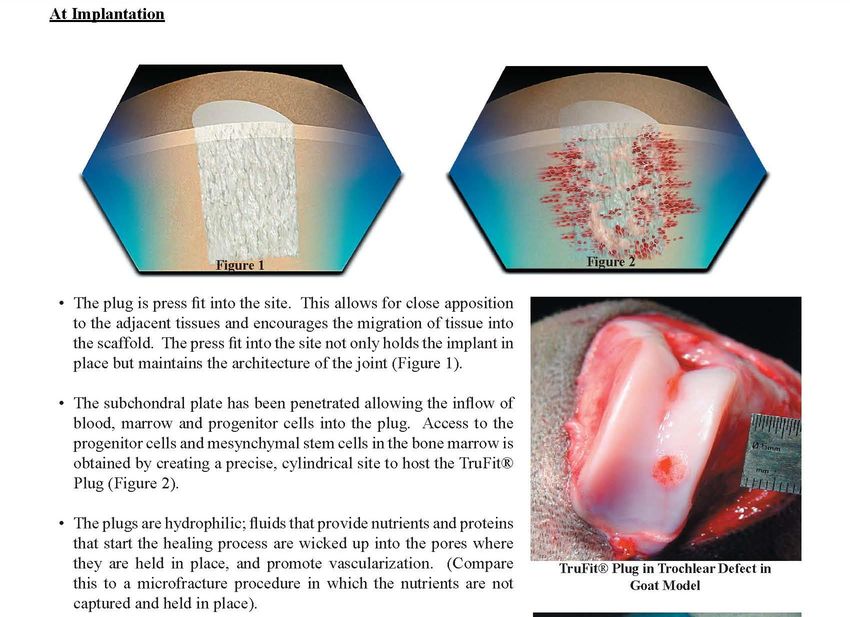
• Open procedureMarrow Stimulation- OBI plug Scaffold of PGA/ PLA and Calcium Triphophate Available in preshaped diameter plugs that can be cut to custom length Provides 3 dimensional scaffold that for marrow stimulation repair High tech microfracture technique
OBI plugs
OBI Plugs
OBI Plugs
OBI Plugs
OBI Plugs
OBI Plugs
OBI Plugs FDA has approved the use of OBI plugs as a bone void filler only This is an off label use/indication for this device.
Future of Mesenchymal Stem Cell Stimulation Microfracture enhanced with BMP-7 OBI plugs – Plus ACI – Plus PRP (Platelet Rich Plasma) – Plus OP1/BMP7 ACI plus Scaffolds – Hyaluronic acid Hyalograft – PLA/PGA Fleece – Collagen MACI
Future is partly here. MACI procedure. Matrix Autologous Chondrocyte Implantation 1. Cartilage Biopsy
Description of MACI
MACI, autologous cultured chondrocytes on porcine collagen membrane,
is a cellular sheet that consists of autologous chondrocytes seeded on a 3 x 5
cm, resorbable porcine Type I/III collagen membrane, for implantation into
cartilage defects of the knee.
The active ingredients of MACI are the autologous cultured chondrocytes
and porcine Type I/III collagen. The autologous chondrocytes are propagated
in cell culture and are seeded on the collagen at a density of 500,000 to
1,000,000 cells per cm2. The final MACI implant contains at least 500,000
cells per cm2 and does not contain any preservative.Biopsy Transport Medium Bottle→Ship to Vericel
MACI IMPLANTATION
Epinephrine 1cc—1:1000 Vial
Neurosurgical Patties (Spinal, 1/2” Square)
Fibrin Sealant
6-0 VicrylR Suture on P1 Cutting Needle
Sterile Intermediary Dishes (2)
Ink Marker (Sterile) and Ruler (Sterile)Alternate technique Ring (4.5 mm and 6 mm) or Spoon Curette No. 15 Surgical Scalpel Toothless Adsons (2) Fine Dissecting Scissors Sterile Paper or Foil (from surgical gloves or suture packaging) Epinephrine 1cc—1:1000 Vial Neurosurgical Patties (Spinal, 1/2” Square) Fibrin Sealant 6-0 VicrylR Suture on P1 Cutting Needle Sterile Intermediary Dishes (2) Ink Marker (Sterile) and Ruler (Sterile)
THE MACI IMPLANT is available as a cellular sheet, 3 x 5 cm, with a 0.5-cm2 section removed from the lower left-hand corner, consisting of autologous cultured chondrocytes on a resorbable Type I/III collagen membrane at a density of at least 500,000 cells per cm2.
Preparation of defect
Applying fibrin sealant to the bone bed for fixation of the MACI implant
The MACI implant should be implanted with the cell-side facing the subchondral bone. The cell seeded side has the rougher texture
The MACI implant should completely fill the defect
Close wound in standard fashion. The use of an intraarticular drain is not recommended because it may damage the implant. Intra-articular injections of any type are also not recommended.
Post op care- recommended • Wrap knee in soft, supportive dressing. • Fit patient with knee immobilizer and set at 0° flexion for the first 12 to 24 hours. • Cryotherapy may be administered. • Begin continuous passive motion (CPM) within 12 to 24 hours following implantation surgery. (I rarely use it!) • Range of motion (ROM) control brace (initially set at 0°–30° of knee flexion) should be worn 24 hours per day for the first 3 weeks. • Weightbearing depends on location of the defect.
Rehabilitation No high impact or cutting twisting sports for 6-9 months. I recommend a year for full return. Long term results better than microfracture.
The pain relief held in longer term followup
KOOS Pain and Function (SRA) Scores in the 3-Year
Extension Study
Visit MACI Microfx
N Pain Function N Pain Function
Baseline 65/65 37.1 15.4 63/63 35.2 11.9
2 years 63/63 82.2 60.5 60/60 71.8 48.9
5 years 65/64 82.2 61.3 59/59 74.8 50.3Thank You ! Gregory.Woods @nghs.com
You can also read