Does This Patient Have Generalized Anxiety or Panic Disorder? The Rational Clinical Examination Systematic Review
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Review & Education
The Rational Clinical Examination
Does This Patient Have Generalized Anxiety
or Panic Disorder?
The Rational Clinical Examination Systematic Review
Nathaniel R. Herr, PhD; John W. Williams Jr, MD, MHSc; Sophiya Benjamin, MD; Jennifer McDuffie, PhD
Supplemental content at
IMPORTANCE In primary care settings, generalized anxiety disorder (GAD) and panic disorder jama.com
are common but underrecognized illnesses. Identifying accurate and feasible screening CME Quiz at
instruments for GAD and panic disorder has the potential to improve detection and facilitate jamanetworkcme.com and
treatment. CME Questions page 89
OBJECTIVE To systematically review the accuracy of self-report screening instruments in
diagnosing GAD and panic disorder in adults.
DATA SOURCES We searched MEDLINE, PsycINFO, and the Cochrane Library for relevant
articles published from 1980 through April 2014.
STUDY SELECTION Prospective studies of diagnostic accuracy that compared a self-report
screening instrument for GAD or panic disorder with the diagnosis made by a trained clinician
using Diagnostic and Statistical Manual of Mental Disorders or International Classification of
Diseases criteria.
Author Affiliations: Department of
Psychology, American University,
RESULTS We screened 3605 titles, excluded 3529, and performed a more detailed review of Washington, DC (Herr); Durham
76 articles. We identified 9 screening instruments based on 13 articles from 10 unique studies Veterans Affairs Evidence-based
Synthesis Program (ESP) Center,
for the detection of GAD and panic disorder in primary care patients Across all studies,
Durham, North Carolina (Williams,
diagnostic interviews determined that 257 of 2785 patients assessed had a diagnosis of GAD McDuffie); Duke University
while 224 of 2637 patients assessed had a diagnosis of panic disorder. The best-performing Department of Medicine, Durham,
test for GAD was the Generalized Anxiety Disorder Scale 7 Item (GAD-7), with a positive North Carolina (Williams, McDuffie);
Grand River Hospital, Kitchener,
likelihood ratio of 5.1 (95% CI, 4.3-6.0) and a negative likelihood ratio of 0.13 (95% CI, Ontario, Canada (Benjamin);
0.07-0.25). The best-performing test for panic disorder was the Patient Health Department of Psychiatry and
Questionnaire, with a positive likelihood ratio of 78 (95% CI, 29-210) and a negative Behavioral Neurosciences, McMaster
University, Hamilton, Ontario, Canada
likelihood ratio of 0.20 (95% CI, 0.11-0.37).
(Benjamin).
Corresponding Author: John W.
CONCLUSIONS AND RELEVANCE Two screening instruments, the GAD-7 for GAD and the Williams Jr, MD, MHSc, 411 W Chapel
Patient Health Questionnaire for panic disorder, have good performance characteristics and Hill St, Ste 500, Durham, NC 27701
are feasible for use in primary care. However, further validation of these instruments is (jw.williams@duke.edu).
needed because neither instrument was replicated in more than 1 primary care population. Section Editors: David L. Simel, MD,
MHS, Durham Veterans Affairs
Medical Center and Duke University
JAMA. 2014;312(1):78-84. doi:10.1001/jama.2014.5950 Medical Center, Durham, NC; Edward
H. Livingston, MD, Deputy Editor.
to determine whether Ms B’s symptoms and related behaviors in-
Clinical Scenario dicate an anxiety disorder?
Ms B is a 42-year-old computer programmer with a history of irri-
table bowel syndrome who presents to her primary care physician
Why Is This Question Important?
for a blood pressure check. Six months ago, she began caring for her
chronically ill mother, and she reports increased stress. You note that Anxiety disorders are prevalent, are often chronic, cause impor-
she had a visit to urgent care after having transient chest pain, short- tant functional impairment, and are associated with increased health
ness of breath, and palpitations. Myocardial ischemia was ruled out care use.1,2 Two of the more common anxiety disorders are gener-
without requiring hospital admission. Female sex, stressful life alized anxiety disorder (GAD) and panic disorder. In community
events, and chronic medical illness place her at increased risk for an samples, the estimated lifetime prevalence rates for GAD and panic
anxiety disorder. What tools could be used by the physician or nurse disorder are 5.1% and 3.5%, respectively, and 12-month rates (ex-
78 JAMA July 2, 2014 Volume 312, Number 1 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014Screening for Generalized Anxiety or Panic Disorder The Rational Clinical Examination Clinical Review & Education
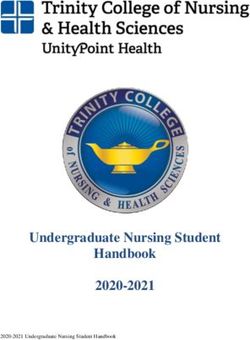
Table 1. Diagnostic Criteria for Generalized Anxiety and Panic Disordera
Main Symptoms Associated Symptoms Functional Qualifier Exclusions
GAD (DSM-5)
Excessive worry and difficulty controlling worry Individuals with GAD often experience Significant Not due to another Axis I illness,
for at least 6 mo Trembling/shakiness impairment in medical illness, or substance
≥3 of the following symptoms: Muscle aches functioning (drug of abuse or medication)
Restlessness Sweating/nausea/diarrhea
Easily fatigued Irritable bowel
Irritability Headaches
Difficulty concentrating
Muscle tension
Sleep disturbance
Panic Disorder (DSM-5)
Recurrent and unexpected panic attacks Panic attacks are an abrupt surge in Significant Not due to another Axis I illness,
At least 1 mo of ≥1 of the following symptoms: symptoms, including impairment in medical illness, or substance
Persistent concern about having another attack Palpitations functioning (drug of abuse or medication)
Significant maladaptive change in behavior Sweating
related to attacks Trembling/shaking
Shortness of breath/choking
Chest pain
Nausea
Dizziness
Chills/heat sensations
Paresthesias
Derealization
Fear of losing control
Fear of dying
Abbreviations: DSM, Diagnostic and Statistical Manual of Mental Disorders; GAD, exception: the DSM-5 no longer asks diagnosticians to determine whether
generalized anxiety disorder. panic disorder is with or without agoraphobia.
a
The DSM-5 criteria for these disorders are identical to those of DSM-IV, with 1
perienced anytime within the last 12 months, including currently) are ing; shortness of breath; feeling of choking; chest pain or discom-
3.1% and 2.3%, respectively.3 Primary care patients have higher rates fort; nausea or abdominal distress; feeling dizzy, unsteady, light-
of both GAD (8%) and panic disorder (6.8%), and the prevalence headed, or faint; paresthesias; chills; or hot flushes.8 Although
rate of GAD increases to 22% among those with anxiety problems agoraphobia was previously considered to be a subtype within the
as the presenting concern.4,5 Many patients with anxiety disorders panic disorder diagnosis, in the Diagnostic and Statistical Manual of
present to their primary care physician with somatic symptoms, Mental Disorders (Fifth Edition) (DSM-5) it is now classified as a dis-
which contributes to underrecognition of these conditions and can crete disorder characterized by avoidance of public spaces for fear
result in unnecessary and costly diagnostic testing.6 When diag- of having a panic attack.
nosed, both GAD and panic disorder can be treated successfully with A clinical evaluation of anxiety disorders can begin with an open-
medication and/or psychotherapy. Furthermore, care manage- ended question such as “Tell me about your worries, fears, con-
ment trials have shown that screening, coupled with effective pri- cerns, and stresses, and how they affect you.”9 When GAD is in-
mary care treatment, improves outcomes for patients with anxiety quired about specifically, a question such as “Would you say that you
disorders.7 have been bothered by ‘nerves’ or feeling anxious or on edge?” can
elicit symptoms of the disorder. When inquiring about panic disor-
der specifically, the clinician can ask a question such as “Did you ever
have a spell or an attack when all of a sudden you felt frightened,
How to Diagnose GAD and Panic Disorder
anxious, or very uneasy?”10
Anxiety symptoms such as worry or physical tension are experi- Another approach to the diagnosis of GAD and panic disorder
enced nearly universally in response to stressful or threatening situ- in primary care clinics is to ask all patients, or those with risk fac-
ations. Anxiety may be an adaptive emotional experience that helps tors, to complete a self-report screening instrument. Depending on
a person to avoid or prepare for future challenges. In contrast, anxi- the prevalence of the disease, the physician may want to optimize
ety disorders cause severe and persistent symptoms that impair func- the positive likelihood ratio (LR+) to avoid unnecessary additional
tioning. The criterion standards for GAD and panic disorder are sum- testing or the negative likelihood ratio (LR−) to be confident that anxi-
marized in Table 1. Generalized anxiety disorder is characterized by ety disorders do not require additional consideration. An alterna-
at least 6 months of persistent, excessive anxiety or worry that is tive as part of the initial diagnostic assessment would be to evalu-
difficult to control and causes significant distress or impairment. The ate only patients who present with symptoms that raise suspicion
diagnosis requires at least 3 of 6 additional symptoms: restless- of an anxiety disorder. For routine use in primary care settings, the
ness, fatigue, irritability, decreased concentration, muscle tension, ideal instrument should be brief, accurate, easy to score and inter-
and sleep disturbance.8 Panic disorder is characterized by fre- pret, and studied in mixed populations of patients. For patients with
quent and unexpected panic attacks, and individuals with this dis- a positive screening result, a careful clinical interview coupled with
order exhibit intense worry about having them. Panic attacks are pe- a targeted physical examination and any indicated diagnostic test-
riods of intense fear or terror associated with autonomic arousal, and ing to evaluate for an underlying explanatory medical illness is re-
typical symptoms include palpitations; sweating; trembling or shak- quired for a definitive diagnosis. To inform decision making regard-
jama.com JAMA July 2, 2014 Volume 312, Number 1 79
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014Clinical Review & Education The Rational Clinical Examination Screening for Generalized Anxiety or Panic Disorder
ing a standard instrument to assess primary care patients for anxiety Statistical Methods
disorders, we conducted a systematic review of the literature to Sensitivity, specificity, and likelihood ratios (LRs) were calculated with
evaluate the performance of self-report instruments used to diag- CIs for instruments evaluated in each study. An LR+ is the ratio of
nose GAD and panic disorder in primary care settings. the likelihood of a positive test result in an individual with the con-
dition to the likelihood of a positive test result in an individual with-
out it. An LR− is the ratio of the likelihood of a negative test result in
an individual with the condition to the likelihood of a negative test
Methods
result in an individual without it. Tests with higher specificity gen-
Search Strategy and Study Selection erally have higher LRs, and positive results are most useful for iden-
We searched MEDLINE, PsycINFO, and the Cochrane Library from tifying patients with an anxiety disorder, whereas tests with higher
January 1980 through April 2014 for studies conducted in general sensitivity generally have lower LRs, and negative results are most
medical settings that compared a self-report instrument with an ac- useful for ruling out patients who do not have an anxiety disorder.
ceptable criterion standard. The search strategy included the terms If an LR+ is 2, a positive test result (in this case, a positive score on
generalized anxiety disorder and panic disorder, the names of an anxiety questionnaire) is twice as likely to occur in an individual
anxiety instruments, and a validated search filter for retrieving with an anxiety disorder as opposed to an individual without one.
articles on the diagnosis of health disorders (eAppendix 1 in the An LR− of 0.2 means that a negative screening result is one-fifth as
Supplement).11,12 Electronic searches were supplemented by exam- likely to occur in an individual with an anxiety disorder as opposed
ining the bibliographies of systematic reviews, a recent technical re- to an individual without one. Because GAD and panic disorder are 2
port, and the studies we ultimately included in the technical report.13 distinct clinical entities, we calculated summary estimates sepa-
We included studies that were conducted with patients aged rately for studies on GAD-specific instruments and panic disorder–
at least 18 years who were treated in general medical settings (ie, specific instruments.
general internal medicine, family medicine, geriatrics, emergency To estimate the prior probability of GAD and panic disorder, we
department, and women’s health clinic); compared self-report calculated a random-effects summary measure from the included
questionnaires for GAD or panic disorder with diagnostic inter- studies. The Symptom Driven Diagnostic System for Primary Care
views, using criteria from either the Diagnostic and Statistical (SDDS-PC) instrument was evaluated in 3 studies, which allowed us
Manual of Mental Disorders (Third Edition) (DSM-III) or Interna- to calculate separate summary measures for the sensitivity, speci-
tional Classification of Diseases, Ninth Revision, or more recent ficity, and LR with 95% CI. All other instruments were evaluated in
editions of these publications; and were peer-reviewed, English- only 1 study, for which we show the test’s point estimate and 95%
language publications from North America, western Europe, New CI. We explored heterogeneity among the studies with Cochran Q
Zealand, or Australia. Geographic and language limitations were and I2, which describe the percentage of total variation across stud-
designed to identify studies with the highest applicability to US ies due to heterogeneity rather than chance, and we used meta-
populations. Two reviewers independently examined each regression to evaluate the effect of age and sex on the LRs. Hetero-
abstract for relevance. Next, full-text articles identified by either geneity was categorized as low, moderate, or high according to I2
reviewer as potentially relevant were examined by 2 reviewers, values of 25%, 50%, and 75%, respectively. We used Comprehen-
who evaluated the articles’ eligibility according to predetermined sive Meta-Analysis (Biostat version 2.2.064) for all meta-analyses.
criteria (eAppendix 2 in the Supplement). Disagreements were
resolved by discussion or a third reviewer.
Results
Data Abstraction and Quality Ratings
We extracted selected data elements informed by the principles out- Study Characteristics
lined by the Standards for Reporting of Diagnostic Accuracy.14 These We identified 3605 unique citations from a combined electronic
elements included descriptors to assess applicability (eg, setting, search of MEDLINE via PubMed (n = 1167), PsycINFO (n = 1810), and
sample characteristics, anxiety disorder prevalence), test perfor- the Cochrane Library (n = 605) and from a manual examination of
mance, and quality (eg, recruitment method, blinding, reference references (n = 23). After inclusion and exclusion criteria were ap-
standard, sample size) of each study. When provided, raw data for plied, 3529 articles were excluded at the title and abstract level. We
the 2 × 2 table were extracted, and when not provided, data were retrieved 76 articles for full-text review and excluded 63. For data
derived from other performance characteristics such as sensitivity abstraction and evidence synthesis, we retained a total of 13 ar-
and specificity. When results were adjusted for the sampling de- ticles representing 10 unique studies.16-25 Because some studies in-
sign (eg, partial verification of the criterion-based diagnosis), we use cluded more than 1 sample or evaluated more than 1 instrument, we
the adjusted results. A second reviewer verified all data abstrac- included 14 unique evaluations of anxiety instruments. The eFigure
tions, and disagreements were resolved by reviewer discussion or in the Supplement illustrates the literature search process.
by obtaining a third reviewer’s opinion. Of 13 articles describing 10 studies, 9 different instruments were
For each selected study, raters completed the Quality Assess- evaluated (Table 2). Across all studies, diagnostic interviews deter-
ment of Diagnostic Accuracy Studies, a 14-item tool that assesses mined that 257 of 2785 patients assessed had a diagnosis of GAD
study quality (eAppendixes 3-4 in the Supplement). We followed rec- while 224 of 2637 patients assessed had a diagnosis of panic disor-
ommendations from The Rational Clinical Examination series15 by der. The average age of patients in studies of GAD (n = 6) (Table 3)
assigning a level of evidence for each study, ranging from I (high qual- was similar across 5 of the samples18,21,23,25 (range, 38-47 years),
ity) to V (low quality). whereas 1 study20 contained older patients (mean age, 73 years).
80 JAMA July 2, 2014 Volume 312, Number 1 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014Screening for Generalized Anxiety or Panic Disorder The Rational Clinical Examination Clinical Review & Education
Table 2. Characteristics of 8 Self-report Measures for Generalized Anxiety and Panic Disorder
No. of Time Score Usual Cut Literacy Tracking of
Instrument Items Response Format Frame Range Point Levelsa Completion Time Symptoms
GAD
ADS-GA26 11 Yes or no Unknown 0-11 4-5 Easy Unknown Unknown
GAD-723 7 4 Frequency ratings: 2 wk 0-21 5 = mild Average Unknown Unknown
not at all, several days, 10 = moderate
more than half the days, 15 = severe
nearly every day
GAD-Q-IV25 9 5 Yes or no; 2 Likert 6 mo 0-12 ≥5.7 Average Unknown Unknown
(9 response choices);
1 count of worries;
1 physical symptom
checklist
SDDS-PC18 4 GAD Yes or no 6 mo 0-5 Unclear EasyClinical Review & Education The Rational Clinical Examination Screening for Generalized Anxiety or Panic Disorder
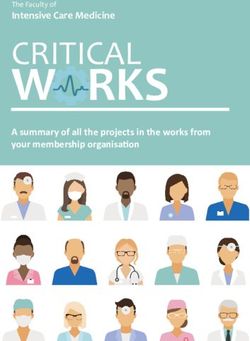
Table 3. Performance Characteristics of Self-report Instruments
(95% CI)
No. (% Age, Mean Quality
Instrument Study Prevalence)a (SD), y Females, % Sensitivity Specificity LR+ LR– Rating
GAD
GAD-7 Spitzer et al,23 2006 965 (7.6) 47 (16) 65 0.89 0.83 5.1 0.13 I
(0.82-0.96) (0.80-0.85) (4.3-6.0) (0.07-0.26)
GAD-Q-IV Moore et al,25 2014 99 (27) 39 (13) 85 0.89 0.63 2.4 0.18 III
(0.77-1.0) (0.51-0.74) (1.7-3.3) (0.1-0.5)
20
ADS-GA Krasucki et al, 1999 88 (15) 73 64 0.39 0.88 3.2 0.70 III
(0.12-0.65) (0.81-0.95) (1.3-8.0) (0.45-1.08)
SDDS-PC Leon et al,21 1996 501 (16) 49 (13) 66 0.74 0.82 4.1 0.32 I
(0.64-0.83) (0.78-0.86) (3.2-5.2) (0.22-0.46)
18
Broadhead et al, 257 (5.4) 40 (13) 79 0.92 0.54 2.0 0.15 I
1995 (0.76-1.00) (0.49-0.59) (1.6-2.4) (0.02-1.01)
Broadhead et al,18 388 (3.1) 39 (12) 73 0.86 0.60 2.1 0.24 I
1995 (0.67-1.00) (0.53-0.66) (1.6-2.8) (0.07-0.87)
Summary SDDS-PC 0.78 0.67 2.6 0.31
(0.66-0.87) (0.47-0.82) (1.6-4.1) (0.22-0.43)
Panic Disorder
PHQ Spitzer et al,22 1999 585 (6.0) 46 (17) 66 0.81 0.99 78 0.20 I
(0.68-0.93) (0.98-1.00) (29-210) (0.11-0.37)
SDDS-PC Leon et al,21 1996 501 (8.0) 49 (13) 66 0.70 0.91 7.9 0.33
(0.56-0.84) (0.88-0.93) (5.5-11) (0.20-0.53)
Broadhead et al,18 257 (6.2) 40 (13) 79 0.78 0.80 3.9 0.28 I
1995 (0.62-0.94) (0.76-0.84) (2.9-5.2) (0.14-0.56)
Broadhead et al,18 388 (7.0) 39 (12) 73 0.63 0.83 3.8 0.45 I
1995 (0.39-0.86) (0.78- 0.88) (2.3-6.0) (0.23-0.70)
Summary SDDS-PC 0.71 0.86 4.9 0.35
(0.60-0.80) (0.77-0.91) (3.0-7.9) (0.25-0.48)
10-Item scale Barsky et al,16 1997 124 (26) 47 57 0.72 0.71 2.4 0.40 II
(0.56-0.88) (0.60-0.80) (1.7-3.6) (0.22-0.70)
19
BPDS Johnson et al, 2007 295 (14) 54 (11) 66 0.61 0.29 0.86 1.36 I
(0.46-0.76) (0.23-0.35) (0.66-1.1) (0.88-2.08)
GAD or Panic Disorder
BAI-PC Beck et al,17 1997 56 (23) 49 (16) 73 0.85 0.81 4.6 0.19 III
(0.65-1.00) (0.67-0.92) (2.3-8.9) (0.05-0.68)
PRIME-MD Spitzer et al,24 1994 431 (18) 55 (16) 60 0.93 0.53 2.0 0.12 I
(0.88-0.99) (0.48-0.58) (1.8-2.3) (0.05-0.29)
Abbreviations: ADS-GA, Anxiety Disorder Scale–Generalized Anxiety; BAI-PC, All studies were conducted in primary care with unselected participants, except
Beck Anxiety Inventory–Primary Care; BPDS, Brief Panic Disorder Screen; GAD, that by Barsky et al,16 which was conducted at a specialty clinic and selected
generalized anxiety disorder; GAD-Q-IV, Generalized Anxiety Disorder patients presenting with heart palpitations.
Questionnaire Fourth Edition; GAD-7, Generalized Anxiety Disorder Scale 7 Item; a
Reported Ns were calculated according to the number of patients who
LR, likelihood ratio; PHQ, Patient Health Questionnaire; PRIME-MD, Primary completed the criterion standard and not the number enrolled in the study;
Care Evaluation of Mental Disorders; SDDS-PC, Symptom Driven Diagnostic age is reported as mean (standard deviation).
System for Primary Care.
yielded similar diagnostic accuracy results across the sex distribu- includes a brief depression module previously found to have high
tion of the studies we evaluated (range female, 64% to 85%). sensitivity and specificity for diagnosing depression.28
The 4 instruments had high heterogeneity for the LR+ (I2, 92%;
Panic Disorder P < .001), but the LR− showed low heterogeneity (I2, 14%; P = .32).
We assessed the heterogeneity of 4 of the 6 studies for identifying In a meta-regression, age was not associated with the summary LR+
patients with panic disorder. One study16 was not included be- (R2, 0), suggesting that the results are similar in the age range we
cause it assessed patients with palpitations who presented to spe- evaluated (mean age range 39 to 54 years). The meta-regression
cialists rather than unselected patients presenting to a primary care showed that the summary LR+ accounted for a small amount of the
provider. A second study19 was not included because it had no di- variability in the LR+ (R2, 15%; P = .03).
agnostic utility (both LR CIs included 1), so it could not classify the
presence or absence of panic disorder. Combined Screening for GAD and Panic Disorder
The Patient Health Questionnaire (PHQ), using a positive re- For identifying patients who may have either GAD or panic disorder,
sponse to all 5 questions, had good sensitivity (81%) and specificity the Beck Anxiety Inventory–Primary Care performed well compared
(99%), the best LR+ (78; 95% CI, 29-210), and the best LR− (0.20; with other instruments, with an LR+ of 4.6 (95% CI, 2.3-8.9) and an
95% CI, 0.11-0.37). The PHQ requires less than 1 minute for comple- LR− of 0.19 (95% CI, 0.05-0.68). The instrument has an easy literacy
tion and has an easy literacy level. The SDDS-PC is also efficient, with and can be completed quickly (approximately 1 minute). An alterna-
a summary LR+ of 4.9 (95% CI, 3.0-7.9) and summary LR− of 0.35 tive combined instrument, the Primary Care Evaluation of Mental Dis-
(95% CI, 0.25-0.48). An additional advantage of the PHQ is that it orders, has the fewest number of questions for the patient (3), short
82 JAMA July 2, 2014 Volume 312, Number 1 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014Screening for Generalized Anxiety or Panic Disorder The Rational Clinical Examination Clinical Review & Education
completion time (1 minute), and easy literacy level. At a threshold score moreethnicallydiversesamplestobetterdeterminehowthesescreen-
of less than or equal to 1 question with a positive response, individu- ing measures perform in different subgroups.
als with no positive responses have the lowest LR− with the narrow-
est CI for either anxiety disorder (LR−, 0.12; 95% CI, 0.05-0.29). How to Learn a Method for Diagnosing GAD
and Panic Disorder
Both the GAD-7 and PHQ screening instruments are available on-
line (www.phqscreeners.com) and have been translated into many
Discussion
languages. Because both of these instruments are self-
We found that 2 screening instruments, GAD-7 for GAD and the PHQ administered, minimal clinician training is needed to administer them.
for panic disorder, have good performance characteristics and are Additional advantages of GAD-7 are that it has good operating char-
feasible for use in primary care. Further validation of these instru- acteristics in a 2-item abbreviated version (the GAD-2) and in screen-
ments is needed because neither instrument was replicated in more ing for anxiety disorders other than GAD.4 A manual for scoring both
than 1 primary care population. instruments is also available online. All of the instruments included
in this review are for screening or case-finding purposes and do not
Study Strengths diagnose GAD or panic disorder. Although these instruments may
This study was a highly structured and systematic review of the ex- be used as part of the initial diagnostic evaluation, a criterion-
tant evidence. Our evidence synthesis was guided by a carefully de- based diagnosis must be established through further evaluation by
signed standardized protocol, including a systematic search of re- a primary care physician or by a mental health professional to whom
search databases and relevant bibliographies, double data the patient is referred. Such confirmation should be determined by
abstraction, and use of validated criteria to assess the quality of iden- follow-up questions based on the DSM-5 (outlined in Table 1) and
tified studies. Our multidisciplinary team included expertise in in- should rule out psychiatric disorders with related symptoms (eg,
ternal medicine, primary care, psychiatry, and psychology. Our search posttraumatic stress disorder, depression) and medical causes of
identified a large number of anxiety screening instruments, but few symptoms suggestive of anxiety. The studies we reviewed used DSM-
had been studied in primary care populations. These instruments III or DSM-IV diagnostic criteria for GAD and panic disorder; no sig-
had moderate to good operating characteristics, but unlike instru- nificant changes in these criteria were introduced in DSM-5.
ments used in the detection of other common mental illnesses such
as depression or dementia, the operating characteristics have not Treatment
been replicated in multiple samples. Even for the SDDS-PC—the only Screening alone is not sufficient to ensure that patients with anxi-
instrument evaluated in multiple studies—the versions studied were ety disorders in the primary care setting receive appropriate treat-
different, which might change the test performance. ment. Although referring a patient for a psychiatric evaluation is one
option, primary care physicians should also familiarize themselves
Study Limitations with the diagnostic criteria for GAD and panic disorder, as well as with
In most studies, threshold values for the screening instrument were pharmacologic and other treatments for these disorders that are ap-
specified after analysis of results instead of before. Thus, replication propriate for primary care. Collaborative care models integrating psy-
is needed to validate the cutoffs recommended in these studies. Ad- chiatric treatment in the primary care setting have also been shown
ditionally, many of the studies did not confirm the diagnosis with the to be effective for anxiety disorders.7 Furthermore, because there
referencestandardinallpatients,orinarandomsampleofthem,which is symptom overlap between GAD or panic disorder and other psy-
could introduce partial verification bias. A further limitation is the lack chiatric diagnoses, false-positive results on any of these screening
of studies reporting on patient outcomes and societal influence. This instruments may be not only “true” false-positives (ie, when the pa-
lack of important patient outcomes has been recognized as a chal- tient meets the criteria for no related diagnoses) but also due to the
lenge in systematic reviews of diagnostic tests.29 Because our eligibil- presence of a related psychiatric disorder. As such, a positive screen-
ity criteria were designed to exclude poor-quality studies (ie, studies ing result, even if it is a false-positive for GAD or panic disorder, may
in which the same person conducted the screening and criterion stan- indicate the need for further evaluation of the patient.
dard), we may have excluded studies that could provide low-level evi-
dence on the topic. Furthermore, one of the better-performing mea- Scenario Resolution
sures, the Beck Anxiety Inventory–Primary Care, was tested in a very You observe that Ms B has important risk factors for an anxiety dis-
small sample (n = 56) and that study17 was rated as having a higher risk order, and her trip to urgent care suggests a possible panic attack.
of bias (quality rating = III). A solution to these issues is to encourage You decide that in addition to checking her blood pressure, you will
future high-quality validation studies, which are notably absent de- conduct case-finding for GAD and panic disorders. You administer
spite that many of them were published almost 20 years ago. The cri- the GAD-7 and PHQ, wherein she scores 12 on the GAD-7 and an-
terion standard for GAD and panic disorder has not changed appre- swers no to the PHQ item about anxiety attacks. With a pretest prob-
ciably in that time, and thus the performance characteristics of these ability of 20% for GAD (based on an estimate of twice the preva-
measures remain applicable to current diagnoses. Finally, these stud- lence in unselected primary care patients) and a GAD-7 LR+ of 5.1,
ies were not designed to address differing performance in sub- Ms B. has a 59% probability of having GAD. After discussing op-
groups, so our evaluation of age and sex as explanations for varying tions for evaluation and treatment, you refer her for a psychiatric
performance is based on a small number of studies, uses indirect com- evaluation in which her condition may be diagnosed and treated with
parisons, and should be considered exploratory. Indeed, future stud- empirically supported treatments such as cognitive behavioral
ies would benefit from the inclusion of older patients (>65 years) and therapy or an appropriate pharmacotherapy.
jama.com JAMA July 2, 2014 Volume 312, Number 1 83
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014Clinical Review & Education The Rational Clinical Examination Screening for Generalized Anxiety or Panic Disorder
it assesses both conditions with relatively few questions. For clini-
Bottom Line cal practices that opt for patient-completed screening instru-
ments (eg, in the waiting room), the Primary Care Evaluation of
There are several promising case-finding instruments with good Mental Disorders shows promise for identifying anxiety that
performance characteristics for GAD and panic disorder in pri- might prompt additional questions during an examination. Fur-
mary care populations. In particular, the GAD-7 and PHQ stand ther replication of these initial validation studies, in particular
out as the most efficient instruments, whereas the SDDS-PC may with samples of older and more ethnically diverse patients, is
be an adequate alternative when a fast screen is desired because needed in primary care settings.
ARTICLE INFORMATION unrecognized anxiety disorders and major depressive 15. Simel DL. Update: primer on precision and
Author Contributions: Dr Williams had full access disorder. J Affect Disord. 1997;43(2):105-119. accuracy. In: Simel DL, Rennie D, Keitz SA, eds. The
to all of the data in the study and takes 3. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime Rational Clinical Examination: Evidence-Based Clinical
responsibility for the integrity of the data and the and 12-month prevalence of DSM-III-R psychiatric Diagnosis. New York, NY: McGraw Hill; 2009:9-16.
accuracy of the data analysis. disorders in the United States: results from the 16. Barsky AJ, Ahern DK, Delamater BA, Clancy SA,
Study concept and design: Williams, Benjamin, National Comorbidity Survey. Arch Gen Psychiatry. Bailey ED. Differential diagnosis of palpitations:
McDuffie. 1994;51(1):8-19. preliminary development of a screening
Acquisition, analysis, or interpretation of data: All 4. Kroenke K, Spitzer RL, Williams JB, Monahan instrument. Arch Fam Med. 1997;6(3):241-245.
authors. PO, Löwe B. Anxiety disorders in primary care: 17. Beck AT, Steer RA, Ball R, Ciervo CA, Kabat M.
Drafting of the manuscript: Herr, Benjamin, McDuffie. prevalence, impairment, comorbidity, and Use of the Beck Anxiety and Depression Inventories
Critical revision of the manuscript for important detection. Ann Intern Med. 2007;146(5):317-325. for primary care with medical outpatients.
intellectual content: Herr, Williams, Benjamin. Assessment. 1997;4(3):211-219.
Statistical analysis: Herr, Williams, Benjamin. 5. Wittchen HU. Generalized anxiety disorder:
Obtained funding: Williams. prevalence, burden, and cost to society. Depress 18. Broadhead WE, Leon AC, Weissman MM, et al.
Administrative, technical, or material support: Herr, Anxiety. 2002;16(4):162-171. Development and validation of the SDDS-PC screen
McDuffie. 6. Zaubler TS, Katon W. Panic disorder in the general for multiple mental disorders in primary care. Arch
Study supervision: Williams. medical setting. J Psychosom Res. 1998;44(1):25-42. Fam Med. 1995;4(3):211-219.
Conflict of Interest Disclosures: All authors have 7. Woltmann E, Grogan-Kaylor A, Perron B, et al. 19. Johnson MR, Hartzema AG, Mills TL, et al. Ethnic
completed and submitted the ICMJE Form for Comparative effectiveness of collaborative chronic differences in the reliability and validity of a panic
Disclosure of Potential Conflicts of Interest and care models for mental health conditions across disorder screen. Ethn Health. 2007;12(3):283-296.
none were reported. primary, specialty, and behavioral health care 20. Krasucki C, Ryan P, Ertan T, Howard R, Lindesay
Funding/Support: This report is based on research settings: systematic review and meta-analysis. Am J J, Mann A. The FEAR: a rapid screening instrument
conducted by the Evidence-based Synthesis Psychiatry. 2012;169(8):790-804. for generalized anxiety in elderly primary care
Program (ESP) Center, located at the Durham VA 8. American Psychiatric Association. Diagnostic attenders. Int J Geriatr Psychiatry. 1999;14(1):60-68.
Medical Center, and funded by the Department of and Statistical Manual of Mental Disorders: DSM-5. 21. Leon AC, Olfson M, Weissman MM, et al. Brief
Veterans Affairs, Veterans Health Administration, 5th ed. Washington, DC: American Psychiatric screens for mental disorders in primary care. J Gen
Office of Research and Development, Health Association; 2013. Intern Med. 1996;11(7):426-430.
Services Research and Development (VA-ESP 9. Zaroukian MH, Kotaru VP. Anxiety. In: 22. Spitzer RL, Kroenke K, Williams JB; Patient
Project 09-010). Henderson MC, Tierney LM, Smetena GW, eds. The Health Questionnaire Primary Care Study Group.
Role of the Sponsors: The funding organization Complete Patient History: An Evidence-Based Validation and utility of a self-report version of
had no role in the design and conduct of the study; Approach to Differential Diagnosis. 2nd ed. Lange PRIME-MD. JAMA. 1999;282(18):1737-1744.
collection, management, analysis, and Medical Books/McGraw Hill; 2012. 23. Spitzer RL, Kroenke K, Williams JB, Löwe B. A
interpretation of the data; preparation, review, or 10. Means-Christensen AJ, Sherbourne CD, brief measure for assessing generalized anxiety
approval of the manuscript; and decision to submit Roy-Byrne PP, Craske MG, Stein MB. Using five disorder: the GAD-7. Arch Intern Med. 2006;166
the manuscript for publication. questions to screen for five common mental (10):1092-1097.
Disclaimer: The findings and conclusions in this disorders in primary care: diagnostic accuracy of 24. Spitzer RL, Williams JB, Kroenke K, et al. Utility
article are those of the authors, who are responsible the Anxiety and Depression Detector. Gen Hosp of a new procedure for diagnosing mental disorders
for its contents; the findings and conclusions do not Psychiatry. 2006;28(2):108-118. in primary care: the PRIME-MD 1000 study. JAMA.
necessarily represent the views of the Department 11. Wilczynski NL, Haynes RB; Hedges Team. 1994;272(22):1749-1756.
of Veterans Affairs or the US government. EMBASE search strategies for identifying
Therefore, no statement in this article should be 25. Moore MT, Anderson NL, Barnes JM, Haigh EA,
methodologically sound diagnostic studies for use Fresco DM. Using the GAD-Q-IV to identify
construed as an official position of the Department by clinicians and researchers. BMC Med. 2005;3:7.
of Veterans Affairs. generalized anxiety disorder in psychiatric
12. Haynes RB, Wilczynski NL. Optimal search treatment seeking and primary care medical
Additional Contributions: We thank Lori Bastian, strategies for retrieving scientifically strong studies samples. J Anxiety Disord. 2014;28(1):25-30.
MD, MHS, Padmanabhan Premkumar, MD, Jason of diagnosis from Medline: analytical survey. BMJ.
Webb, MD, and Joseph Zanga, MD, for their 26. Lindesay J, Briggs K, Murphy E. The Guy’s/Age
2004;328(7447):1040. Concern survey. Prevalence rates of cognitive
valuable comments on previous drafts of the
manuscript. We also thank Liz Wing, MA, Megan 13. Benjamin S, Herr NR, McDuffie J, et al. impairment, depression and anxiety in an urban
von Isenburg, MS, and Avishek Nagi, MS, for Performance characteristics of self-report elderly community. Br J Psychiatry. 1989;155:317-329.
assistance with manuscript preparation and instruments for diagnosing generalized anxiety and 27. Apfeldorf WJ, Shear MK, Leon AC, Portera L. A
literature searching. No one received financial panic disorders in primary care: a systematic brief screen for panic disorder. J Anxiety Disord.
compensation for his/her contributions. review. http://www.hsrd.research.va.gov 1994;8(1):71-78.
/publications/esp/anxiety-panic.cfm#
.Ug0KjNuF-YA. Accessed August 15, 2013. 28. Williams JW Jr, Noël PH, Cordes JA, Ramirez G,
REFERENCES Pignone M. Is this patient clinically depressed? JAMA.
1. Hoffman DL, Dukes EM, Wittchen HU. Human 14. Bossuyt PM, Reitsma JB, Bruns DE, et al; 2002;287(9):1160-1170.
and economic burden of generalized anxiety Standards for Reporting of Diagnostic Accuracy.
Towards complete and accurate reporting of 29. Tatsioni A, Zarin DA, Aronson N, et al.
disorder. Depress Anxiety. 2008;25(1):72-90. Challenges in systematic reviews of diagnostic
studies of diagnostic accuracy: the STARD Initiative.
2. Schonfeld WH, Verboncoeur CJ, Fifer SK, et al. The Ann Intern Med. 2003;138(1):40-44. technologies. Ann Intern Med. 2005;142(12 pt 2):
functioning and well-being of patients with 1048-1055.
84 JAMA July 2, 2014 Volume 312, Number 1 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by Bradford Kney on 07/20/2014You can also read