EVALUATION OF RADIOTHERAPY OF PATIENTS WITH GRAVES' DISEASE TREATED WITH FIXED ACTIVITIES OF 555 MBq OF IODINE-131
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2013 International Nuclear Atlantic Conference - INAC 2013
Recife, PE, Brazil, November 24-29, 2013
ASSOCIAÇÃO BRASILEIRA DE ENERGIA NUCLEAR - ABEN
ISBN: 978-85-99141-05-2
EVALUATION OF RADIOTHERAPY OF PATIENTS WITH GRAVES’
DISEASE TREATED WITH FIXED ACTIVITIES OF 555 MBq OF
IODINE-131
José M. F. da Silva1, João A. Filho2, Manoel R. de S. Júnior3 e Keyla M. C. Mendonça4
1
Department of Nuclear Energy (DNE) – Federal University of Pernambuco
1000 Professor Luiz Freire Ave – University City
50740-540 Recife, PE
josemarcosfs@yahoo.com.br
2
Department of Nuclear Energy (DNE) – Federal University of Pernambuco
1000 Professor Luiz Freire Ave – University City
50740-540 Recife, PE
jaf@ufpe.br
3
Department of Nuclear Energy (DNE) – Federal University of Pernambuco
1235 Professor Moraes Rego Ave – University City
50670-901 Recife, PE
manoel@de.ufpe.br
4
Department of Nuclear Energy (DNE) – Federal University of Pernambuco
1000 Professor Luiz Freire Ave – University City
50740-540 Recife, PE
keylamcm@yahoo.com.br
ABSTRACT
Graves’ disease treatment is done by radioiodine therapy (RIT), which destroys cells of the thyroid and reduces
the synthesis of T3 and T4; and surgery. In Brazil, applies RIT with fixed activities. Studies show that RIT
should be based on individual biokinetics. There is controversy regarding the use of fixed activities or
calculated. This study was conducted at the HC-UFPE in the period 2006-2010. Of the overall sample of 132
patients that entered the study, twenty-five of them formed a group chosen to estimate the maximum uptake of
131
I and thyroid mass, to calculate the activity to be administered and the absorbed dose. All the patients were
treated with fixed activities of 555 MBq 131I. Observed that 28% of patients received radioactivities above, 72%
received radioactivities below, and nobody received no radioactivity as a real need. The group obtained an
average rate of cure of (76 ± 5) % at 24 months of follow up, less than those obtained under the same conditions
biokinetics and mean follow-up interval, among many, who have used doses of 250 Gy and 350 Gy and
achieved cure rates approximately 90%. Doses received totaled 9,166 Gy, and 6,698 Gy were necessary,
therefore were wasted 2,468 Gy. Were risk factors observed: extrapolation of interval of the thyroid function
tests of three to six months to one to three years; economic difficulties, interfamily, socioemotional and to
perform the tests requested and great distances between homes and hospital; among others; may be limitations
that led to the contraposition that higher activities of 131I promote greater cure rate of GD. Results of univariate
analysis – were statistically significant risk factors: female, thyroid mass between 31 g and 60 g and duration of
the GD before of RIT > five years (p < 0.05). The factors sex and thyroid mass are consistent with other studies.
The results suggest the use of optimized activities based on individual dosimetric parameters and the
implementation of more effective public policies for the patient accompaniments, so that be decreased the
radiological risks, detriments and unnecessary expenses.
Keywords: Fixed activity. Graves’ disease. Risk factors. Thyroid. Radioiodine therapy.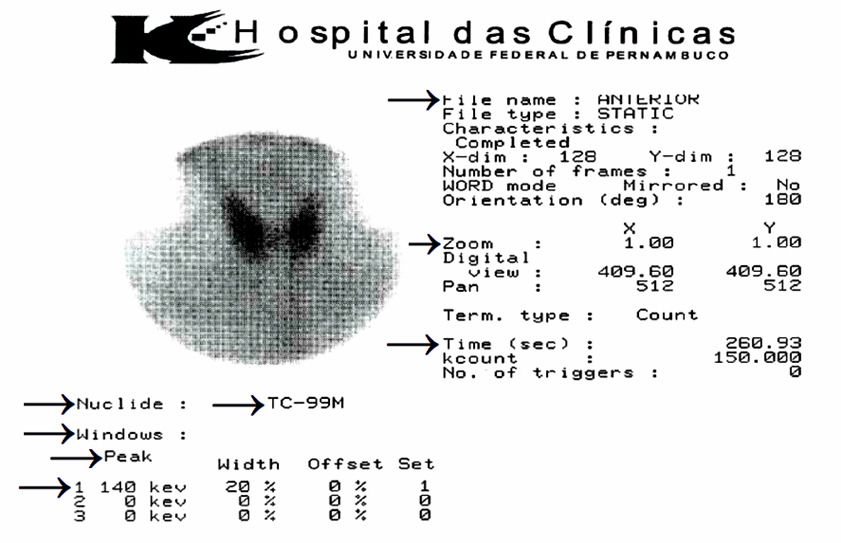
1. INTRODUCTION
The thyroid is an endocrine glands, the largest of the human body located in the neck in front
of the trachea, a structure composed of two lobes and sometimes with a central isthmus
(Figure 1), is responsible for producing the hormones triiodothyronine (T3) and
tetraiodothyronine (T4) – where iodine is the basic component – act in regulating the rate of
metabolism and affect the growth and function of many other systems of the body [1].
Hyperthyroidism (very active thyroid) of Graves' disease, caused by the production of
autoantibodies, overproduction of T3 and T4 and thyroid hyperplasia (Figure 2), presents
symptoms: agitation, anxiety and irritability; diarrhea or increased bowel movements,
difficulty in lifting heavy materials, excessive hunger, fatigue and tiredness, weakness,
infertility, insomnia, ophthalmopathy; much weight loss, even with normal feeding; sweat
excessive and exaggerated sense of warmth, tachycardia and hand tremors [2, 3].
Currently, treatments applied to thyroid disease are: antithyroid drugs (ATD), which inhibit
the formation of T3 and T4; radioiodine therapy (RIT) with the radiopharmaceutical sodium
iodide (Na131I), which destroys the thyroid cells and reduces the synthesis of T3 and T4, and
Surgery.
In Brazil typically applies RIT with fixed activities. Studies have shown that RIT should be
based on individual biokinetics [4]. There is controversy regarding the use of fixed activities
or calculated. The administration of fixed activities resulted in the under and over-exposure to
radioactivity, producing radiological detriments and unnecessary expenses.
The medical literature presents a large number of studies on the treatment of GD, which
evaluated the use of 131I as a therapeutic option, without considering the biokinetics patient
with regard to the amount of activity to be administered, so that it results in a optimal
relationship between this quantity and the quality of the result obtained [5, 6, 7].
Currently, RIT can apply different ways of evaluating the activity to be administered, among
them, the equations Quimby-Marinelli (1948), the Computed Tomography Single Photon
Emission (SPECT, 1990), the formalism of the Medical Internal Radiation Dosimetry
(MIRD, 1991) and Positron Emission Tomography (PET, 1993), [8].
However, in the medical literature there are two classical protocols for the administration of
131
I activity for treating Graves’ disease. The first uses fixed activities varying from 370 MBq
(MegaBequerel) ou10 mCi (millicurie) to 555 MBq or 15 mCi, using the method of palpation
to determine the mass of the thyroid. In the second, the activity is calculated as the percentage
(%) of maximal uptake of 131I in 24 hours and thyroid mass, using the MIRD and Quimby-
Marinelli equations [9].
Therefore, considering this context, the present study had the objective to evaluate the RIT
with fixed activities of 555 MBq of 131I, comparing them with activities adjusted for
maximum uptake and thyroid mass and the residence time of the Na131I, and the clinical
performance of the GD, two years post-RIT, considering gender, thyroid mass, duration of
GD before RIT and previous medication, as risk factors related to the cure.
INAC 2013, Recife, PE, Brazil.
2. PATIENTS AND METHODS
After approval of the Ethics Committee, the study was conducted at the Clinical Hospital of
the Federal University of Pernambuco (CH-FUPE) in the period 2006-2010. Initially from a
sample of 132 patients, has been selected a group of 25 patients prospective (Table 1) to
obtain maximal uptake of 131I in 24 hours and thyroid mass (Figures 2 and 3). Next, the study
sample, now retrospective, which was submitted to RIT with fixed activities of 555 MBq of
131
I (Table 2), based on data from medical records rescued of the Service Medical Records
and Statistics of the Federal University of Pernambuco.
Figure 1: Thyroid and its location in neck.
Figure 2: Thyroid with Graves' disease.
2.1 Estimation of accumulated activity
The accumulated activity before and during scintigraphy was estimated by Equation 1:
INAC 2013, Recife, PE, Brazil.
At = A1 × (1 − e − λ x t ) (1)
Where: At is the accumulated activity for a given time interval t considered, A1 is the activity
measured liquid injected through a Capintec Activimeter model CRC-7 or activity adjusted
for a given time interval considered, e-λxt is the decay factor for a time interval considered,
and λ is the decay constant of 99mTc considered equal to 0.001919 minutes-1 (λ = ln2/6,02h).
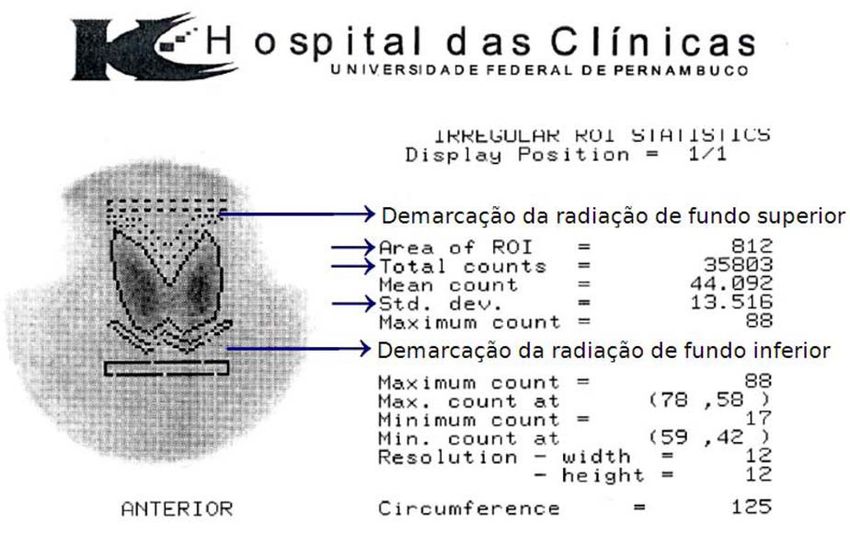
2.2 Estimation of the 99mTc uptake
The estimated uptake of the 99mTc was obtained by the conditioning radiotracer in 5 ml
syringe and measuring the initial activity and residual (post-application) using a Capintec
activimeter. Twenty minutes (min) after injection, the patient was positioned in Gamma
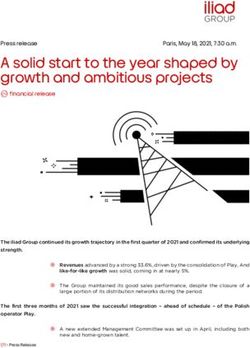
Camera Starcam, for taking the scintigraphy. The data obtained from two irregular ROI
Statistics (Figures 3 and 4) [10] – for each patient – was used in Equation 2 [11]:
PT 100
CTc −99m (%) = (CT − CB) × × (2)
PB CI
Where: CTc-99m(%) is the percentage of uptake of 99mTc, CT is the total count in the ROI (Total
counts), CB is the total count in the ROI background (BG), PT is the number of pixels in ROI
(Area of ROI), PB is the number of pixels in the ROI of the BG, and CI is the count of the
activity adjusted (Equation 1).
Figure 3: Partial thyroid scintigraphy with Graves' disease, showing a window containing the input parameters
and acquisition of Scintigraphy and Uptake of the Thyroid (Time (sec)).
The data from the ROI demarcated BG (top and bottom) – each patient – are presented in
other scintigraphy.
INAC 2013, Recife, PE, Brazil.Figure 4: Partial thyroid scintigraphy with Graves disease, showing a statistic Irregular ROI containing
parameters for the Evaluation of Thyroid Uptake (indicated by arrows).
2.3 Conversion of the uptake 20 min of 99mTc in uptake of 131I in 24h
The conversion of maximum uptake 20 min 99mTc was obtained from Equation 3 [12]:
CI −131(%) =17,72 × lnCTc−99m(%) +30,40 (3)
Where: CI-131(%) is the percentage uptake of I31I in 24h, 17.72 and 30.40 are linear
coefficients, and ln CTC-99m (%) is the neperian logaritm of the percentage of uptake of 99mTc.
2.4 Estimation of thyroid mass
Estimation of thyroid mass was obtained by multiplying the increase in thyroid given by the
Medical Record by the standard mass [13], using Equation 4:
m = nV × M (4)
Where: m is the mass of the thyroid estimated by palpation, in g, nv is the number of volume
increases thyroid estimated by the physician in increments of 1, 1.5, 2.0, 2.5, etc. times the
normal volume of the thyroid, M is the mass standard thyroid, 16.25 g/normal volume of the
gland for women and 17 g/normal volume of the gland to the Brazilian man.
2.5 Calculation of the activity to be administered and absorbed dose
INAC 2013, Recife, PE, Brazil.Calculations of activities and absorbed doses were performed by Equation 5 [14]:
DT (Gy ) × m ( g )
A ( MBq) = (5)
0,041× Cap (%) × TR (dias )
Where A is the activity to be administered, DT is the absorbed dose required for thyroid (200
Gy/g – related cure rates > 90%) [15], m is the mass of the thyroid; 0.041 is a constant due
the correlation between the old units of absorbed dose and activity (rad and mCi) used in the
MIRD S factor [16] and the units of absorbed dose and activity of the International System of
Units (Gy and GBq) and, Cap (%) is the percentage of maximum uptake of 131I in 24 and TR
is the residence time of the radiopharmaceutical in the organ (or TF of the 131I) [5].
3. RESULTS AND DISCUSSION
Table 1 presents the activities and absorbed doses fixed and calculated.
Table 1: Parameters of 25 patients with Graves' disease prospective submitted to thyroid scintigraphy with 555
MBq of 131I, in the Nuclear Medicine Service of CH-FUPEa in the period 2006-2007.
Patients Age Maximum Thyroid Activities Absorbed doses
(years)uptake (%) mass (MBq) (Gy)
99m 131
Tc I (g) Fixed Calculated Required Fixed
1 18 6.96 65 49 555 488 243 213
2 50 2.39 46 24 555 477 351 301
3 59 0.83 27 49 555 2826 101 513
4 18 1.18 33 26 555 1004 232 420
5 59 19.67 83 24 555 146 633 166
6 47 36.50 94 24 555 114 717 147
7 38 9.11 70 49 555 420 261 198
8 51 1.22 34 68 555 2473 91 408
9 64 45.85 98 24 555 105 747 141
10 61 6.50 64 24 555 246 488 216
11 44 4.67 58 24 555 300 442 239
12 20 12.01 74 33 555 253 410 187
13 45 7.75 67 49 555 459 250 207
14 45 1.70 40 49 555 1288 149 347
15 55 4.73 58 24 555 300 442 179
16 36 3.82 54 24 555 346 412 257
17 39 2.11 44 32 555 695 252 315
18 44 2.25 45 16 555 332 515 308
19 44 13.23 76 49 555 357 284 183
20 37 1.46 37 16 555 491 423 374
21 51 1.70 40 24 555 631 305 347
22 40 14.31 78 41 555 283 348 177
23 70 4.66 58 50 555 625 212 239
24 20 2.27 45 24 555 498 343 308
25 39 2.34 45 16 555 332 515 308
Average 44 8.37 57 33 555 620 367 268
Standard deviation 14 10.86 19 14 0 667 173 96
a. Clinical Hospital of the Federal University of Pernambuco. Source: the study itself.
INAC 2013, Recife, PE, Brazil.All activities and fixed and calculated absorbed doses showed statistically significant
differences (p < 0.05), according to the Chi-Square Test of Independence with a Degree of
Freedom.
It is observed that 28% of patients received up activities above, 72% received activities
below, and none of them received their activity dose according to real necessity. The
prospective group of 25 patients received a average dose of (367 ± 173) Gy.
The group of retrosprospective patients (including the 25 prospective) obtained an average
cure rate (76 ± 5) % at 24 months follow-up. Rate lower than the rates obtained for the same
conditions biokinetic and average follow-up times, among many studies using doses between
250 and 350 Gy and obtained cure rates greater than 90% [17, 18].
Group of Table 1, the doses received totaled 9,166 Gy, and the necessary resulted in a total of
6,698 Gy, so were wasted an amount of 2,468 Gy, or 27% of the radiotracer available to
serve that demand.
Factors of inefficiency observed: extrapolation of time limits stipulated for tests of thyroid
function of three to six months for about one to three years; economic difficulties,
interfamily, socioemotional and to perform the required examinations; great distances among
the residences and CH-FUPE, among others, may be limitations that led to the contraposition
that higher activities of 131I promote higher cure rate of Graves' disease [19, 20].
The data presented are in disagreement with the guidelines in relation to the amount of
activity to be administered at RIT, so that it results in an optimal relation between the quality
and quantity of the expected outcome of the activity to be used [5, 6, 7].
In the analysis presented in Table 2 – considered the Central Limit Theorem, which gives
large enough samples from 30 elements, approximately normally distributed, which allows to
quantify the uncertainty inherent in statistical inference without having to make major
assumptions difficult to check [21].
Table 2: Parameters of 132 patients (Ni) retrospective with Graves disease treated with antithyroid drugs and
555 MBq of 131I, at the SEM/NMSMNa CH-FUPE in the period 2006-2010
Variable With premedication Without premedication
considered Methimazole Propylthiouracil
N Patients % N Patients % N Patients %
cured cured cured
Sex
Male 16 8 50 3 1 33 5 4 80
Female 73 58 79 19 12 63 16 12 75
Age range
18 to 45 years 75 56 75 12 8 67 14 11 79
46 to 60 years 11 9 82 8 5 63 7 5 71
Over 60 years old 3 2 67 2 1 50 0 0 0
Thyroid mass
16 to 30 grams 48 33 69 7 5 71 14 10 71
31 to 60 grams 36 29 81 11 9 82 6 5 83
Above 60 grams 1 1 100 2 0 0 0 0 0
Disease duration
0.5 to 2.0 years 40 30 70 9 7 78 8 6 75
2.1 to 5.0 years 31 25 81 6 4 67 5 5 100
Over 5.0 years 12 9 75 7 3 43 2 2 100
a. Service of Endocrinology and Metabolism/Nuclear Medicine Service of HC-UFPE. Source: the
study itself.
INAC 2013, Recife, PE, Brazil.Considering this proposition statistics were analyzed, only patients constituent subgroups
containing 30 or more patients in whom remission rates – were as follows: Variable females
(79%), aged 18-45 years (75%), thyroid mass of 31-60 g (81%) and duration of GD before
RIT 2.1 to 5.0 years (81%), making an average cure rate of (76 ± 5) % after 24 months
follow-up.
Rates of remission or cure found here are consistent with the studies [22, 23, 24], confirming
that responses to treatment may depend on the increased activity administered, the thyroid
mass and female factor, which due to higher iodine deficiency, has its maximum uptake
percentage increased, incurring higher absorbed dose, and hence a better result
radiotherapeutic.
The results of the univariate analysis (Odds Ratio with Confidence Interval of 95%) – showed
statistically significant risk factors: female gender (p = 0.036), thyroid mass between 31 g and
60 g (p = 0.029) and duration GD > 5 years (p = 0.008) – strongly associated with response to
treatment with fixed activities of 555 MBq following 24 months. However, the sex factor did
not agree with the study of Canadas et al., 2007 [24]. However, the factors sex and thyroid
mass are consistent with [10, 23, 26].
Figure 5 shows the comparison between the adjusted and fixed activities, showing that only
about 7% of the activities were still acceptable, considering the biokinetic aspect of the
patient and the criteria to adopt a specific absorbed dose of 200 Gy/g of thyroid tissue.
Equation: y = -23,853x + 929,65
3000 R2 = 0,0692
2500
Activities
Activities em MBq
2000
adjusted
1500 Activities fixed
1000
500
0
1 3 5 7 9 11 13 15 17 19 21 23 25
Distribution of fixed activities and calculated for the 25 patients with
Graves' disease
Figure 5: Comparison between fixed activities administered and activities adjusted
INAC 2013, Recife, PE, Brazil.4. CONCLUSION
Given the existence of a disparity between the calculated and fixed activities, We recommend
activities with radioiodine administered optimally, based on the individual biokinetic
parameters and the implementation of more integrated clinical procedures on behalf of
patients. So that the under and over-exposure to activities incompatible with their needs,
radiological risks, environmental impacts, treatment abandonments and unnecessary
expenses, among other inconveniences, are effectively diminished.
ACKNOWLEDGEMENTS
Professionals at the Department of Nuclear Energy, Nuclear Medicine Service, Service of
Endocrinology and Metabolism and Medical Records and Statistics, Federal University of
Pernambuco.
REFERENCES
1. SIMOCELLI, Sylvia. Fisiologia da Tireoide. Artigo online, publicado em 18/06/2012. Disponível em:
https://www.portaleducacao.com.br/Artigo/Imprimir/13540. Acesso em 22 jul 2013.
2. DUARTE, I.. Anatomia patológica de la glándula tiróides. Bócio. 2005. 53k. 1 fotografia color. 640 x
421 pixels. Disponível em: . Acesso em: 28 jul. 2013.
3. CASTILHOS, M. Tireoide. The Hormone Foundation. Disponível em: www.hormone.org. Acesso em
jul de 2013.
4. ARAÚJO, F. et al., Proposta de metodologia para tratamento individualizado com iodo-131em
pacientes portadores de hipertireoidismo da doença de Graves. Radiol Brás, Vol. 40, n.6, pp. 389-395
(2007).
5. INTERNATIONAL COMMISSION ON THE RADIOLOGICAL PROTECTION. ICRP Publication n.
53. Radiation Dose to Patients From Radiopharmaceutical. Oxford. Pergamon Press, 1987.
6. INTERNATIONAL COMMISSION ON THE RADIOLOGICAL PROTECTION. Recommendations
of Internatiotional Commision on Radiological Protection. Oxford. Pergamon Press, 1990.
7. INTERNATIONAL COMMISSION ON THE RADIOLOGICAL PROTECTION. ICRP Publication n.
103. The 2007 Recommendations of the International Commission on Radiological Protection.
Philadelphia, PA: Elsevier, 2007.
8. LIMA, F. F. Otimização da dose terapêutica com 131I para carcinoma diferenciado da tireóide. 2002.
93 pp. Tese (Doutorado em Instrumentação e Dosimetria), Departamento de Energia Nuclear,
Universidade Federal de Pernambuco, Recife, 2002.
9. LOPES, M. H. C. Terapia com 131I para a resolução do hipertiroidismo doença de Graves: seleção da
dose. Arq Bras Endocrinol Metab, Vol. 51, n. 7, pp. 1031-1033 (2007).
10. SILVA, J. M. F. Avaliação da terapêutica com atividades ajustadas e fixas de 444, 555 e 740 MBq de
¹³¹I em pacientes com doença de Graves.Dissertação de Mestrado, Universidade Federal de
Pernambuco, Recife, 95 pp. (2010).
11. KIDOKORO-KUNII, Y. et al., Analysis of the factors associated with Tc-99m pertechnetate uptake in
thyrotoxicosis and Graves’ disease. J Nippon Sch, Vol. 73, n. 1, pp. 10-17 (2006).
12. SMITH, J. J. et al., J Clin Nuc Med, Vol. 15, pp. 80-83 (1990).
13. XIMENES, E. Modelagem computacional do manequim matemático da mulher brasileira para
cálculos de dosimetria interna, Tese de doutorado, Universidade de São Paulo, São Paulo, 222 pp.
(2006).
14. MANZANO, P. R. et al., Revista de Física Médica, Vol. 3, n. 1, pp. 7-11 (2002).
15. PETERS, H. et al., Thyroid, Vol. 7, n. 2, pp. 247-51 (1997).
INAC 2013, Recife, PE, Brazil.16. GEORGE, S. et al., MIRD Pamphlet n. 22 (Abridged): Radiobiology and Dosimetry of alfa-Particle
Emitters for Targeted Radionuclide Therapy. The Journal of Nuclear Medicine, Vol. 51, n. 2, pp. 311-
328 (2010).
17. WILLEMSEN, U. F.; KREISIG, T.; PICKARDT, C. R.; KIRSCH, C. M. Functional results of
radioiodine therapy with a 300-Gy absorbed dose in Graves' disease. Eur J Nucl Méd, Vol. 20, n. 11,
pp. 1051-1055, 1993.
18. USTUN, F. U. et al., The incidence of recurrence and hypothyroidism after radioiodine treatment in
patients with hyperthyroidism in Trakya, a mild iodine deficiency area, during the period 1991–2003.
Annals of Nuclear Medicine, Vol. 19, n. 8, pp. 737-742, 2005.
19. SOLOMON, B. et al., Current trends in the management of Graves' disease. J Clin Endocrinol Metab,
Vol. 70, pp. 1518-1524 (1990).
20. GROSSO, M. et al., Comparison of Different Thyroid Committed Doses in Radioiodine Therapy for
Graves' Hyperthyroidism. Cancer Biotherapy & Radiopharmaceuticals, Vol. 20, n. 2, pp. 218-223,
2005.
21. PAGANO, M.; GAUVREAU, K. Princípios de Bio estatística. São Paulo: Ed. Pioneira Thomson
Learning, 506 pp. (2004).
22. COOPER, D. S. Antithyroid drugs for the treatment of hyperthyroidism caused by Graves’disease.
Endocrinol Metab Clin, Vol. 27, pp. 225-247 (1998).
23. ALLAHABADIA, A. et al., Age and gender predict the outcome of treatment for Graves'
hyperthyroidism. J Clin Endocrinol Metab, Vol. 85, pp. 1038-1042 ( 2000).
24. STREETMAN, D. D.; KHANDERIA, U. Diagnosis and treatment of Graves disease. Ann
Pharmacother, Vol. 37, pp. 1100-1109 (2003).
25 CANADAS, V. et al., Arq Bras Endocrinol Metab, Vol. 51, n. 7, pp. 1069-1076 (2007).
26 SOLOMON, B. Current trends in the management of Graves' disease. J Clin Endocrinol Metab, Vol.
70, pp. 1518-1524 (1990).
INAC 2013, Recife, PE, Brazil.You can also read