2021 OPEN ENROLLMENT November 3 - 18, 2020 - Kleinfelder
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 OPEN ENROLLMENT November 3 – 18, 2020

OPEN ENROLLMENT
Act now! Open enrollment is your once-a-year opportunity to make
changes to your benefits without a qualifying life event.
Changes can include:
‹ Enroll in or terminate coverage in a benefit plan
‹ Move from one medical plan to another
‹ Add or drop dependent coverage
‹ New dependents added to benefits will require eligibility documentation
IMPORTANT!
If you do not take action during open enrollment, your 2020 benefit elections will roll
over as your 2021 elections, except the FSA.
You are encouraged to verify all benefits, including your annual HSA election.
You are required to re-enroll in your Flexible Spending Account, as this election will
not roll over.
Don’t’ forget: Open Enrollment is November 3rd – 18th
Elections will be effective January 1, 2021
QUALIFYING LIFE EVENT
Act now! You won’t be able to change your benefits until next year
unless you experience a qualifying life event. Changes to your benefits
due to a life event must be completed within 31 days of the event.
Qualifying life events include:
‹ Change in marital status (marriage or divorce)
‹ Change in the number of dependents (through birth or adoption, or if a child is no
longer an eligible dependent)
‹ Change in your spouse’s employment status, resulting in a loss or gain of coverage
‹ Change in your employment status to/from a benefits-eligible position, resulting in a
loss or gain of coverage
‹ Entitlement to Medicare or Medicaid
‹ Change in your address or location that may affect the coverage for which you are
eligible
‹ Eligibility for coverage through the Marketplace
ELIGIBLE DEPENDENTS
Who can you include on your insurance plan?
Spouse (same and opposite sex)
‹ Married
‹ Domestic partner (where applicable)
‹ Common-law spouse (where applicable)
‹ Civil union partner (where applicable)
Children
‹ Up to age 26, regardless of student status
‹ Natural child
‹ Stepchild
‹ Legally adopted child
‹ Child for whom you have been awarded legal guardianship
‹ Dependent child age 26 or older, who is unmarried, primarily supported by you, and
incapable of self-sustaining employment by reason of mental or physical disability
WHAT IS CHANGING IN 2021?
‹ Medical premiums will increase slightly
‹ Telemedicine through Teladoc
‹ General health copay will increase from $40 to $47 before you meet your deductible
‹ Behavioral Health and Dermatology consultations available beginning January 1, 2021
‹ Health Savings Account maximum contributions will increase
‹ Individual – $3,600 (up from $3,550)
‹ Family – $7,200 (up from $7,100)
‹ Dental carrier will change from Aetna to United Concordia (UCCI)
‹ Dental plan and contributions will remain the same
‹ Vision network will be extended
‹ Walmart/Sam’s Club and Costco will be added to the network January 1, 2021
‹ Life and Disability carrier will change from Lincoln Financial to Unum
‹ Benefits and rates will remain the same
‹ Opportunity for you and your spouse/DP to enroll for Voluntary Life Insurance up to the
Guaranteed Issue amount without submitting an EOI, even if coverage was previously waived
‹ Accident and Critical Illness
‹ Enhanced benefits will be provided at lower rates!
‹ Long Term Care premiums will increase
‹ Additional information will be provided to those impacted at a later date
‹ Live Well Wellness Program
‹ Payroll credits for biometric screenings, benchmarks for activities and premium credits, and
raffles. Three competitions will be held.
2021 MEDICAL PLANS
No Plan Changes! AETNA HDHP 2000 AETNA HDHP 3000
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Aggregate Deductible Embedded Deductible
Aggregate:
Family amount must
Deductible $2,000 $4,000 $3,000 $6,000
Individual be met by one
Family
$4,000 $8,000 $6,000 $12,000 individual or a
Embedded Out-of-Pocket Embedded Out-of-Pocket
combination of all
family members
Out-of-Pocket Maximum $5,000 $10,000 $6,000 $12,000
Individual
Family
$10,000 $20,000 $12,000 $24,000 Embedded:
Family amount must
Coinsurance (You Pay) 20%* 40%* 20%* 40%* be met but no
individual within the
Preventive Care Covered 100% 40%* Covered 100% 40%* family will be subject
to more than the
Primary Care 20%* 40%* 20%* 40%*
individual amount
Specialist Services 20%* 40%* 20%* 40%*
Urgent Care 20%* 40%* 20%* 40%* Note:
See Medical Plan
Emergency Room 20%* 20%* 20%* 20%*
Expense Examples in
Inpatient Hospital 20%* 40%* 20%* 40%* the Appendix
Outpatient Hospital 20%* 40%* 20%* 40%*
*After Deductible
To find out if your provider is in-network, access aetna.com/docfind and search for providers in the
Aetna Choice® POS II (Open Access) network.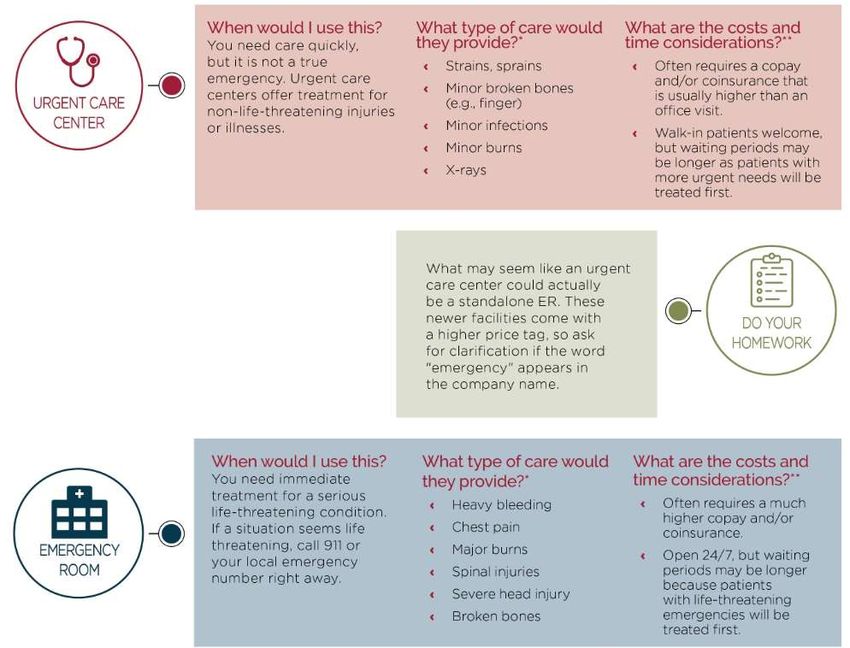
MEDICAL PREMIUMS
Employee monthly cost for medical insurance:
2020 2020
AETNA HDHP AETNA HDHP 3000
2000
MONTHLY CONTRIBUTIONS
Employee Only $103 $51
Employee + Spouse $274 $170
Employee + Children $228 $133
Employee + Family $421 $255
2021 2021
AETNA HDHP AETNA HDHP 3000
2000
MONTHLY CONTRIBUTIONS
Employee Only $110 $54
Employee + Spouse $292 $181
Employee + Children $243 $142
Employee + Family $448 $272
VIRTUAL MEDICINE – TELADOC
‹ You and your family can be treated for ‹ NEW! Mental Healthcare
general health issues at home for a ‹ Talk to a therapist seven days a week
$47 consultation fee until your
deducible is met ‹ Therapist visit: up to $85 until your
deductible is met
‹ Telemedicine is useful for after-hours,
‹ First psychiatrist visit: up to $190 until
non-emergency care, when your
your deductible is met
primary doctor is unavailable
‹ Ongoing psychiatrist visit: up to $95
‹ Teledoc doctors can treat many until your deductible is met
medical conditions, including:
‹ NEW! Dermatology
‹ Cold and Flu
‹ Bronchitis ‹ Upload images of a skin issue online
‹ Urinary Tract Infection (such as eczema, acne, and rashes)
‹ Respiratory infection and get a custom treatment plan
‹ Sinus Problems ‹ Consultation: up to $75 until your
deductible is met
Log on to Teladoc.com/Aetna or call Teladoc directly at
855-Teladoc (855-835-2362) to schedule your consultation.
PHARMACY BENEFITS
Your prescription cost is determined by the tier assigned to the medication.
AETNA HDHP 2000 AETNA HDHP 3000
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
RETAIL RX (30-DAY SUPPLY)
Generic $15 Copay* 50% after Copay* $15 Copay* 50% after Copay*
Preferred $60 Copay* 50% after Copay* $60 Copay* 50% after Copay*
Non-Preferred $90 Copay* 50% after Copay* $90 Copay* 50% after Copay*
Preferred Specialty $95 Copay* Not Covered $95 Copay* Not Covered
Non-Preferred Specialty $115 Copay* Not Covered $115 Copay* Not Covered
MAIL ORDER RX (90-DAY SUPPLY)
Generic $30 Copay* Not Covered $30 Copay* Not Covered
Preferred $120 Copay* Not Covered $120 Copay* Not Covered
Non-Preferred $180 Copay* Not Covered $180 Copay* Not Covered
*After Deductible
Apps such as GoodRx and RxSaver let you compare prices of prescription drugs and find possible
discounts. Note that these discounts cannot be combined with your benefit plan's coverage. If you use
these tools, make sure to check the price against the cost through your plan to get the best deal.
HEALTH SAVINGS ACCOUNT
Are You HSA Eligible?
You are eligible to open and fund an HSA if:
‹ You are enrolled in an HSA-eligible High Deductible Health Plan (HDHP)
‹ You are not covered by your spouse’s non-HDHP
‹ Your spouse does not have a health care Flexible Spending Account or Health
Reimbursement Account
‹ You are not eligible to be claimed as a dependent on someone else’s tax return
‹ You are not enrolled in Medicare or TRICARE
‹ You have not received Department of Veterans Affairs medical benefits in the past
90 days for non-service-related care (service-related care will not be taken into
consideration)
Don’t Forget to Enroll
You will need to complete all HSA enrollment materials and designate the amount to
contribute on a pre-tax basis.HEALTH SAVINGS ACCOUNT
Why have one?
The HSA is owned by you with triple tax benefits:
1. Tax-free contributions
Kleinfelder contributions belong to employees and are not taxable*
Employee contributions are pre-tax and can be set up through payroll
deductions; post-tax contributions are an “above the line” deduction*
2. Tax-free interest on your HSA balance and investment gains*
3. Tax-free withdrawals for qualified healthcare expenses
Advantages
‹ Use your HSA debit card, pay bills online, or use auto-pay to pay healthcare
expenses
‹ Any balance in the account (including Kleinfelder contributions) is yours to keep,
even if you switch medical plans or leave the company
‹ Your HSA balance rolls over from year-to-year (no “use it or lose it“ rule!)
‹ Investment options are available when your account reaches a balance of $2,000
*Account holders should consult a tax advisor. Tax references are at the federal level and special state tax rules may apply.HEALTH SAVINGS ACCOUNT
Contributions
‹ Kleinfelder will contribute $750/Individual or
$1,500/Family for employees enrolled on January 1st
‹ IRS funding limits include Kleinfelder’s contribution
‹ You can contribute a fixed pre-tax amount per pay
period
‹ Employer funding will be deposited bi-weekly
‹ Verify your annual contribution for 2021
Eligible Expenses
‹ Some eligible expenses may not be covered by your health plan, but the IRS allows you to pay for
them with your HSA money:
‹ LASIK eye surgery
‹ Hearing aids
‹ Glasses
‹ Dental expenses
‹ COBRA, Medicare, and Long-Term Care expenses
‹ You can find the full list of allowable expenses in IRS Publication 502 at irs.govHEALTH SAVINGS ACCOUNT
HealthEquity – Make Funds Grow
Maximize your earnings
‹ HSAs earn interest like a traditional savings account
‹ HSA interest earnings are not taxed*
‹ After $2,000 account balance, you can invest in HealthEquity’s or Vanguard’s
investment funds
Easy, Powerful Tools
‹ HealthEquity offers investment guidance to members
‹ HealthEquity Advisor can provide professional advice and access to online tools
‹ How much to keep in your HSA
‹ How much to invest
‹ How to diversify among best-in-class mutual funds to minimize risk and maximize growth
* Account holders should consult a tax advisor. Tax references are at the federal level and special state tax rules may apply.FLEXIBLE SPENDING ACCOUNT
Limited Purpose Flexible Spending Account (LPFSA)
‹ May be elected in addition to an HSA bank account
‹ Funds may be used for dental and vision expenses only
‹ Pre-tax plan year contributions are $2,750
Health Care Flexible Spending Account (HCFSA)
‹ Only for employees who are not enrolled in a Health Savings Account (HSA)
‹ Funds may be used for eligible medical, dental, and/or vision expenses; over-the-counter
drugs must be prescribed by a doctor to be an eligible expense
‹ Pre-tax plan year contributions are $2,750
Dependent Care Flexible Spending Account (DCFSA)
‹ Can only access funds that are in the account at the time of service/claim
‹ Funds may be used for child care (for a child age 12 and under), elder care, or care for
an adult dependent who is not capable of self-care
‹ Pre-tax plan year contributions up to $5,000 per family
Claims must be incurred by December 31, 2021
Unclaimed balances on March 31, 2022 will be forfeitedDENTAL BENEFITS
United Concordia (UCCI) will be your new dental administrator. The dental
network is the Elite Plus Network.
No Contribution Changes!
2021 No Plan Changes!
UCCI DPPO PLAN
Dental Plan IN-NETWORK OUT-OF-NETWORK
MONTHLY CONTRIBUTIONS DEDUCTIBLE
INDIVIDUAL $50 $50
EMPLOYEE ONLY $36.96 FAMILY $150 $150
EMPLOYEE + SPOUSE $73.24 MAXIMUM
PER PERSON $1,500 $1,500
EMPLOYEE + CHILD $80.24
COVERED SERVICES
EMPLOYEE + FAMILY $109.93
PREVENTIVE SERVICES
Oral Exams, Routine Cleanings,
100% 100%
Bitewing X-rays, Fluoride Deductible waived Deductible waived
‹ If you elect dental coverage in 2021, you will BASIC SERVICES
receive a paper ID card from United Concordia. Fillings, Root Canal, Simple 90%* 80%*
Extractions
You may download an electronic ID card
MAJOR SERVICES
beginning January 1, 2021 Crowns, Implants, Dentures, Denture 60%* 50%*
Repair
‹ It is important to present your new dental ORTHODONTICS
information to your provider for any services Child(ren) and Adults
50%
after January 1, 2021. Otherwise, they will ORTHODONTIC LIFETIME
$1,500
MAXIMUM
not be able to verify benefits
*After deductible
Tip: If you choose to use a dentist who doesn’t participate in your plan’s network, your out-of-pocket costs will be higher,
and you will be subject to balance billing.DENTAL WELLNESS & TUITION BENEFITS
Smile for Health® Wellness College Tuition
‹ UCCI offers an enhanced dental ‹ Earn Tuition Rewards points that can
benefit for those who have been be redeemed for tuition discounts at
diagnosed with certain chronic more than 400 participating private
medical conditions: colleges and universities nationwide
‹ Oral Cancer ‹ 1 tuition rewards point = $1 in tuition
‹ Cerebral Vascular Disease discount
‹ Cardiovascular Disease ‹ Earn 2,000 points just by electing
‹ Diabetes coverage with UCCI, then earn
2,000 points each year you’re
‹ Lupus covered by UCCI
‹ Organ Transplant ‹ Transfer your points to your
‹ Rheumatoid Arthritis children, grandchildren, nieces,
‹ Enhanced Benefits include 100% nephews, stepchildren, godchildren
coverage for periodontal (gum and adopted children
disease) maintenance, scaling and ‹ Each child enrolled receives a one-
root planing and periodontal time bonus of 500 tuition reward
surgery, if needed points
‹ To register on or after January 1st, ‹ To sign up on or after January 1st, visit
visit UnitedConcordia.com/GetMDB UnitedConcordia.comDENTAL RESOURCES
My Dental Benefits Find a Dentist
‹ Visit UnitedConcordia.com/GetMDB ‹ Visit UnitedConcordia.com/FindADentist
‹ See coverage and network details ‹ Find in-network dentists near you
‹ Check claim and predetermination status ‹ Search under ELITE Plus Network
‹ See Explanation of Benefits ‹ Search by specialty, and practice or
‹ Print ID cards provider name
‹ Subscribe to helpful emails
‹ Register for special wellness benefits
Mobile Apps
‹ Member App
‹ Find a dentist
‹ Virtual ID card
‹ Access benefits information
‹ Chomper Chums App for Kids
‹ 2-minute brushing timer
‹ Proper brushing habits
‹ Fun animal charactersVISION BENEFITS
No Contribution Changes! 2021 VSP Plan
MONTHLY CONTRIBUTIONS
EMPLOYEE ONLY $5.34
EMPLOYEE + SPOUSE $10.70
EMPLOYEE + CHILD $11.76
EMPLOYEE + FAMILY $18.19
NEW! Walmart/Sam’s Club and Costco
in-network as of January 1, 2021
‹ Retail frame allowance:
‹ Walmart/Sam’s Club: $160
‹ Costco: $90
Suncare Plan
‹ Use your frame allowance toward ready-to-
wear non-prescription sunglasses from a
VSP provider with no prescription requiredSURVIVOR BENEFITS
Unum will replace Lincoln Financial as your Life and Disability carrier
Basic Life and AD&D Insurance
‹ Paid for by Kleinfelder
‹ Employee coverage 2 x base annual earnings
up to a maximum benefit of $400,000
‹ Spouse/Domestic Partner coverage
‹ $2,500
‹ Dependent coverage
‹ $500 per child (birth to 6 months)
‹ $1,000 per child (6 months to age 26)
‹ Don’t forget to complete your beneficiary
designation in UltiPro Benefits
Note: You must enter dependent demographic information in UltiPro Benefits to enroll for Spouse/Domestic
Partner and/or Dependent coverage.SURVIVOR BENEFITS
Voluntary Life Insurance
‹ You have the option to purchase life insurance in addition to the basic life insurance provided
by Kleinfelder
‹ You must purchase coverage for yourself in order to purchase coverage for your spouse/domestic
partner and/or children.
‹ If you enroll for at least $10,000 of Voluntary Life Insurance when initially offered, you may increase your
coverage up to the guaranteed issue of $200,000 during a future Open Enrollment without providing
Evident of Insurability (EOI). Employees who wish to enroll or increase their coverage beyond $200,000
will need to complete an EOI application.
‹ During the 2021 Open Enrollment only, you will be able to purchase up to the Guaranteed Issue amount
for yourself and your spouse/DP without any health questions – even if you waived coverage previously.
‹ Rates and payroll deductions can be found in the Benefits Guide and online during the enrollment
process through UltiPro. Don’t forget to complete the online beneficiary designation form in UltiPro
Benefits.INCOME PROTECTION
Short-Term Disability Overview
Base Short-Term Disability Buy–Up Short-Term Disability
Income
60% of weekly earnings 70% of weekly earnings
Replacement
Weekly Maximum $1,500 $3,500
0 days for disability due to an injury 0 days for disability due to an injury
Waiting Period
7 days for disability due to sickness 7 days for disability due to sickness
Maximum Benefit
13 weeks 13 weeks
Period
Short-Term Disability – Premium paid by Employee post-tax – Benefits are not taxable
Base Short-Term Disability
‹ Mandatory, automatic enrollment for full-time and part-time employees
‹ In California, New Jersey, and New York, the carrier STD benefit will be offset by the benefit
received from the state
Buy-Up Short-Term Disability
‹ Employee can elect Buy-Up option
‹ Rates vary based on salary and age
‹ Conditions treated or diagnosed within 3 months of coverage effective date are excluded for 12
months from coverageINCOME PROTECTION
Long-Term Disability Overview
Base Long-Term Disability Buy–Up Long-Term Disability
Income
60% of monthly earnings 66-2/3% of monthly earnings
Replacement
Monthly Maximum $10,000 $20,000
Waiting Period 90 days 90 days
Maximum Benefit
Up to age 67 Up to age 67
Period
Base Long-Term Disability – Premium Paid by Kleinfelder
‹ Automatic enrollment for full-time and part-time employees
‹ Basic LTD benefits are taxable income
Buy-Up Long-Term Disability– Premium Paid by Employee post-tax
‹ Employee can elect Buy-Up option
‹ Buy-Up LTD benefits are not taxable income
‹ Rates vary based on salary and age
‹ Conditions treated or diagnosed within 3 months of coverage effective date are excluded for 12
months from coverageSUPPLEMENTAL HEALTH
The Company offers ways for you to supplement your medical plan
coverage and help cover unexpected expenses.
Accident Coverage
‹ Provides benefits for you and your covered family members if you have expenses related to an
accidental injury
‹ Can help you pay deductibles, copays, and even typical day-to-day expenses such as a mortgage
or car payment
2020
2021SUPPLEMENTAL HEALTH
Critical Illness Coverage
Enhanced benefits and lower rates
‹ 30-day benefit waiting period waived
‹ 50% recurrence benefit, which provides an additional payout for a subsequent occurrence of benign
brain tumor, coma, heart attack, or stroke, has been added
‹ Pre-existing condition exclusion removed
‹ Guaranteed Issue for employee increased from $20K to $30K
‹ Guaranteed Issue for spouse/domestic partner increased from $10K to $15K
2020 RATES 2021 RATES
Included in the Critical Illness coverage is
an annual wellness benefit which pays
each covered family member $50 for
having a health screening test.
Add the monthly wellness benefit
premium to the Critical Illness monthly
premium.WELLNESS PROGRAM
Live Well Wellness Program is available to all Kleinfelder employees
and spouses/domestic partners
‹ Incentives for 2021:
‹ Biometric + Health Risk Assessment = $150 payroll credit
‹ Raffle entry once you earn 50 points
‹ One entry per quarter for a $100 gift card – 20 winners quarterly
‹ NEW for 2022! Medical Premium Incentive: Employees who are enrolled in
Kleinfelder's Medical Plan and complete the Health Risk Assessment, Biometric Screening,
and earn 150 program points in 2021 will earn a $50 monthly premium incentive in 2022.
That is a discount of $600 a year!
Access Live Well at klflivewell.com
StayWell Help Desk: Telephone 877.571.5156 or Email to klflivewell@staywell.comRETIREMENT PLANNING
‹ The 401(k) plan is designed to encourage you to save through a convenient payroll
deduction process
‹ For 2021, pre-tax and post-tax employee contributions will remain at $19,500
‹ If you are age 50 or older during this calendar year, you may also make a “catch-up
contribution” of $6,500 (no change from 2020), making your maximum contribution
$26,000 for the year
‹ Automatic features of the program include:
‹ Auto enrollment after 30 days of hire at 6% if you do not opt-out
‹ Annual increase of 1% if you do not opt-out
Review your investments for your retirement needs on a regular basis at www.vanguard.com.
Plan No. 091189 / Member Services: 800-523-1123EMPLOYEE ASSISTANCE PROGRAM
Kleinfelder pays for this confidential program for you and your family.
Benefits include:
‹ 24-hour toll-free access – Call 800-932-0034
‹ 6 face-to-face sessions per year (limited to 3 face-to-face sessions per 6 months in
California) with a licensed professional
‹ You can speak confidentially to a consultant who can help you or a family member
with many topics including:
‹ Emotional Health and Well-Being
‹ Alcohol and Drug Dependency
‹ Marriage or Family Relationship Problems
‹ Job Pressures
‹ Stress, Anxiety, Depression
‹ Grief and Loss
‹ Financial or Legal Advice
‹ Legal assistance for unlimited number of
issues per year
‹ Financial consultation for unlimited number
of issues per year
Visit the website Kleinfelder.acieap.comBENEFITS WITH LIMITED ENROLLMENT Benefits that are only available for enrollment at new hire or during open enrollment ‹ Accident ‹ Buy-Up Disability (STD and LTD) ‹ Critical Illness ‹ Flexible Spending Account * ‹ Identity Theft ‹ Pre-paid Legal ‹ Voluntary Life * Certain qualifying life events allow for enrollment in or change of election to a FSA during the year.
MEDICAL/RX PLANS FOR HAWAII EMPLOYEES
Medical Benefits:
HMSA HMO HMSA Comp MED HMSA PPO
IN-NETWORK ONLY IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Annual Deductible $0 $0 $0 $0 $100
Individual
Family
$0 $0 $0 $0 $300
Medical Out-of-Pocket $2,500 $2,500 $2,500 $2,500 $2,500
Individual
Family
$7,500 $7,500 $7,500 $7,500 $7,500
Preventive Care Covered 100% Covered 100% Covered 100% Covered 100% 30% coinsurance
Primary Care $20 copay $14 copay $14 copay $12 copay 30% coinsurance
Specialist Services $20 copay $14 copay $14 copay $12 copay 30% coinsurance
Urgent Care $20 copay $14 copay $14 copay $12 copay 30% coinsurance
Emergency Room $100 copay 20% coinsurance 20% coinsurance 20% coinsurance 20% coinsurance
Inpatient Hospital 10% coinsurance 20% coinsurance 20% coinsurance 10% coinsurance 30% coinsurance
Outpatient Surgery 10% coinsurance 20% coinsurance 20% coinsurance 10% coinsurance 30% coinsuranceMEDICAL/RX PLANS FOR HAWAII EMPLOYEES
Pharmacy Benefits:
HMSA HMO HMSA Comp MED HMSA PPO
IN-NETWORK ONLY IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
Pharmacy Out-of-Pocket $3,600 $3,600 $3,600 $3,600 $3,600
Individual
Family
$4,200 $4,200 $4,200 $4,200 $4,200
Retail (up to 30-day supply)
Generic $7 copay $7 copay $7 copay* $7 copay $7 copay*
Preferred Band $30 copay $30 copay $30 copay* $30 copay $30 copay*
Non-Preferred Brand $30 copay $30 copay $30 copay* $30 copay $30 copay*
Preferred Specialty $100 copay $100 copay Not Covered $100 copay Not* Covered
Plus 20%
Non-Preferred Specialty $200 copay $200 copay Not Covered $200 copay Not Covered
Mail Order (up to a 90-day supply)
Generic $11 copay $11 copay Not Covered $11 copay Not Covered
Preferred Band $65 copay $65 copay Not Covered $65 copay Not Covered
Non-Preferred Brand $65 copay $65 copay Not Covered $65 copay Not Covered
Preferred Specialty Not Covered Not Covered Not Covered Not Covered Not Covered
Non-Preferred Specialty Not Covered Not Covered Not Covered Not Covered Not CoveredDENTAL PLAN FOR HAWAII EMPLOYEES
Dental coverage is included when you elect Medical
HMSA Dental PLAN Calendar Year Rollover
IN-NETWORK OUT-OF-NETWORK
‹ You can accumulate up to $500
annually in unused calendar
maximum that can be carried over
to the next calendar year
CALENDAR YEAR MAXIMUM – You must be a member on the
plan the last day of the calendar
PER PERSON $1,500 $1,500 year
COVERED SERVICES – You must receive one covered
PREVENTIVE SERVICES service during the calendar year
Oral Exams, Routine Cleanings, Bitewing 100% 100% – Your total paid claims during the
X-rays, Fluoride
year must not exceed $700
PREVENTIVE SERVICES – The sum of the rollover amount
70% 70%
Fillings, Root Canal, Simple Extractions from prior years cannot exceed
$1,250
MAJOR SERVICES
Crowns, Implants, Complete or Partial Dentures 50% 50%
ORTHODONTICS Not Covered
Tip: If you choose to use a dentist who doesn’t participate in your plan’s network,
your out-of-pocket costs will be higher, and you will be subject to balance billing.VISION PLAN FOR HAWAII EMPLOYEES
Vision coverage is included when you elect Medical
HMSA Vision Plan ODU HMSA Vision Plan ODV
For those enrolled in the Medical For those enrolled in the Medical
PPO or Comp Med Plan HMO Plan
IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK
EYE EXAMINATION $10 copay Up to $40 N/A N/A
SINGLE VISION LENSES $10 copay Up to $16 $10 copay Up to $16
MULTIFOCAL VISION
LENSES $10 copay Up to $25 $10 copay Up to $25
CONTACT LENSES $130 allowance $130 allowance
Up to $50 Up to $50
(IN LEUI OF GLASSES) after $25 copay after $25 copay
CONTACT LENS FITTING $45 allowance Up to $20 $45 allowance Up to $20
FRAMES $15 copay Up to $12 $15 copay Up to $12MEDICAL/RX PLANS FOR HAWAII EMPLOYEES
Your monthly cost for Medical/Rx, Dental and Vision coverage:
HMSA HMO HMSA Comp MED HMSA PPO
1.5% of gross 1.5% of gross 1.5% of gross
SINGLE
earnings earnings earnings
2 PARTY $243.08 $244.77 $250.36
3 PARTY $486.16 $489.54 $500.72HOW TO ENROLL
Open Enrollment Process Through UltiPro Benefits
Available November 3rd – November 18th
To Begin Enrollment
‹ Logon to UltiPro.com
‹ Go to Myself and then click on
Manage My Benefits
‹ Verify your profile under Personal
‹ Verify your dependents under
Review My Family
‹ Review the dependents that
are listed to ensure the
information is accurate. If you
need to add a new dependent,
click the Add Family MemberHOW TO ENROLL
Shop for Benefits Review and Checkout
‹ There is a separate page for each type of ‹ Once you have made your elections, you
benefit will be taken to Review and Checkout
‹ Review your family members listed in which will summarize your elections
Family Covered. To remove someone ‹ You can view additional detail, including
from that list, select Edit Family covered family members, by clicking the
Covered and uncheck the box next to grey plus (+) button beneath the plan
the name, and click Confirm ‹ You may edit coverage by either using the
‹ Once you are ready to choose your shopping cart at the top of the page or by
plan(s), select View Plan and then selecting Modify Coverage next to the
Update Cart plan
‹ If you wish to decline coverage select the ‹ Select the green Checkout button at the
Decline Benefits button bottom of the page to finalize your benefitsREMINDERS
‹ If you added new dependents, dependent eligibility documentation must be
uploaded to the UltiPro Benefits enrollment site by December 1st
‹ Review your annual HSA election amount to ensure it is correct
‹ FSA participants MUST enroll and elect a new FSA contribution each year
‹ Confirm or add your beneficiary information
‹ Always check your payroll deductions and notify us of any issues. Elections
made during Open Enrollment will be effective on your payroll on January 8,
2021.OPEN ENROLLMENT
Open Enrollment is November 3 – 18, 2020
‹ Attend an Open Enrollment webinar
‹ Your benefits enrollment must be completed/approved by 11:59 p.m. CT, Wednesday,
November 18th
‹ Enroll online through UltiPro Benefits
‹ Additional benefit information is available in the UltiPro Benefit Document Library
‹ We are here to assist you!
Kleinfelder Benefits Assistance Center
844.398.0461
kleinfelderbenefits@lockton.com
Charlotte Harrell Marie Mitchell-Jackson Jacky Vargas
charrell@kleinfelder.com mmitchelljackson@kleinfelder.com javargas@kleinfelder.comQUESTIONS
Thank you for attending!APPENDIX
MEDICAL PLAN EXPENSE EXAMPLES
Example 1: Bob is enrolled in family coverage. He has surgery and his bill is
$10,000 using In-Network providers
AETNA HDHP 2000 AETNA HDHP 3000
Aggregate: Embedded:
Deductible Type An individual is subject to An individual is subject
the family deductible to the individual deductible
Embedded: Embedded:
Out of Pocket Maximum Type An individual is subject to the An individual is subject to the
individual out of pocket max individual out of pocket max
In-Network Deductible for Bob $4,000 $3,000
In-Network Out of Pocket Maximum for Bob $5,000 $6,000
Bob’s Expenses $10,000 $10,000
Deductible Applied - $4,000 - $3,000
Remaining Allowed $6,000 $7,000
Bob’s Coinsurance $1,000 $1,400
Annual Payroll Deduction $5,052 $3,060
Kleinfelder HSA Contribution - $1,500 - $1,500
Bob’s Total Cost for the Year $8,552 $5,960
*This example assumes no other family member had claims for the yearMEDICAL PLAN EXPENSE EXAMPLES
Example 2: Bob is enrolled in family coverage. Everyone in Bob’s family incurs
expenses for routine wellness exams only which are paid at 100% using In-
Network providers
AETNA HDHP 2000 AETNA HDHP 3000
Aggregate: Embedded:
Deductible Type An individual is subject to An individual is subject
the family deductible to the individual deductible
Embedded: Embedded:
Out of Pocket Maximum Type An individual is subject to the An individual is subject to the
individual out of pocket max individual out of pocket max
Family In-Network Deductible $4,000 $6,000
Family In-Network Out of Pocket Maximum $10,000 $12,000
Bob’s Family Expenses $0 $0
Annual Payroll Deduction $5,052 $3,060
Kleinfelder HSA Contribution - $1,500 - $1,500
Bob’s Total Cost for the Year $3,552 $1,560MEDICAL PLAN EXPENSE EXAMPLES
Example 3: Bob is enrolled in family coverage. Everyone in Bob’s family incurs
expenses, but no one person reaches $3,000
AETNA HDHP 2000 AETNA HDHP 3000
Aggregate: Embedded:
Deductible Type An individual is subject to An individual is subject
the family deductible to the individual deductible
Embedded: Embedded:
Out of Pocket Maximum Type An individual is subject to the An individual is subject to the
individual out of pocket max individual out of pocket max
Family In-Network Deductible $4,000 $6,000
Family In-Network Out of Pocket Maximum $10,000 $12,000
Bob’s Expenses $2,500 $2,500
Jane’s Expenses $2,000 $2,000
Julie’s Expenses $1,500 $1,500
Deductible Applied - $4,000 - $6,000
Remaining Allowed $2,000 $0
Bob’s Coinsurance $400 $0
Annual Payroll Deduction $5,052 $3,060
Kleinfelder HSA Contribution - $1,500 - $1,500
Bob’s Total Cost for the Year $7,952 $7,560
*MEDICAL PLAN EXPENSE EXAMPLES
Example 4: Bob is enrolled in family coverage. Everyone in Bob’s family incurs
high expenses, resulting in the family meeting their out of pocket maximum.
AETNA HDHP 2000 AETNA HDHP 3000
Aggregate: Embedded:
Deductible Type An individual is subject to An individual is subject
the family deductible to the individual deductible
Embedded: Embedded:
Out of Pocket Maximum Type An individual is subject to the An individual is subject to the
individual out of pocket max individual out of pocket max
Family In-Network Deductible $4,000 $6,000
Family In-Network Out of Pocket Maximum $10,000 $12,000
Bob’s Family Expenses $10,000 $12,000
Annual Payroll Deduction $5,052 $3,060
Kleinfelder HSA Contribution - $1,500 - $1,500
Bob’s Total Cost for the Year $13,552 $13,560
*MEDICAL PLAN EXPENSE EXAMPLES
Example 5: Susan is enrolled in employee only coverage. She has surgery and
her bill is $12,000 using In-Network providers
AETNA HDHP 2000 AETNA HDHP 3000
Aggregate: Embedded:
Deductible Type An individual is subject to An individual is subject
the family deductible to the individual deductible
Embedded: Embedded:
Out of Pocket Maximum Type An individual is subject to the An individual is subject to the
individual out of pocket max individual out of pocket max
In-Network Deductible $2,000 $3,000
In-Network Out of Pocket Maximum $5,000 $6,000
Susan’s Expenses $12,000 $12,000
Deductible Applied - $2,000 - $3,000
Remaining Allowed $10,000 $9,000
Susan’s Coinsurance $2,000 $1,800
Annual Payroll Deduction $1,236 $612
Kleinfelder HSA Contribution - $750 - $750
Susan’s Total Cost for the Year $4,486 $4,662WHERE TO GO FOR CARE
WHERE TO GO FOR CARE
FLEXIBLE SPENDING ACCOUNT
Dependent Care Health Care Limited Purpose
FSA FSA FSA1
Maximum Deferral $5,000 $2,750 $2,750
Childcare
Medical
Eldercare Dental
Eligible Expenses Dental
Daycare for disabled Vision
Vision
dependent
Debit Card Included? No Yes Yes
1If you enroll in a HDHP medical plan, the online system will automatically provide you with the option to enroll in the
Limited Purpose FSA
Limited Purpose FSA
‹ Eligible dental and vision expenses only (medical expenses must be reimbursed
through HSA per IRS regulations)
‹ Debit card may only be used at providers that exclusively provide dental and vision
services (i.e., dentists, optometrists, ophthalmologists, dental surgeons, and vision/eye
care centers)SURVIVOR BENEFITS
Example – Employee age 35 elects $120,000 of coverage, non-smoker
TO CALCULATE HOW MUCH YOUR VOLUNTARY LIFE COVERAGE WILL COST
$ 120,000 ÷ 10,000 = $ 12.00 X $0.70 = $ 8.40
Benefit Elected Monthly PremiumCOMMUTER BENEFITS Aetna / PayFlex Commuter Benefits Public Transportation ‹ Transit passes, fare cards, smart cards Parking Products ‹ Monthly Direct Pay to parking provider; daily, weekly, or monthly Commuter Check for Parking; Pre-paid MasterCard Bicycle Benefit ‹ $20 voucher/month for bicycle storage between commutes for on-going maintenance. The vouchers may also be saved up for the purchase towards a new bicycle. (Taxable Benefit) ‹ Cannot use with commuter benefit – IRS does not allow the bike benefit to be combined with any other Commuter Benefit products or company subsidy. Note: The $20 per month bicycle commuter reimbursement benefit has been eliminated by the Tax Cuts and Jobs Act through the year 2025. Kleinfelder will continue to offer this benefit to its employees; however, it must be reported as taxable income to the IRS.
COMMUTER BENEFITS
Aetna / PayFlex Commuter Benefits Ordering Process
‹ Employees can order or change their commuter benefits online at www.PayFlex.com
‹ Employees can place their orders up until the 8th of the month at 11:59 p.m. Eastern
Time for the following benefit month
‹ Monthly orders are confirmed via email next business day
‹ Recurring orders are confirmed via email each month 2 days before order cutoff
date
‹ Kleinfelder will subsidize up to $100 per month for paid parking at select locations
‹ Employees can make changes at any time based on commuter status
Member Services: 888.678.8242 Website: PayFlex.comVOLUNTARY BENEFITS
Home / Auto Insurance
‹ Employees have access to discounted home and auto insurance through MetLife
‹ Auto insurance includes your vehicle, boat, motor home, or recreational vehicle
‹ Your coverage stays with you even if you leave Kleinfelder
Long-Term Care
‹ Provides a benefit when you need assistance, either at home or in a facility, with
activities of daily living due to an accident, an illness, or advancing age
‹ A monthly benefit is paid directly to the insured individual, to be used at their
discretion, to help pay for needed care
‹ This plan is offered through UNUMVOLUNTARY BENEFITS
Pre-Paid Legal Coverage
Legal Plan Benefits
Family Law
Guardianship or Conservatorship (Contested)
Real Estate Matters
Home Equity Loans (Second or Vacation Home)
Refinancing of Home (Second or Vacation Home)
Sale or Purchase of Home (Second or Vacation Home)
The complete and detailed list of Met Life Legal enhanced benefits is available in UltiPro Benefits
under the Benefit Document Library.
LEGAL PLAN
Monthly Premium $17.50VOLUNTARY BENEFITS
Identity Theft Protection – What’s Covered
Identity Restoration – Licensed private Privacy Monitoring – Monitors websites,
investigators perform the bulk of the networks, and social media for member’s
restoration work required to restore your personal identifiable information, looking for
identity to pre-theft status matches of name, date of birth, social
security number, driver’s license number,
passport number, and/or medical ID number
Identity Consultation Services
‹ Privacy and Security Best Practice
Security Monitoring – Provides internet
‹ Event-Driven consultation support court record and credit monitoring, along with
‹ Lost/stolen wallet assistance credit inquiry alerts, payday loan monitoring,
and quarterly credit score tracking
‹ Alert and Notifications
‹ Monthly identity theft updates to help
educate and protect
IDENTITY THEFT
Employee Only Employee + Family
Monthly Premium $8.95 $18.95MILK STORK
Milk Stork
‹ Breast milk delivery service for
business-traveling moms
‹ Refrigerated, express shipping or
easy toting of breast milk home to
baby
How It Works
The Pump and Ship
‹ For a mom who needs a no-fuss
solution to overnight her refrigerated
breast milk home
The Pump and Tote
‹ For a mom who would prefer to carry
her refrigerated breast milk home
milkstork.com/KleinfelderFAMILY CARE BENEFITS
Back Up Care For Children
Subsidized and vetted childcare when you need it most. Backup Care isn’t just for
emergencies. Use your benefit to cover school holidays or any other time you need a
quality caregiver.
Ways To Use Your Benefits
‹ Sick kids
‹ Teacher workdays
‹ Sick nanny
‹ Early flights or business travel
‹ Late nights working
‹ School holidays
‹ Working from home
‹ Daycare closures
‹ In-Center Benefits
‹ Vetted network of childcare centers
‹ Coverage across the US throughout the week
‹ In-Home Benefits
‹ Back up care is available for any of your children from newborns to teens, 24/7 for work-related
issues
‹ Care may be requested up to 90 days in advanceFAMILY CARE BENEFITS
Help for every adult family member
Back Up Care For Adults
‹ You can provide quality care for your spouses, parents, in-laws, grandparents, and
adult children
‹ Subsidized and vetted in-home care for any adult in your family – including yourself.
Caregivers may be certified nurse’s aides, home health aides, or experienced elder
care companions
Ways To Use Your Family Care
Benefits
‹ Mom or dad needs a ride to doctor
appointments
‹ You (or your spouse) are recovering
from surgery
‹ Companion care for your adult child
‹ Cover a gap in your regular adult
senior careADDITIONAL BENEFITS
Aetna World Traveler
‹ Employees are provided with emergency and urgent medical benefits and
assistance during a shot-term business trip
‹ Aetna’s tools and resources will help you prepare for your trip and obtain important
information during your travels
‹ Aetna’s secure member website allows you to search for international doctors and
hospitals, review country specific health and security information, and obtain
translations for medical terms in multiple languages
Assist America
‹ Travel assistance through Assist America can help bring comfort and reassurance if
you face a medical emergency while traveling 100 or more miles from home
‹ Assist America can help with:
‹ Hospital admission, prescription replacement, referral to medical providers
‹ Critical care monitoring
‹ Emergency medical evacuation
‹ Care and transport of unattended minor children
‹ Lost or stolen travel documents
‹ Legal and interpreter referrals
‹ Emergency message serviceYou can also read