MASS CASUALTY INCIDENT (MCI) - AN OVERVIEW - Jim Thomas, Captain EMT-B, EMSI, FF2, FSI, FI
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MASS CASUALTY INCIDENT
(MCI)
AN OVERVIEW
Atlanta bus crash (internet photo)
wikimedia.org
Jim Thomas, Captain
EMT-B, EMSI, FF2, FSI, FI
As emergency responders, we all respond to hundreds of emergency calls every year, and
we have attended many thousands of alarms throughout our careers. A reasonable
number of these emergency calls are not serious; maybe a tripped private alarm, a false
CO alarm, an overheated automobile on the highway, a routine “frequent flyer”
emergency medical call. Most are simply public relations opportunities, but they are, of
course, still important.
At times we actually “get” something; maybe we respond to a house fire or a damage
accident, or we run a good code. We certainly can bring these incidents to successful
conclusion effortlessly, but at the end of the day, that is what the public expects. We will
not be judged on those routine undertakings. Our true value as emergency responders will
be revealed in our ability to handle more extreme circumstances.
There is one type of emergency that many of us may respond and therefore must be ready
for: a true Mass Casualty Incident (MCI).
We constantly practice and prepare for the routine incidents. We study our protocol
books, participate in station drills on firefighting tactics, attend classes to stay sharp on
medical emergencies, practice with ladders, etc. However, we must not forget to practice
our MCI-related skills as well.
This module provides an overview of Mass Casualty Incident components with respect to
emergency medical response. Components include:
¾ INITIAL TRIAGE
¾ PATIENT EXTRACTION
¾ SECONDARY TRIAGE/MEDICAL TREATMENT
¾ TRANSPORTATION OF PATIENTS
Lets get started.
Mass Casualty Incident Defined - A Mass Casualty Incident (MCI) can be defined as an
incident that has produced more casualties than a customary response assignment can
handle. Types of incidents that can produce mass casualties include, but are not limited
to:
9 Multiple vehicle collision
2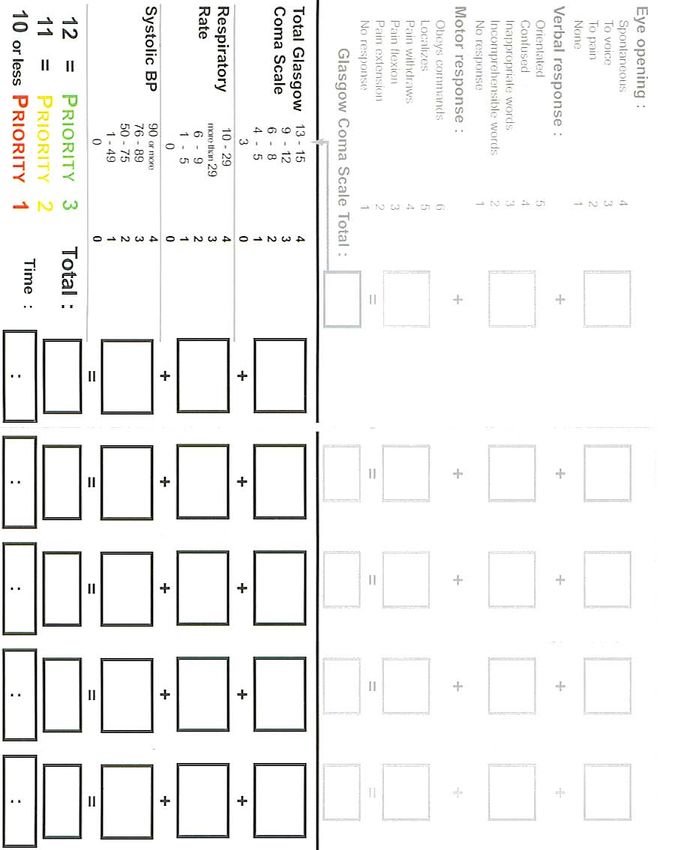
9 Building collapse
9 Mass transit accidents
3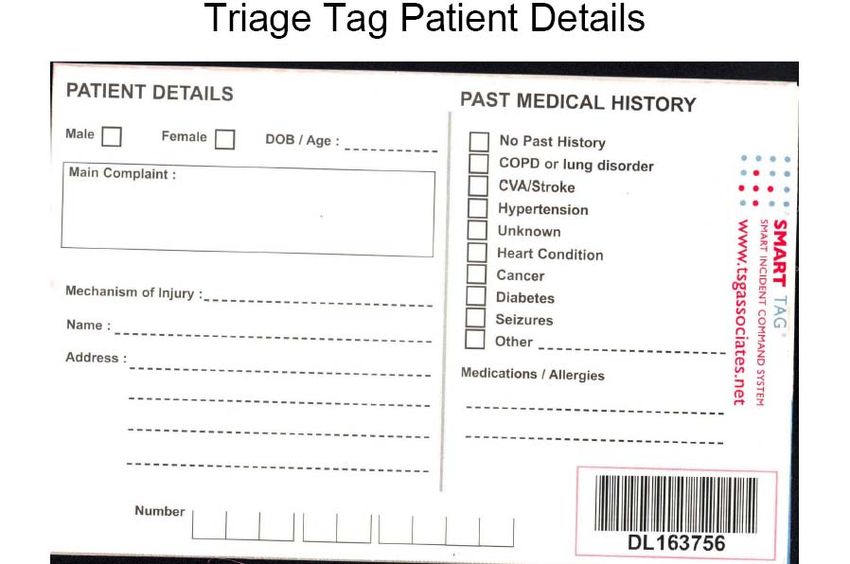
9 CO Emergencies
9 HAZMAT incidents
9 WMD
9 Multiple-shooting victims
9 Chemical exposure
Some of the above incidents can occur accidentally. Any of them can be intentionally
caused.
ICS CONSIDERATIONS
Mass casualties create the need for expansion of the ICS to include a Medical Sector
Officer to be appointed as soon as possible by the IC or Operations Officer. The Medical
Officer shall in turn designate as needed: Triage Team(s), Treatment Team(s), and a
Transport Officer within the ICS. If the incident is a HAZMAT or an intentional
chemical, biological or radiological release, etc, follow HAZMAT guidelines on
appropriate decon and level of protection. The steps below will be undertaken with the
4
appropriate level of personal protective equipment, and decon (if applicable) will be
performed on all affected victims per the HAZMAT team guidelines.
I. INITIAL TRIAGE
For the purpose of this module, we will be using the START triage model for adult
patients, JumpSTART Triage for pediatric patients and the SMART triage tagging
system. By using START triage, patients are objectively sorted on how they present. The
severity of injury, and, therefore, the treatment and/or transport priority in START triage
is sorted by color code. The tag is simply folded so that the color of the triage category is
exposed, then simply slip the tag back into the clear plastic pouch. SMART triage tags
contain large color fields so treatment and transport crews can easily see which patients
have been triaged to which level. For a flow chart of START triage (see figure 1 on pg.
9, and procedure 1 on pg. 8). Due to the nature of these incidents, it is likely that
properly trained responders with appropriate personal protective equipment (possibly
including self-contained breathing apparatus) will be providing initial triage. Those
lacking proper training and PPE will receive patients away from the hazardous area or
Hot Zone. These responders can set up and work in treatment zones.
Initial Triage can begin immediately after size-up but shall be done as soon as possible.
First in units may encounter non-injured and/or slightly injured victims self-evacuating
the area of the incident. These victims should be directed to an area of refuge and triage
tagged Green or “minor”. Qualified individuals should monitor those green-tagged
victims for any changes in their conditions.
The only interventions that are to be performed during initial triage are maintaining an
open airway and stopping uncontrolled bleeding. Other interventions can be performed
once initial triage is completed or after more personnel arrive.
II. PATIENT EXTRACTION
Patient extraction is the act of removing the remaining victims from the affected areas
and delivering them to designated treatment areas. Patient extraction can begin as soon as
resources on scene allow. Extraction can commence prior to the completion of initial
triage but shall begin as soon as initial triage has been completed or additional personnel
in proper PPE are available.
5
Patients that are tagged red or “immediate” are to be extracted first, followed by those
tagged yellow or “delayed” (green or “minor” patients most likely have self-extracted
already). Extraction is essential and all possible assistance should be sought. Cots and
litters are to be used for extraction when they are available. There may be private sector
items on the scene that can be employed to assist with patient extraction. Local response
teams have equipment to assist in extraction, but since these assets may not be
immediately available, they can be deployed to assist when they arrive. Deliver each
patient to the appropriate treatment area. Due to the nature of these incidents, many
hazards may still be present in the triage area. Regardless of the distance the treatment
areas are from the affected areas, victims shall be moved as carefully and as quickly as
those residual threats dictate.
Proper PPE shall be worn during extraction. The level of protection shall be equal to the
level necessary for the initial triage teams.
III. SECONDARY TRIAGE/TREATMENT
The nature of a mass casualty event suggests that the affected areas will not be a safe
place to establish treatment areas. Hazards may include chemical, biological or
radioactive contamination, unstable building components, secondary device threats, fire
involving structures and/or vehicles, limited space, utility issues, etc. The location of the
treatment areas will depend on these hazards and threats. If no additional hazard(s) exist,
the treatment areas can be established at or near the scene.
Treatment areas shall be established in safe locations so as not to interfere with other
units arriving for incident control. Treatment areas shall be marked with colored flags or
tarps. Treatment area locations shall also be easily accessible to transport vehicles
arriving from medical staging. In MCI incidents, a treatment area for each category of
patient (RED, YELLOW, GREEN) shall be established. Patients tagged BLACK shall
be left in place. Emergency medical equipment must be brought to the treatment areas to
support the treatment teams. Regional response teams have assets for MCI incidents and
they will be brought to the scene as soon as possible. Members of on-scene units being
used for medical treatment will need to use supplies carried on the apparatus until those
additional assets arrive. Each treatment area should have a secondary triage officer and a
treatment officer assigned by the Medical Officer, and it shall be staffed with adequate
treatment personnel.
All patients delivered to a treatment area will be re-triaged to affirm entrance into the
area. Patients with airway problems will be scheduled for immediate transport. The
patient’s triage category can be upgraded or downgraded by refolding the SMART triage
tag to expose the color field relating to their status. Patients being up-triaged or down-
triaged shall be moved to the appropriate treatment area.
Treatment for each patient will begin as soon as possible and will follow the local Patient
Care Protocols. All patients will be stabilized as soon as possible by individuals assigned
to treatment areas with available supplies and equipment. The SMART tag secondary
6
triage calculations identify the order of transport within the triage category (see figure 4
pg. 15, and Procedure 2 pg. 14). All treatment information will be logged on the triage
tag including known history, vital signs, assessments, interventions etc. (see figure 3 on
pg. 13).
IV. PATIENT TRANSPORT
Once sufficient Emergency Medical personnel are assigned to initial triage, patient
extraction, secondary triage, and treatment areas, subsequent responding transport units
and personnel re-assigned from completed tasks can assist in transport. Depending on the
size of the incident, the IC can request transport units other than Local FD Rescue Squads
from throughout the county. Transport units will report to Medical Staging and will be
assigned by the Staging Officer at the request of the Transport Officer. In large incidents,
an oversight communications agency may actually control the flow of patients to various
hospitals. The Transport Officer shall fill out and tear off the transport record on the
triage tag and keep it for future reference. Patients with minor illnesses/injuries may be
transported by unconventional means or mass transit such as local buses.
Note: Only decontaminated patients will be transported.
CONCLUSION: Any time the phone rings, it could be another false alarm, frequent
flyer, or faulty smoke detector in a business. It could also be something more urgent.
When the alarm sounds, no matter what the emergency, we will handle it. We hear a lot
about pre-plan, but what about post-plan? After the incident, and after critique, we can
look back and “post-plan” as if the incident were something more serious. For example,
we may have just responded to a two-car motor vehicle collision with three injured
occupants. We can mentally apply the START Triage rules to them after the fact. Would
they have been tagged red? Yellow? Decide how they would have been tagged, just for
practice. What if it were a serious bus accident with thirty patients? Where would
treatment areas have been set up? Where would the medical staging area have been
located? How would inclement weather have affected treatment area selection? Post-
planning incidents as if they could have been something more can serve as better
preparation for “the big one”.
See the attached figures and procedures.
7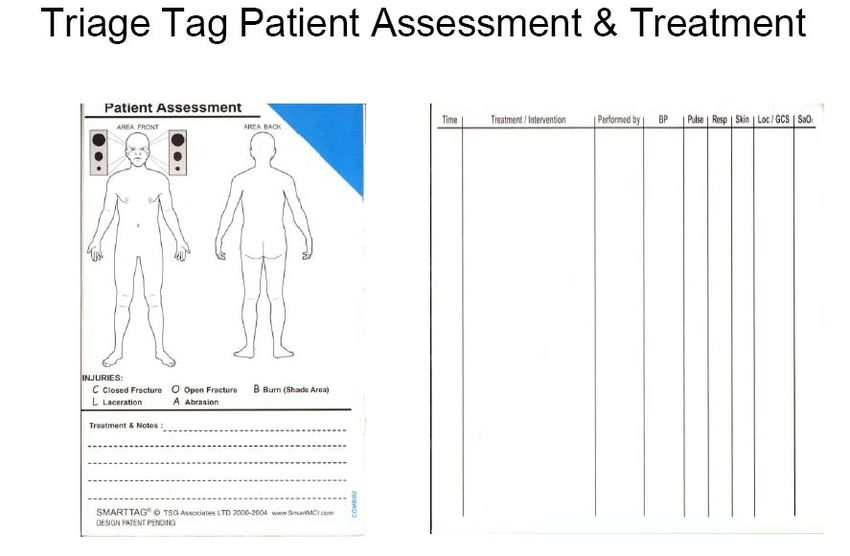
S.T.A.R.T. TRIAGE PROCEDURE (Adults)
The following procedure shall be used to sort casualties of Multiple or Mass Casualty incidents.
SMART triage tags and the S.T.A.R.T. triage system shall be used. JumpSTART shall be used
for pediatric patients and is covered below.
Code casualties by tag color.
GREEN Minor injury (walking wounded)
YELLOW Delayed- can wait
RED Immediate!
BLACK Dead
Require any victims who can self evacuate to do so. Call out “IF YOU CAN GET UP
AND GET OUT OF HERE DO SO NOW!” Direct them to an area of refuge for further
monitoring and placement of GREEN triage tags.
For the remaining non-ambulatory patients begin triage “where you stand” and move
systematically through the casualties. On each patient, first assess Respirations, followed
by Perfusion and then Mental status (RPM). Once a color tag can be assigned, place the
tag, stop your assessment and move on. The only interventions that are to be performed
during initial triage are maintaining an open airway and stopping uncontrolled bleeding
(Solicit capable bystanders to assist with this if available). Other interventions can be
performed once triage is completed or adequate personnel arrive.
Assess breathing.
o If absent, open the airway.
If respirations return, tag RED.
If respirations do not return, tag BLACK and move on.
o If breathing is present, assess the rate.
If greater than 30/min tag RED
If less than 30 move to assess perfusion
Assess perfusion
o Assess radial pulse
If absent, tag RED
If present, assess capillary refill (blanch test)
o Assess capillary refill
If greater than 2 seconds tag RED
If less than or equal to 2 seconds move to assess mental status
Assess mental status
o If patient cannot follow simple commands, tag RED
o If patient can follow simple commands, tag YELLOW
It’s that simple. Patients can easily be up-triaged or down-triaged if their conditions
change with SMART triage tags.
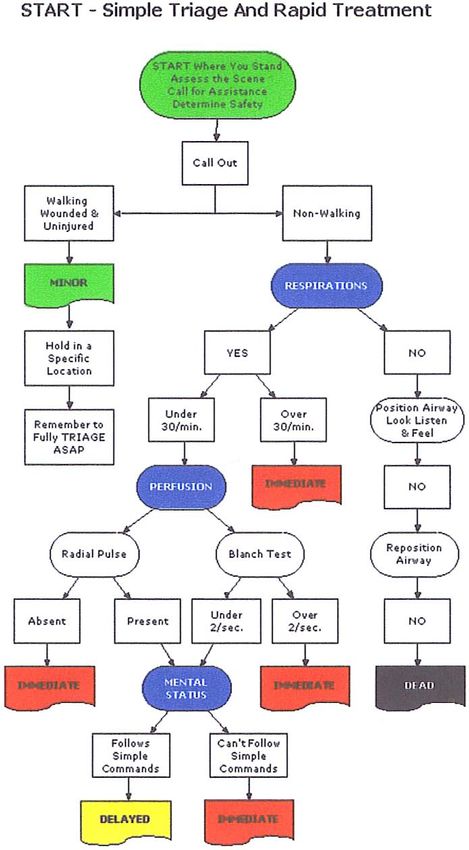
Procedure 1, START Triage
8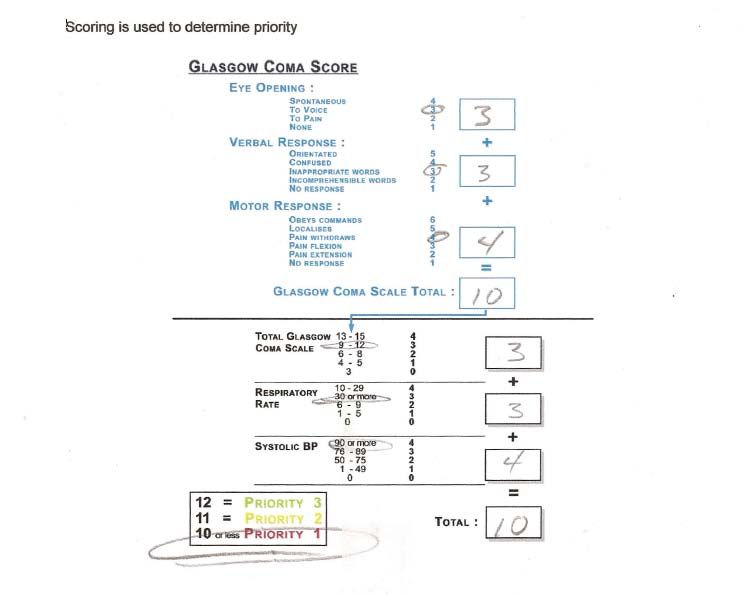
Figure 1) Start triage algorithm
9
JUMPSTART, PEDIATRIC PATIENT MCI TRIAGE
JumpSTART is an objective pediatric patient MCI triage tool developed specifically for
the triage of children in the multi-casualty/disaster setting. JumpSTART was developed
in 1995 to be used along with the START triage system and mirrors the structure.
JumpSTART objectives:
1. Optimize initial triage of children in the MCI setting
2. Enhance the effectiveness of resource allocation for all MCI victims
3. Reduce emotional burden on personnel assigned to initial the triage of
children
JumpSTART provides an objective structure to help assure responders triage injured
children with their heads, not their hearts. This can reduce the possible over-triage that
may siphon resources away from other patients who may need them more, and result in
physical and emotional trauma to children from unnecessary painful procedures and
separation from loved ones. Under-triage is addressed as well by recognizing key
differences between adult and pediatric physiology, and using appropriate pediatric
physiological parameters at triage decision points.
JumpSTART is rapidly gaining popularity and has become widely accepted in many
national and state venues. It has also been incorporated into pediatric education and is
included in the curriculum of Advanced Pediatric Life Support (APLS) and Pediatric
Disaster Life Support (PDLS).
Note: JumpSTART was designed ONLY to be used in the MCI/disaster setting not for
routine EMS or hospital triage.
See JumpSTART algorithm (Figure 2 on page 11)
10Figure 2) JumpSTART
11The SMART TRIAGE TAG
The SMART tag provides perforated sections to simplify the categorization of victims.
The codes include:
1. Colors
2. Numbers
3. Symbols
Triaging, or “sorting” victims into using these categories will allow you to arrive at
treatment and transport priority decisions.
Once the appropriate category is determined, the tag is placed to the patient in the plastic
pouch. The tag is folded so the color corresponding to the victim’s triage category is
visible.
Information that will be filled in on various sections of the tag includes:
1. Time and date
2. Victim’s name and address
3. Vitals signs
4. Interventions
5. Medications
6. Chief complaint
7. MOI
8. Past medical history
9. etc
The transport officer tears off the perforated transport record and enters the transport
destination and personal identifiers on the torn off section. The transport officer retains
the torn off portion while the tag accompanies the patient.
The SMART Tag is usable in all conditions and will provide a permanent patient record.
The tags contain bar codes for scan tracking (if available to your department) and is
resistant to water, chemicals, bodily fluids etc. There are also WMD/HAZMAT tags
available as well.
12Figure 3) Triage tag data entry fields
13SECONDARY TRIAGE CALCULATOR PROCEDURE
The following procedure will be used to establish the order of hospital transport during
Mass Casualty Incidents.
Casualties with airway problems shall be transported first.
The transport order of the remaining patients will be determined using the SMART triage
tag secondary triage calculator by the following:
¾ Assess Glasgow Coma Score (GCS), respiratory rate and BP
o Assign the appropriate numerical value for the GCS
o Assign the appropriate numerical value for the respiratory rate
o Assign the appropriate numerical value for Systolic BP
Add these values together to determine transport priority 1, 2 or 3 within the triage
category.
Procedure 2) Secondary Triage Calculator
14Figure 4) SMART Triage tag secondary triage calculator
15THIS PAGE INTENTIONALLY BLANK
16You can also read