Improving the quality and reproducibility of diagnostic assays - Clare Morris Division of Infectious Disease Diagnostics, NIBSC, UK - 4 All Of Us
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Improving the quality and
reproducibility of diagnostic assays
Clare Morris
Division of Infectious Disease Diagnostics, NIBSC, UK
The National Institute for Biological Standards and
Control (NIBSC)
• Assure the quality of biological
medicines worldwide; developing
standards and reference materials,
testing medicinal products and
carrying out regulatory research
• Centre within the Medicines and
Healthcare Products Regulatory
Agency (MHRA), which is an
executive agency of the Department
of Health and Social Care (DHSC)
• https://www.nibsc.org/
2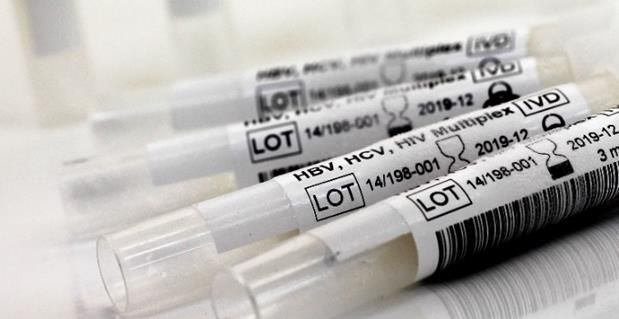
What are we trying to achieve?
Accurate measurement
More robust and reproducible diagnostic assays
Improved health – prevention and clinical
management
3
How can we achieve this?
External Quality
Assurance
Clinical and other
materials
Regular Panels
Quality System External Evaluation of External Quality
results Controls
Training
Competence Continual monitoring
Management Trend Analysis
Facilities Westgaard Rules
Biological
Clinically Standardisation
Validated Assay Diagnostic Common External
Validation Panels
Clinical Sensitivity and Test Result Calibrator
Relative potency
Specificity
Int’l Units (IU’s)
4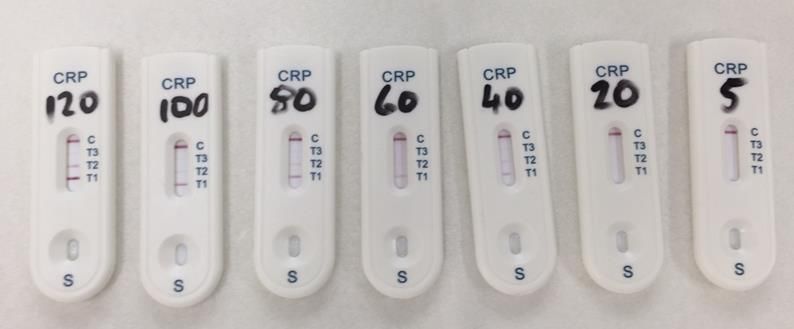
How can we achieve this?
External Quality
Assurance
Clinical and other
materials
Regular Panels
Quality System External Evaluation of External Quality
results Controls
Training
Competence Continual monitoring
Management Trend Analysis
Facilities Westgaard Rules
Biological
Clinically Standardisation
Validated Assay Diagnostic Common External
Validation Panels
Clinical Sensitivity and Test Result Calibrator
Relative potency
Specificity
Int’l Units (IU’s)
5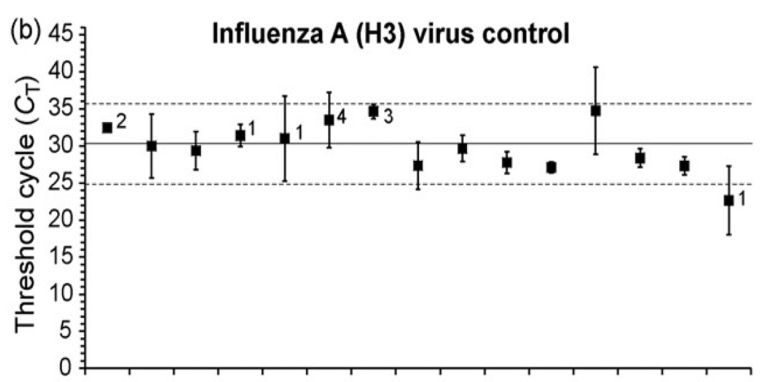
Internal (Kit) QC vs External QC
Internal (Kit) Controls External quality Controls
Included in kit/assay Supplied independent of kit/assay
Optimised for specific assay Suitable for range of assays
Wide acceptance range, may Acceptance range is defined and
change between batches fixed between batches
Poor for highlighting subtle changes Optimised for detecting small
in assay performance (strong +ve) changes and/or go/no-go criteria
Does not allow comparison between Allows comparison between different
different assay kits or platforms kits or assay platforms
Changes with kit batches Consistent between kit batches
Provides assurance on each specific Enables intra-lab and inter-lab
assay performance to be assessed
6
What are External QC Reagents?
• Tested in addition to patient samples
and kit controls
• Similar to defined analyte
• High quality and well characterised
• Confers confidence in assay
performance (chemical, physical or
biological)
➢ Provides assurance in the output of
each assay
7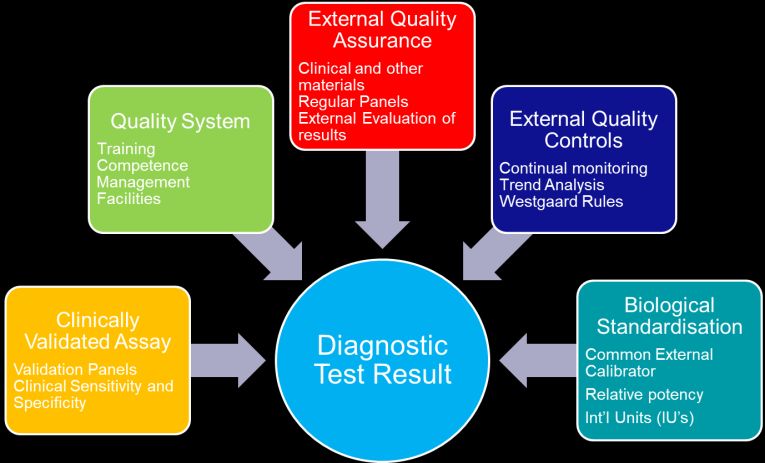
EQC in action – Norovirus study, 2008
• NIBSC prepared a large batch of Norovirus and aliquoted material. Each tube
contained identical sample
• Tubes shipped to 21 UK labs offering clinical diagnostic test for Norovirus
• Labs returned data to NIBSC for analysis
➢ What happened next?
8
Inter-lab comparisons 9
Inter-lab comparisons
Some assays don’t
detect this sample
10Inter-lab comparisons
Labs with excellent reproducibility
but give different values.
Which one is correct?
11Inter-lab comparisons
Intra laboratory reproducibility
varies between labs
12Inter-lab comparisons - Norovirus controls,
2016
13Assuring the Quality of Diagnosis
External Quality
Assurance
Clinical and other
materials
Regular Panels
Quality System External Evaluation of External Quality
results Controls
Training
Competence Continual monitoring
Management Trend Analysis
Facilities Westgaard Rules
Biological
Clinically Standardisation
Validated Assay Diagnostic Common External
Validation Panels
Clinical Sensitivity and Test Result Calibrator
Relative potency
Specificity
Int’l Units (IU’s)
14Hierarchy of standards
WHO International standard (higher order,
international conventional calibrator)
Traceability
Secondary Standard (calibrator for assays and
tertiary standards)
Tertiary Standard (working reagent, Kit
control, run control)
Uncertainty of
measurement
15Standardisation
When numbers are important
Comparing data between labs using CMV EQC
• EQC’s inform reproducibility
• EQC’s cannot confirm value
• E.g. CMV load in transplant
recipients
16Are all tests equal?
A need for standardisation
Over quantification - immunosupressant reduced too soon
Under quantification - organ damage - potential graft rejection
BK virus viral load estimate in copies/mL
17WHO International Standards
Highest order of reference for biological materials medicines
Allows direct comparison between different assays and methodologies
Quantify “relative potency” in a specific but arbitrarily defined International
Unit (IU)
Control all steps of the assay
Behave in similar way to clinical material
Stable over many years
Are quantified in International Units (IU’s) assigned following a multicentre
collaborative study using multiple assays
Intended for calibration of secondary references
18Anyone for coffee?
19.95 francs 498 pesetas 5730 lira 5.70 marks
Which coffee is the most expensive?
193 Euro 20
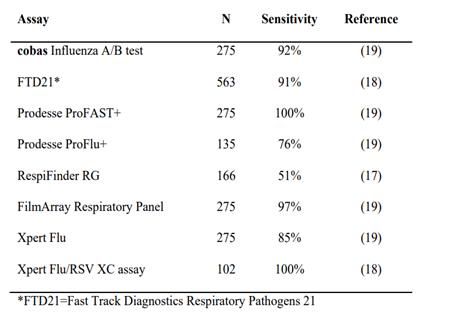
Current work – Influenza detection
• Influenza NAT diagnostics
• Classical molecular detection
• Point of care testing
• Do the numbers matter?
– Sensitivity
– Flu pos/Flu neg
– Really?
21• Assays are reported to be capable of detecting
both type A and B with equivalent sensitivity.
Inter-laboratory variability
• However data returned through EQA schemes
indicates that there is a large degree of variation
across all assays
Mean 2SD
Numbers adjacent to ■ indicate the number of negative results
• The use of molecular assays is becoming
increasing more frequently in the determination
of a respiratory illness being caused by influenza
in particular the use of rapid/POC assays. Intra-laboratory
variability
Individual laboratory datasets
22Current work- point of care testing for CRP
• 3 mg/L and 10 mg/L - mildly elevated
- diabetes, hypertension, or lifestyle
factors but not infection
• 10 mg/L and 100 mg/L are
moderately elevated significant
inflammation from an infectious or
non-infectious cause.
• Levels above 100 mg/L are severely
elevated and almost always a sign of
severe bacterial infection.
23• POC tests for CRP being trialled in pharmacies, GP surgeries
• Outcome reliant on accuracy of assay
• International Standard for CRP produced in 1985
• Clearly not produced for this assay type
• Developing a study to understand suitability of this material in
POC tests.
clare.morris@nibsc.org
24Concluding Comments
EQC reagents:
• part of framework of assurance
• critical role for comparability of results
“through time and space”
• essential tools for harmonising
performance of diagnostic assays
• help to deliver the right results that
lead to better patient care
25Acknowledgements
Jacqueline Fryer
Sheila Govind
Graham Prescott
Rehan Minhas
Claire Ham
Rob Anderson
Cristina
Neil Almond
Global study participantsYou can also read