Diabetes mellitus Typ 2: Die Rolle der SGLT-2 Hemmer - Harald Sourij, Graz
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diabetes mellitus Typ 2:
Die Rolle der SGLT-2 Hemmer
Harald Sourij, Graz
Neue Substanzen bei Typ 2 Diabetes mellitus
DPP-4 SGLT2
inhibitors inhibitors
ß Older T2D agents Newer T2D agents à
1950 1960 1970 1980 1990 2000 2010 2012 2013 2018
GLP-1 receptor
agonists
Lente class Recombinant
of insulins human insulin Insulin
produced produced degludec
SUs first used Insulin glargine
2nd-generation available2
SUs available
Metformin
introduced Three new classes:
α-glucosidase
inhibitors, meglitinides
and TZDs
Adapted from Kirby1
DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1; SGLT2, sodium–glucose transporter 2; SU, sulphonylurea; TZD, thiazolidinedione.
1. Kirby. Br J Diabetes Vasc Dis 2012;12:315–20. 2. Lantus® SPC.
Pathophysiologie des Typ 2 Diabetes mellitus
Reduzierter Inkretineffekt
Betazelldysfunktion GLP1 Gesteigerte
DPP4i Lipolyse
TZDs
Islet β-cell
GLP1 TZDs
DPP4i
(SFU)
Gesteigerte
GLP1 Glukose-
Islet α-cell
DPP4i reabsoption
HYPERGLYKÄMIE
Erhöhte SGLT2i
Glukagon-
sekretion
TZDs
GLP1 GLP1 TZDs
Metformin GLP1
DPP4i Reduzierte
Erhöhte hepatische Glukoseaufnahme
Glukoseproduktion
Neurotransmitter-
dysfunktion
Adapted from DeFronzo RA. Diabetes 2009;58:773–95. ÓWolters Kluwer Health
SGLT2 Hemmer
SGLT2
Glukose
S1 Segment
des proximalen
Tubulus
Distales Sammelrohr
~90% Reabsorption Segment
SGLT1
des proximal
~10% Reabsorption Tubulus
Keine Glucose
Chao EC et al. Nat Rev Drug Discov. 2010;9:551–559.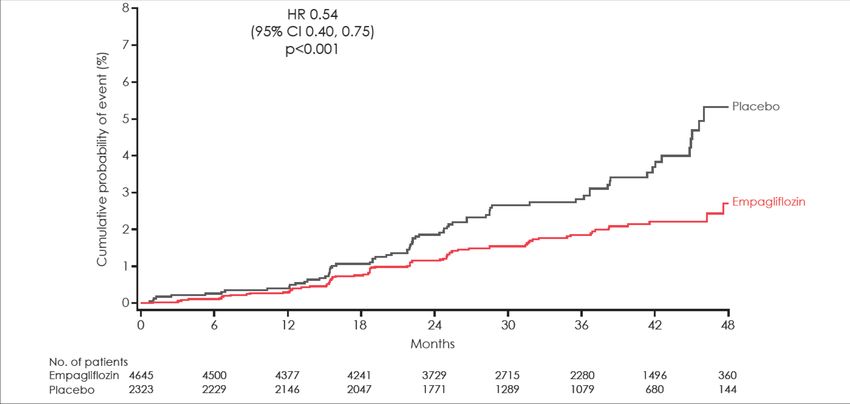
SGLT2 Hemmer
SGLT2
Glukose
S1 Segment
des proximalen
Tubulus
Distales Sammelrohr
~90% Reabsorption Segment
SGLT1
des proximal
~10% Reabsorption Tubulus
ca. 80 g Glukose
pro Tag
Chao EC et al. Nat Rev Drug Discov. 2010;9:551–559. Heise T et al. Diabetes, Obesity and Metabolism 2013;15:613-621
Phlorizin
Natürlich vorkommend in der Rinde von Birnen-, Apfel-, Kirschen- und anderen Bäumen
Kompetitiver Hemmer von SGLT-1 und SGLT-2
Zuckersenkender Effekt bereits 1987 erkannt
Substanzen im Überblick
EC50 (nM) Selektivität SGLT2 vs.
SGLT1
Sotagliflozin 1,4-1,8 20
Canagliflozin 2,2-2,7 260-414
Sotagliflozin
Dapagliflozin 1,1-1,3 610-1200
Ertugliflozin 0,9-1,4 1300-2300
Empagliflozin 3,1-3,6 1100-2700
EC50 half maximal effective concentration
Washburn & Poucher Expert Opin. Investig. Drugs 2013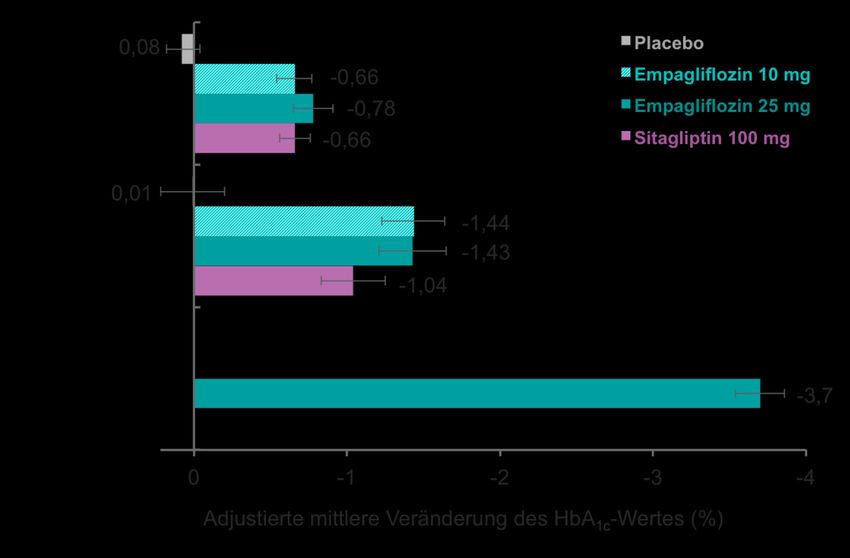
HbA1c-Senkung
Vertis Mono: HbA1c Senkung nach 52 Wochen
0,4 Zugabe von Metformin
(in Placebogruppe)
0,2 Placebo/Metformin
Änderung des HbA1c, %
ERTU 5 mg
0,0 ERTU 15 mg
(LS mean ± SE)
–0,2
–0,4
–0,6
–0,8
–0,9%
–1,0 –1,0%
–1,0%
–1,2
6 12 18 26 39 52
Studienbeginn
Wochen
Angepasst von Aronson R et al. Diabetes Obes Metab. 2018;20:1453–1460.; ; Storgard H et al. PlosOne 2016
Blutzuckersenkung je nach HbA1c Ausgangswert
Patienten, n
228
Ausgangs-HbA1c 224 *
ø 7,9 % 224 *
223 *
51
Ausgangs-HbA1c 54
*#
≥ 8,5 % 45 * *p
Körpergewichtsreduktion
Körpergewicht
Netzwerkmetaanalyse
0,0
Veränderung des Körpergewichtb ggü.
Studienbeginn, LS-Mittelwerte, kg
94,2 94,0 90,6 Körpergewicht zu
Studienbeginn, kg
–1,0
–1,4 Placebo (n=153)
–2,0
ERTU 5 mg (n=155)
ERTU 15 mg (n=152)
–3,0
–3,2
–4,0 -3,6
–1,8c Unterschied zu Placebo
c
–2,2
Terra SG et al. Diabetes Obes Metab. 2017;19:721–728. Zaccardi F. et al. Diabetes Obes Metab 2016Blutdrucksenkung Mazidi M. et al. J Am Heart Assoc 2017
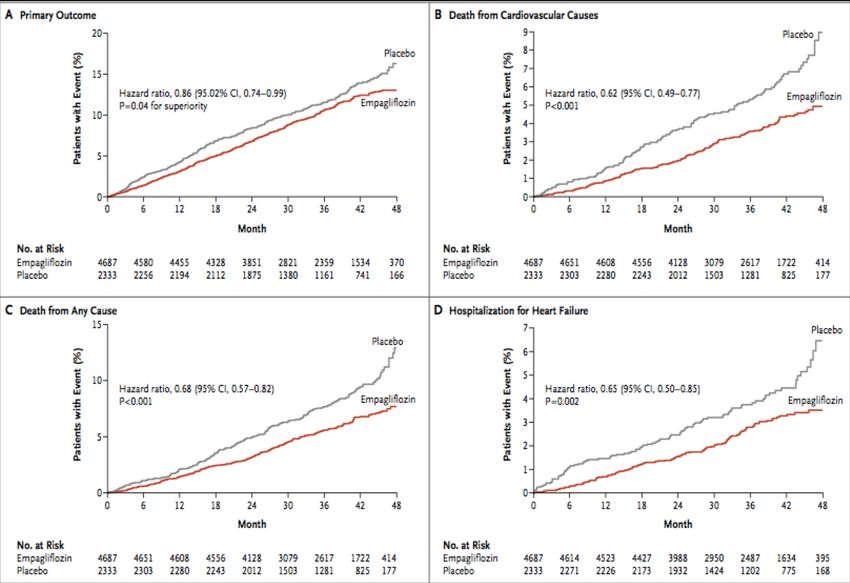
Design – EMPA REG OUTCOME
Placebo
(n=2333)
Randomisiert u.
Gescreent Empagliflozin 10 mg
behandelt (n=2345)
(n=11531)
(n=7020)
Empagliflozin 25 mg
(n=2342)
• Haupteinschlusskriterien
– Erwachsene mit Typ 2 Diabetes
– BMI ≤45 kg/m2
– HbA1c 7–10%*
– Vorbestehende kardiovaskuläre Erkrankung
• Vorangegangener Myokardinfarkt, KHK, Insult, instable AP od. pAVK
• Hauptausschlusskriterien
– eGFREMPA REG OUTCOME
EMPA-REG OUTCOME
Placebo
(n=2333)
Randomisiert u.
Gescreent Empagliflozin 10 mg
behandelt (n=2345)
(n=11531)
(n=7020)
Empagliflozin 25 mg
(n=2342)
• Haupteinschlusskriterien
– Erwachsene mit Typ 2 Diabetes
– BMI ≤45 kg/m2
– HbA1c 7–10%*
– Vorbestehende kardiovaskuläre Erkrankung
• Vorangegangener Myokardinfarkt, KHK, Insult, instable AP od. pAVK
• Hauptausschlusskriterien
– eGFRSGLT2-Hemmer CVOT im Vergleich
EMPA-REG CANVAS DECLARE- TIMI 58
Endpunktstudie mit Ertugliflozin
OUTCOME Programm
(VERTIS CV) läuft aktuell noch.
Hospitalisierung HI oder CV 0.83 (0.73 – 0.95)
Tod
3p MACE 0.86 (0.74-0.99) 0.86 (0.75-0.97) 0.93 (0.84-1.03)
Nicht-tödlicher Herzinfarkt 0.87 (0.70-1.09) 0.85 (0.69-1.05) 0.89 (0.77 – 1.01)
Nicht-tödlicher Schlaganfall 1.24 (0.92-1.67) 0.90 (0.71-1.15) 1.01 (0.84-1.21)
*Verdopplung des Serumkreatinins, Beginn einer
CV-Tod 0.62 (0.49-0.77) 0.87 (0.72-1.06) 0.98 (0.82 -1.17) Nierenersatztherapie, Tod aufgrund einer
Nierenerkrankung
Gesamtmortalität 0.68 (0.57-0.82) 0.87 (0.74-1.01) 0.93 (0.82 – 1.04) **40% Reduktion der eGFR, ESRD, Tod aufgrund einer
Nierenerkrankung
Hospitalisierung HI 0.65 (0.50-0.85) 0.67 (0.52-0.87) 0.73 (0.61 – 0.88)
Komb. Renaler Endpunkt 0.54 (0.40-0.75)* 0.60 (0.47-0.77)** 0.53 (0.43 -0.66)**
Empa-REG (N=7,020)
N=6,950 Manifeste CV Erkrankung
CV Risikofaktoren
CANVAS ~34.4% MRF (N=10,142)
N=6,656 N=3,486
DECLARE ~59.4% MRF (N=17,160)
N=6,974 N=10,186eGFR (CKD-EPI) über 192 Wochen
2 5 6 8 9
Baseline 4 12 108 122 136 150 164 178 192
8 2 6 0 4
No. analyzed
Placebo 2323 2295 2267 2205 2121 2064 1927 1981 1763 1479 1262 1123 977 731 448
Empagliflozin 10 mg 2322 2290 2264 2235 2162 2114 2012 2064 1839 1540 1314 1180 1024 785 513
Empagliflozin 25 mg 2322 2288 2269 2216 2156 2111 2006 2067 1871 1563 1340 1207 1063 838 524
No. in follow-up for
adverse/outcome events
Total 7020 7020 6996 6931 6864 6765 6696 6651 6068 5114 4443 3961 3488 2707 1703
eGFR, estimated glomerular filtration rate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration. Wanner C. et al. NEJM 2016Verdopplung des Serumkreatinins*, Beginn einer Nierenersatztherapie,
Tod aufgrund einer Nierenerkrankung
Kaplan-Meier estimate in patients treated with ≥1 dose of study drug.
Hazard ratios are based on Cox regression analyses.
*Accompanied by eGFR [MDRD] ≤45 ml/min/1.73m2. HR, hazard ratio; CI, confidence interval. Post-hoc analyses.
Wanner C. et al. NEJM 2016Mechanismen
SGLT 2 Inhibition Daten gestützt Hypothese
↓ Insulin/ Glucosurie Natriurese
↑ Glucagon
Negative ↓ HbA1c ↑ Uricosurie ↓ Blutdruck ↓ Plasma- ↑ Tubulo-
Kalorien- volumen glomerulärer
balance Feedback
↓ Körperfett ↓ Inflammation ↓ Arterielle ↓ Myokardiale Afferente
↓ Plasma
↓ Glukosetoxizität Gefäß- Dilatation Arteriolen-
Harnsäure konstriktion
Keton steifigkeit
körper-
Produktion ↓ Arteriosklerose ↓ Ventrikuläre Aktivierung
↓ Epikardiales ACE 2-Ang 1/7
Herz: Shift Arrhythmien
Fett
im
Energie- ↓ Intraglomeruläre
substrat
↓ Inflammation ↑ kardiale Hypertension
zu Kontraktilität
Fibrose ↓ Hyperfiltration
Keton-
körpern
Kardiale und renale Protektion
Modifiziert nach Heerspink H et al. Circulation 2016;34: 752-772Nebenwirkungen
4Genitale Pilzinfektionen (Risiko verdreifacht)
4Euglykämische Ketoazidosen
- selten bei PatientInnen mit Typ 2 Diabetes
- meistens ein auslösender Faktor (Infektionen, reduziere Nahrungs- und
Flüssigkeitszufuhr, verstärkter Alkoholgenuss, absoluter
Insulinmangel,…)
à Pausieren im Krankheitsfall
4Erhöhte Raten für periphere Amputationen (nur für Canagliflozin gezeigt)ADA / EASD consensus To avoid
clinical inertia
reassess and
FIRST-LINE THERAPY IS METFORMIN AND COMPREHENSIVE LIFESTYLE (INCLUDING WEIGHT MANAGEMENT AND PHYSICAL ACTIVITY) modify
IF HbA1c ABOVE TARGET PROCEED AS BELOW treatment
regularly
NO (3–6 months)
Established ASCVD or CKD
Without established ASCVD or CKD
ASCVD predominates
HF OR CKD predominates
PREFERABLY Compelling need to minimise hypoglycaemia Compelling need to minimise weight
Cost is a major issue††‡‡
EITHER/ SGLT-2i with evidence of reducing HF gain or promote weight loss
OR SGLT-2i and/or CKD progression in CVOT if eGFR DPP-4i GLP-1RA SGLT-2i† TZD
GLP-1RA with proven adequate‡
with proven CVD benefit*, GLP-1RA
OR EITHER/
CVD benefit* if eGFR with good SU|| TZD‡‡
If HbA1c If HbA1c If HbA1c If HbA1c OR SGLT-2i†
adequate† If SGLT-2i not tolerated or contraindicated efficacy for
or if eGFR less than adequate† add GLP-1RA above target above target above target above target weight loss**
with proven CV benefit*
If HbA1c above target If HbA1c above target
GLP-1RA SGLT-2i†
If HbA1c above target If HbA1c above target SGLT-2i† SGLT-2i†
OR OR
GLP-1RA
OR OR DPP-4i DPP-4i SGLT-2i† with good efficacy TZD‡‡ SU||
If further intensification is required or • Avoid TZD in the setting of HF for weight loss**
patient is now unable to tolerate GLP-1RA OR OR
TZD TZD
and/or SGLT-2i, choose agents Choose agents demonstrating CV safety: TZD GLP-1RA
demonstrating CV safety: • Consider adding the other class with
If HbA1c above target If HbA1c above target
proven CVD benefit*
• Consider adding the other class • DPP-4i (not saxagliptin) in the setting
(GLP-1RA and/or SGLT-2i) with of HF (if not on GLP-1RA)
If HbA1c above target If triple therapy required or SGLT-2i
proven CVD benefit • Basal insulin§ • Insulin therapy basal insulin
and/or GLP-1RA not tolerated or
• DPP-4i if not on GLP-1RA • SU|| with lowest acquisition cost
contraindicated use regimen with
• Basal insulin§ Continue with addition of other agents as outlined above lowest risk of weight gain OR
• TZD¶ • Consider DPP-4i OR SGLT-2i with
PREFERABLY
• SU|| lowest acquisition cost‡‡
DPP-4i (if not on GLP-1RA)
If HbA1c above target based on weight neutrality
Consider the addition of SU|| OR basal insulin:
• Choose later generation SU with lower risk of hypoglycaemia If DPP-4i not tolerated or
• Consider basal insulin with lower risk of hypoglycaemia# contraindicated or patient already on
GLP-1RA cautious addition of:
● SU|| ● TZD¶ ● Basal insulin
*Proven CVD benefit means it has label indication of reducing CVD events. For GLP-1RA strongest evidence for liraglutide>semaglutide>exenatide extended release. For SGLT-2i evidence modestly stronger for
empagliflozin>canagliflozin; † Be aware that SGLT-2i vary by region and individual agent with regard to indicated level of eGFR for initiation and continued use; ‡ Both empagliflozin and canagliflozin have shown reduction in
HF and reduction in CKD progression in CVOTs; § Degludec or U100 glargine have demonstrated CVD safety; ¶ Low dose may be better tolerated though less well studied for CVD effects; ||Choose later generation SU with
lower risk of hypoglycaemia; # Degludec / glargine U300dulaglutide>exenatide>lixisenatide; †† If no specific comorbidities (i.e. no established CVD, low risk of
hypoglycaemia and lower priority to avoid weight gain or no weight-related comorbidities); ‡‡ Consider country- and region-specific cost of drugs. In some countries, TZDs relatively more expensive and DPP-4i relatively
cheaper
Davies MJ et al. Diabetologia and Diabetes Care 2018GLP-1 RA with proven CVD benefit:
SGLT2-I with proven CVD benefit:
Liraglutide > Semaglutide > Exenatide LAR
Empagliflozin > Canagliflozin
Davies MJ et al. Diabetologia and Diabetes Care 2018ADA / EASD consensus
To avoid
clinical inertia
reassess and
modify
treatment
regularly
(3–6 months)
NO
Without established ASCVD or CKD
Compelling need to minimise hypoglycaemia Compelling need to minimise weight
Cost is a major issue††‡‡
gain or promote weight loss
DPP-4i GLP-1RA SGLT-2i † TZD
GLP-1RA EITHER/
with good OR SU|| TZD‡‡
If HbA1c If HbA1c If HbA1c If HbA1c SGLT-2i†
efficacy for
above target above target above target above target weight loss**
If HbA1c above target If HbA1c above target
GLP-1RA SGLT-2i†
SGLT-2i† SGLT-2i†
OR OR
GLP-1RA
OR OR DPP-4i DPP-4i SGLT-2i† with good efficacy TZD‡‡ SU||
for weight loss**
OR OR
TZD TZD
TZD GLP-1RA
If HbA1c above target If HbA1c above target
If HbA1c above target If triple therapy required or SGLT-2i
and/or GLP-1RA not tolerated or • Insulin therapy basal insulin
contraindicated use regimen with with lowest acquisition cost
Continue with addition of other agents as outlined above lowest risk of weight gain OR
• Consider DPP-4i OR SGLT-2i with
PREFERABLY
lowest acquisition cost‡‡
DPP-4i (if not on GLP-1RA)
If HbA1c above target based on weight neutrality
Consider the addition of SU|| OR basal insulin:
• Choose later generation SU with lower risk of hypoglycaemia If DPP-4i not tolerated or
• Consider basal insulin with lower risk of hypoglycaemia# contraindicated or patient already on
GLP-1RA cautious addition of:
● SU|| ● TZD¶ ● Basal insulin
Davies MJ et al. Diabetologia and Diabetes Care 2018Kreatinin-Clearance 30-60 ml/min
Metformin 2000mg 1000mg
60 45 30
DPP-4 Hemmer
Alogliptin 25 mg 1xtägl. 12,5 mg 1xtägl.
Linaglitpin 5 mg 1xtägl.
Sitagliptin 100 mg 1xtägl. 50 mg 1xtägl.
Saxagliptin 5 mg 1xtägl. 2.5 mg 1xtägl.
Vildaplitin 50 mg 2xtägl. 50 mg 1xtägl.
60 50 45 30
GLP-1 Rezeptoragonisten
Liraglutide, Dulaglutide, Lixisenatide
Exenatide EQW
60 50 45 30
Pioglitazon
60 45 30
Sulfonylharnstoffe (Gliclazid, Glimepirid) Cave
60 45 Hypoglykämie 30
SGLT-2 Hemmer
Empagliflozin,Dapagliflozin
Canagliflozin, Ertugliflozin
Nicht unter 60 ml/min/1,73 m2 beginnen aber bis 45 ml/min/1,73 m2 belassen
60 45 30
Insulintherapie
60 45 30GLP-1RA und SGLT-2 Hemmer in Kombination
↓ Appetit
↑ glukoseabhängige
Insulinsekretion ↑ Glukoseaus-
↓ Blutzucker scheidung
↓ Blutdruck
GLP- SGLT-2i
↓ Blutdruck
↑ LV Funktion
1RA
↓ Infarktgröße ↓ Gewicht
↓ CV Events
↓ Blutdruck
↓ Gefäßsteifigkeit
↓ Inflammation
Verlangsamte
Magenentleerung
Aus der DURATION -8 Präsentation EASD München 2016DURATION-8 Jabbour SE et al. Diabetes Care 2018; Hardy T. et al Presentation EASD 2018
DURATION-8 Jabbour SE et al. Diabetes Care 2018
Zusammenfassung 4 SGLT-2 Hemmer führen zu einer pharmakologisch induzierten Glukosurie. 4 SGLT-2 Hemmer reduzieren neben dem Blutzucker auch das Körpergewicht. 4 Kardiovaskuläre Endpunkstudie zeigen konstant eine Reduktion der Hospitalisation für Herzinsuffizienz und renaler Endpunkte. 4 Es zeigt sich auch eine Reduktion kardiovaskulärer Endpunkte und/oder der Mortalität – je nach Substanz. 4 Bei PatientInnen mit kardiovaskulärer Erkrankung sind SGLT-2 Hemmer neben GLP1- Rezeptoragonisten die empfohlenen Zweitlinienpräparate nach Metformin. 4 Genitale Pilzinfektionen sind die häufigste Nebenwirkungen der SGLT-2 Hemmer.
You can also read