Disease Research Report: Meningococcal Disease (Meningitis) - Jason K. Whitson Biology 240 Summer 2005
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Disease Research Report:
Meningococcal Disease
(Meningitis)
Jason K. Whitson
Biology 240
Summer 2005Causative Agent:
Meningitis (Mening/o- – meninges (membranes covering the spinal cord and brain), -it is
– inflammation) is quite literally the inflammation of the spinal cord and brain. (Chabner
884) Meningitis is caused by an infection of the cerebrospinal fluid within the cavities
surrounding the spinal cord and brain. (CDC 1) Bacteria and viruses can both cause
meningitis, however, viral meningitis is typically far less severe then its bacterial relative
and usually resolves itself with no to little medical assistance. (CDC 1)
Meningococcal disease is caused by Neisseria meningitidis, also known as
meningiococcus. (CDC 2) N.meningitidis can be found naturally occurring in the upper
respiratory tracts of 5% to 30% of healthy individuals who are entirely asymptomatic.
(Todar 1, 12)
The Gram-negative aerobic bacteria is in many ways identical to that of N.gonorrhoeae
in its staining and morphological characteristics with the exception that N.meningitidis
also protects itself with a prominent antiphagocytic polysaccharide capsule. (Todar 1, 9)
The bacteria is typically cultivated in a peptone-blood based medium in a humid
environment containing 5-10% CO2. (Todar 9)
A rather unusual and unique trait of N.meningitidis is that before inoculation, all media
must be warmed to 37 degrees Centigrade as the bacteria is extremely susceptible to
temperatures outside of this range. Another unusual trait is the rapid rate at which
N.meningitidis undergoes autolysis after death, both in vitro and in vivo. (Todar 9) “This
accounts for the dissemination of lipopolysaccharide (endotoxin) during septicemia and
meniginitis.” (Todar 9)
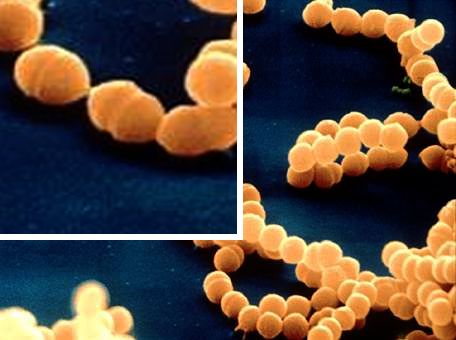
Bacteria in the Neisseria order are approximately 0.6
to 1.0 micrometers in size and are diplococci (twin
spheres squeezes together) with their adjacent sides
flattened against one-another. (Kenyon 1)
N.meningitidis is described as aerobic, strongly
oxidase-positive, having an oxidative metabolism,
susceptible to drying and is fastidious. (Kenyon 1, 2)
N.meningitidis, Courtesy of K.Todar, UoW
Edited for display purposes.
History:
Meningococcal disease was first described in Geneva, Switzerland in 1805. However
wasn’t until eighty-two years later in 1887 when the causative agent, Neisseria
meningitidis, was identified. (CSTS 1) Meningococcal meningitis during the first decade
of the 20th century was reported to have a mortality rate between 75% and 80%. (Swartz
2)
The first break in the in the deadly history of bacterial meningitis came in 1913 when
Simon Flexner began treating bacterial meningitis with intrathecal equine meningococcal
antiserum. (Swartz 2) The results to highly favorable; of the 169 children infected withmeningococcal meningitis at Bellevue Hospital in New York between 1928 and 1936, the
mortality rate was down to 20%. (Swartz 2) Again in the 1930s, with the introduction of
sulfonamides, the mortality rate again dropped, this time to 5% to 15%. (Swartz 2) Over
the course of the last fifteen years (as of 2004), the primary treatment for community-
acquired bacterial meningitis has primarily involved treatment with intravenous penicillin
(or ampicillin), a third-generation cephalosporin, or both. The current treatment plan has
resulted in a mortality rate of approximately 10% for meningococcal meningitis; 7% in
the Netherlands. (Swartz 2)
When it was demonstrated that the bacterial components could cause inflammation by the
release of cytokines, trials using dexamethasone as an adjuvant therapy were performed.
In 1990 trials involving H.influenzae meningitis, the use of dexamethasone did not affect
the mortality rate, but instead lowered the instances of neurological damage, primarily
sensorineural hearing loss. (Swartz 2) Later in 2002, Dutch tests show that in adults,
adjuvant dexamethasone therapy reduce the frequency of unfavorable outcomes from
25% to 15%, most noticeably in pneumococcal meningitis. (Swartz 2) No research
available at the time of this report directly expressed the results for the affects of adjuvant
dexamethasone therapy on meningococcal meningitis.
World Impact:
Meningococcal is a disease that has had some form of
impact on nearly every part of the world. Recently in
the past thirty years Asia has suffered a series of major
epidemics: China in 1979 and 1980, Viet Nam in 1977,
Mongolia in 1973 and 1974 and again in 1994 and
1995, Saudi Arabia in 1987, and Yemen in 1988.
(WHO-Impact 1)
Throughout the last thirty years, Europe and the
Americas have also experienced epidemics, but not
with the magnitude that other parts of the world have African meningococcal belt. Courtesy of
World Health Organization.
experienced. (WHO-Impact 1)
Currently, the largest and most reoccurring outbreaks have been located in the semi-arid
area of sub-Saharan Africa in an area known at the African meningitis belt. (WHO-
Impact 1) The AMB stretches across Africa from Senegal to Ethiopia, encompassing an
estimated 300 million people. (WHO-Impact 1) Occuring in seasonal cycles between late
November and late June, meningococcal epidemic season can vary in intensity due to
location and the arrival of the rainy season. (WHO-Impact 1) Within the AMB,
epidemics of meningococcal disease often occur in cycles of eight to fifteen years.
(WHO-Impact 1)
The most recent pandemic of meningococcal meningitis recently appeared in the mid-
1990s. (WHO-Impact 1) Burkina Faso, Chad, Niger, Mali, Nigeria and other countries
reported 190,000 cases of meningococcal meningitis to the World Health Organization in
1996. (WHO-Impact 1) This epidemic quite literally overwhelmed and paralyzed the
local health care systems of the affected countries and quickly exhausted the international
stocks of vaccine. (Who-Impact 1) “In 1997, the International Coordinating Group (ICG)for Vaccine Provision for Epidemic Meningitis Control was established.” (WHO-Impact 1) Six countries in the AMB experienced large epidemics in 2001: Benin, Burkina Faso, Central African Republic, Chad, Ethiopia, and Niger. (WHO-Impact 1) There are several serious socioeconomic implications of meningococcal disease. The amount of vaccine, medicines and logistical support required makes it difficult to adequately control and prevent epidemics. When an epidemic does occur, a secondary impact is that normal health services in the affected countries are disrupted. (WHO- Impact 2) Higher incident of meningococcal disease has been linked to factors such as poor living conditions and overcrowded housing, and those who do not have the means for acquiring any kind of medical care typically suffer the greatest during an outbreak. Migration and travel are also considered possible facilitative means by which the circulation of pathogenic strains move inside a country, from country to country, and in theory, large population movements such as that of pilgrimages can possibly be blamed for the spread of the disease. (WHO-Impact 2) Refugees finding refuge within large populations are also considered to be a possible risk for the spread of the disease. (WHO-Impact 2) “Waning herd immunity to a particular strain in a population may be necessary for an outbreak to occur and could contribute to the regularity of the epidemic cycles in sub-Saharan Africa.” (WHO-Impact 2) Epidemiology: Meningococcal disease can occur almost anywhere in the world. Recently however in the last half century, the disease has been most prevalent in Asia and Africa. The most recent pandemic in Africa reported over 190,000 cases. (WHO-Impact 1) With proper medication and treatment, the rate of mortality is as low as 7% in some countries. (Swartz 2) Without antibiotics and other medications, the mortality rate of meningococcal meningitis is calculated at approximately 80%. (Swartz 1) Humans are the only known host of Neisseria meningitidis, the bacteria that causes meningococcal meningitis. (Todar 9) The transmission of N.meningitidis is through that of throat and respiratory secretions. The spread of the disease is facilities by close and prolonged contract (close quarters, kissing, coughing, sharing utensils, etc). (CSTS 1) Pathology: N.meningitidis usually enters the body through the pharynx and for an unknown reason, in some individuals, ends up overwhelming the body’s natural defenses causing an infection; the infection will quickly spread through the blood and to the brain. (CSTS 1) N.meningitidis tends to occur intracellularly inside neutrophils in their cytoplasm. The neutrophils in turn are attracted to the sites of inflammation in the mininges. (Todar 10) The bacteria are protected from the phagocytic action of the neutrophil by an antiphagocytic polysaccharide capsule. (Todar 11)
During its growth cycle, N.Meningitidis undergoes autolysis and releases part of its cell wall. With the release of the cell wall portion, lipooligosaccharide is released and acts as an endotoxin. (Todar 11) Once an individual is infected, the average incubation time is four days, with a range of two to ten days. (CSTS 1) Early symptoms of meningococcal disease are stiff neck, high fever, sensitivity to light, confusion, headache, and vomiting. (CSTS 1) 5% to 10% of patients die typically within 24 to 48 hours of symptom onset, even if they receive adequate treatment. (CSTS 1) For 10% to 20% of survivors, brain damage, hearing loss, and learning disabilities occurs. (CSTS 1) Another form of meningococcal disease is that of meningococcal septicemia which is often accompanied by hemorrhagic rashes and rapid circulator collapse. (CSTS 1) Response and Treatment: N.meningitidis is only able to establish systemic infections in individuals who lack the antibodies against the capsular and noncapsular antigens of the invading strain, or “in patients deficient in the late-acting complement components.” (Todar 11) Another point of importance seems be that that of the integrity of the pharyngeal and repiratory epithelium; reoccurring irritation of the mucosa due to environmental factors or infection can assist N.meningitidis in infecting the host. (Todar 11) “The presence of serum bactericidal IgG and IgM is probably the most important host factor in preventing [the] invasive disease.” (Todar 11) Penicillin is the treatment of choice when treating meningococcal meningitis. (Todar 11) While penicillin normally is unable to penetrate the blood-brain barrier, when the meninges are inflamed (as in a meningococcal infection), penicillin passes readily through the barrier. (Todar 11) In individuals allergic to penicillin (or ampicillin), chloramphenicol or a third-generation cephalosporin is used. The use of ‘cillins and other medicals and with the use of adjuvant dexamethasone therapy, the mortality rate of meningococcal disease has dropped from approximately 80% to approximately 7% to 10%. (Swartz 2) Preventive measures include the use of chemoprophylactics. Sulfonamides were the medication of choice for this task for years, but recently it has been discovered that nearly 25% of clinically isolated N.meningitidis in the United States is sulfonamides-resistant, today rifampin is utilized, as there is significantly lower resistance rates associated with it. (Todar 11) Specific vaccines have also been developed and are in use that targets the four main strains of N.meningitidis. (Todar 11) It is hoped that eventually a universal meningococcal vaccine can be developed, but efforts thus far have been hampered by “the high degree of variation in the proteins on the surface of the bacterium which leads to the occurrence of many different antigenic types.” (Todar 11)
Works Cited
CDC. “Meningococcal Disease.” DBMD – Meningococcal Disease – General
Information: CDC website; 7/15/05
CSTS. “Meningococcal meningitis.” Fact Sheet on Meningococcal meningitis: Rev. May
2003. Child Survival Technical Support; 7/17/05
Kenyon College. “Neisseria.” Microbiology Dept, Kenyon College; 7/17/05
Swartz, Morton N. “Bacterial Meningitis – A View of the Past 90 Years.” The New
England Journal of Medicine Boston: Oct 28, 2004. Vol. 351, Iss. 18; pg. 1826, 3
pgs. Proquest; Cannell Library, Vancouver WA. 7/17/05
Todar, Kenneth. “The Pathogenic Neisseriae.” Todar’s Online Textbook of Bacteriology:
2004. University of Wisconsin-Madison Dept. of Bacteriology; 7/15/05
WHO. “Meningococcal Disease.” Impact of the Problem: World Health Organization
website; 7/15/05You can also read