Education for the Revised Transfusion Reaction Algorithm 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Education for the Revised
Transfusion Reaction Algorithm
2018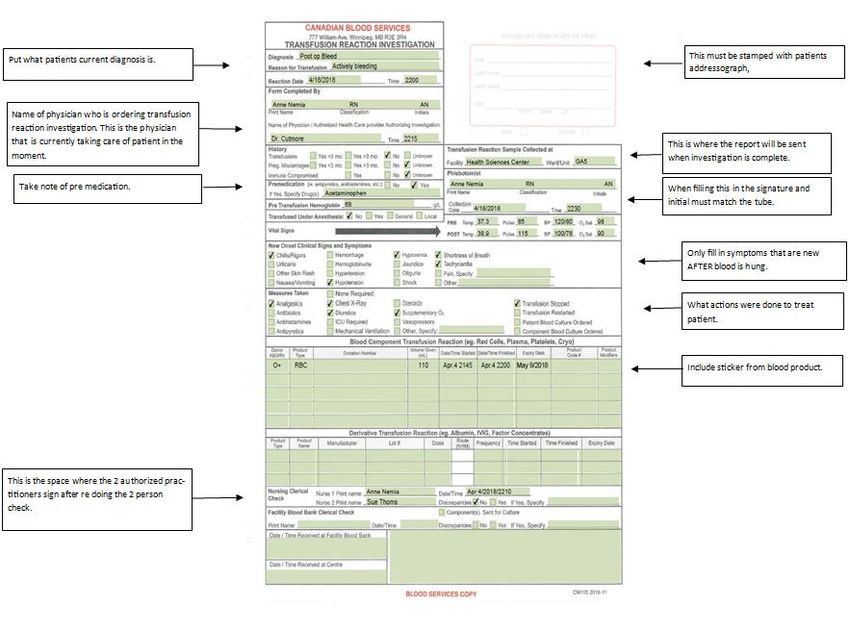
Definition of Transfusion
Reaction
*Any untoward event that occurs as a result of infusion of blood components or
derivatives(plasma protein products)
*Immediate or delayed
*Considered definitely, probably or possibly related to the infusion
*When any unexpected or untoward sign or symptom occurs during or shortly after
the transfusion of a blood component, a transfusion reaction must be considered
as the precipitating event until proven otherwise.
Webert, K. McMaster University. 2015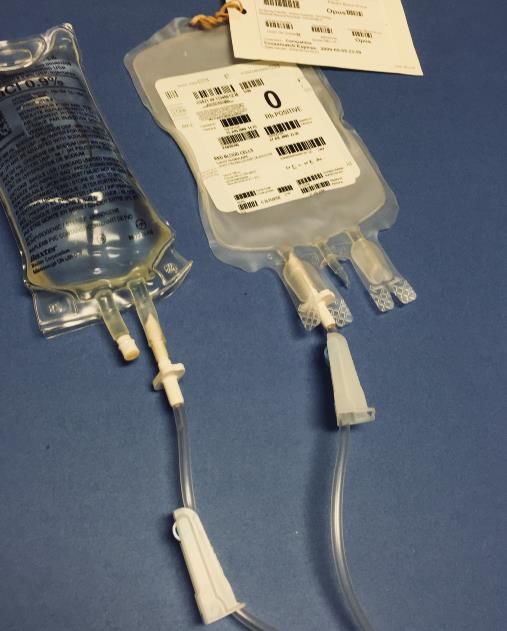
The 5 W’s
Who’s involved
• The Medical Directors at Shared Health
Diagnostic Services Manitoba and Canadian
Blood Services have approved the revised
Transfusion Reaction Algorithm
• PNRGTP have
(Provincial Nursing Resource Group for Transfusion Practice)
participated in content review, supported by
TPC’s( Transfusion Practice Committees)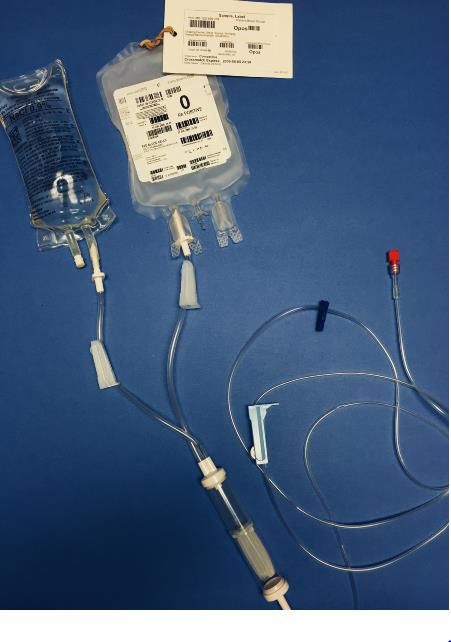
What does the new document look
like?
Side 2

Where does this take effect?
When does this take effect?
Why the revision? • Alignment of algorithm and procedures • Reinforcement that the clinical signs and symptoms observed are NEW onset related to the transfusion • When assessed several common suggestions were made • Easier to follow
Distribution • Designated Site Leads have been sent an education package which include; A letter from DSM indicating that all old algorithms be removed and discarded Laminated transfusion reaction algorithms
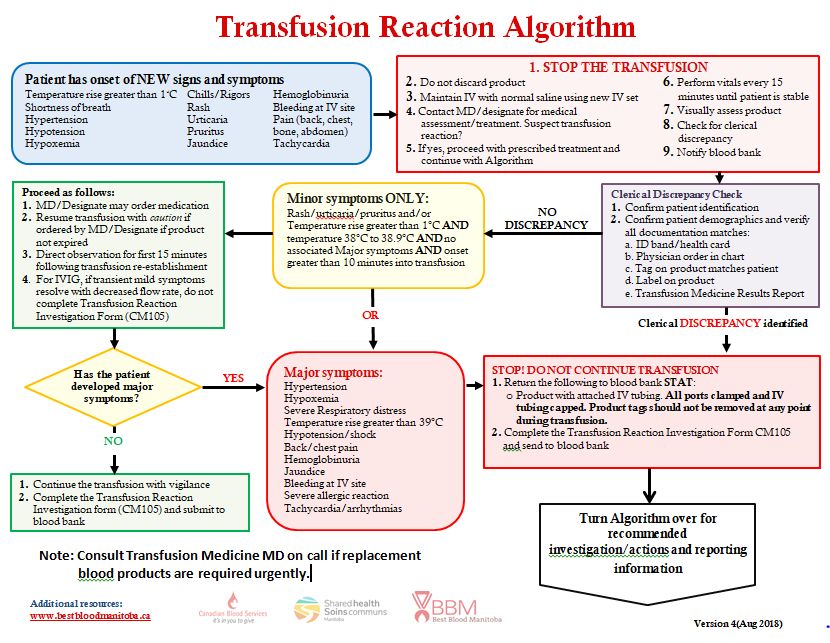
Symptoms No Change
Number 4 and 5 have changed. Now says “Contact MD/Designate for medical assessment/ treatment”. If the physician suspects that this is a transfusion reaction then you are to proceed with the algorithm, if they assess this is not a transfusion reaction then proceed with transfusion. If you are unable to get a hold of the prescribing physician then
Clerical Discrepancy Check Number 2 now reads.. Confirm patient demographics and verify all documentation matches. C. Tag on product matches patient
• The Manilla tag must not be removed from the Blood/ Blood Product until the transfusion is complete and a transfusion reaction is not suspected. • This is a part of Accreditation Canada requirements (CSA Z902-10, 11.3.4.)
• More definition as to how a minor reaction is defined. • Temperature tighter parameters
• Administer any treatment the physician may order • The transfusion will be resumed cautiously and under observation for the first 15 minutes after re- establishment • Complete CM105 • No change to the IVIG
Major Reactions
• Symptoms have been rearranged
• Have removed the “Consult
Transfusion Medicine MD on call… “
so that this is now at the bottom of
the algorithm• Major Transfusion reactions will require specific testing dependent on the symptoms. • Have added a chart on the back that puts the symptoms into more specific groups with the recommended investigations/ actions
Returning the Blood to the Blood
Bank
Tubing must be attached….The C’s
• Blue clipmust be secure
(coming from IV pump)
• Roll clamp must be tight
• A cap must be placed on the
end of the IV line
• complete the CM105
(transfusion reaction
investigation form)Please Do Not Use These
These should not be
used to clamp the
bags!
Rationale:
If they open en-route
back to the blood bank
the blood can no
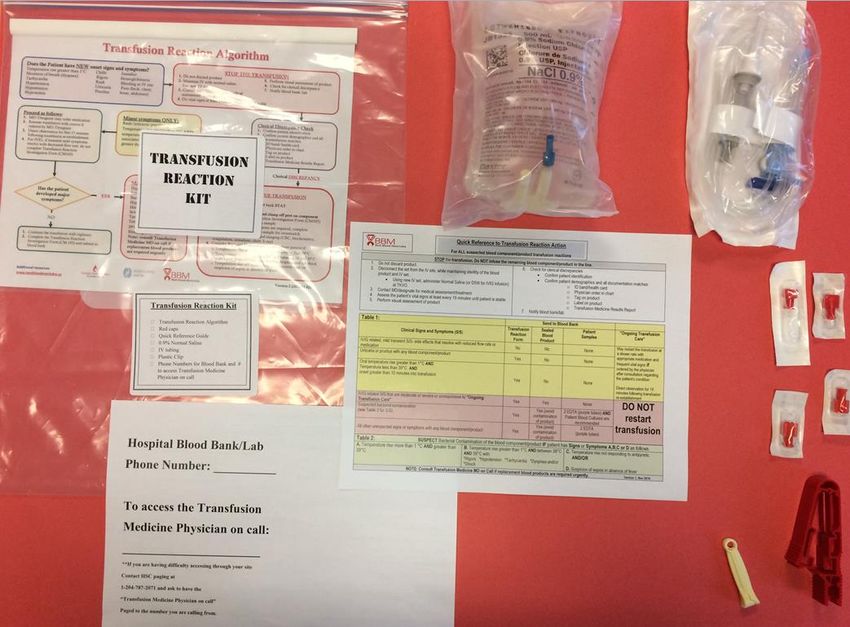
longer be culturedAction Packed! • Each site is encouraged to update their transfusion reaction kit • This could contain: – Algorithm on the front – Sterile Red Cap – Transfusion Reaction Investigation Form – Remove the Clip – This package should be kept somewhere easily accessible - 500 ml bag of Normal saline with a new IV set - Quick Reference Sheet
What could Kits look like?
What happens if I need blood and
the patient has had a reaction?
If URGENT blood is
needed then call the
Transfusion Medicine
Physician on call
If the patient will require further blood
products, send another crossmatch
sample and requisition
** Shared Health provides 24/7 Transfusion Medicine on call support, call your paging
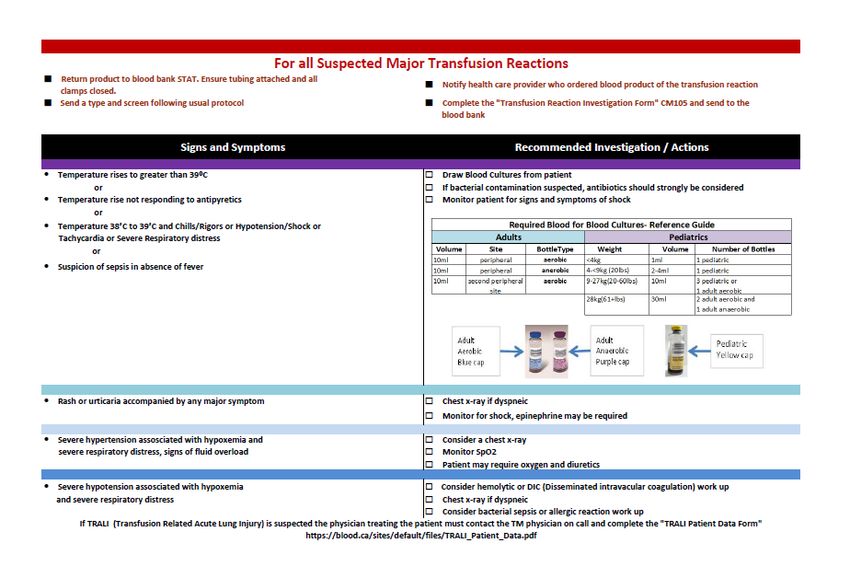
department, blood bank… or HSC Paging to contactThe Back The above actions will be required for all Major transfusion reactions.
Suspected Bacterial Contamination
• Cultures are to be drawn from patient using the above criteria
• Patient should be closely monitored for signs and symptoms of shock when bacterial
contamination is suspected
• Physician who is ordering cultures on patient must also write order for blood bag
contents to be cultured prior to sending the product back to the blood bank
• Once blood is returned to the blood bank it is then sent to microbiology for culturingPossible anaphylactic reaction • Transfusion-associated anaphylactic shock is rare • Anaphylaxis accounts for approximately 5% of transfusion associated deaths (Blood Easy 4, 2016)
• These signs and symptoms are common when TACO ( Transfusion associated
circulatory overload) is suspected.
• Results from impaired cardiac function, and or excessively rapid rate of
transfusion
• Incidence is 1:700 to 8% of transfusion recipients
• TACO is the most common cause of death from transfusion!
• Patients who are most susceptible:
• Over 70 years of age, infants, patients with severe euvolemic anemia
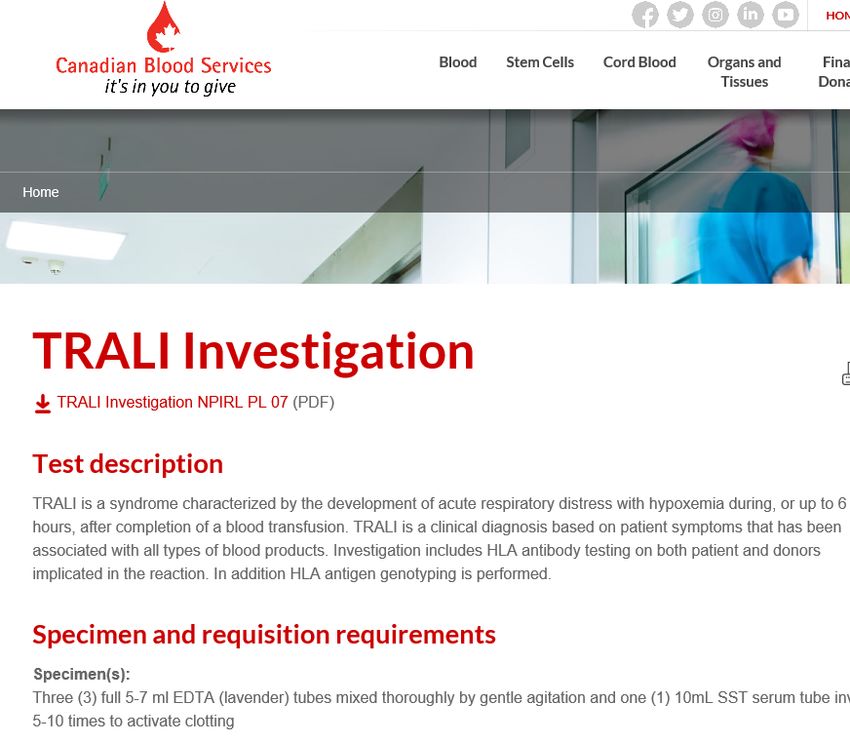
(hemoglobin• Could be TRALI (transfusion related lung
injury)
• Bacterial Contamination
• Acute hemolytic transfusion
reaction- can be associated with
ABO- incompatibility
• AnaphylaxisTransfusion Transmitted
Transfusion Injury
Transmission Surveillance
Information
System (TTISS)
Surveillance SystemQuick Reference Guide *Optional Resource
*Optional Resource
Contacts
Blood Management Service office
1-204-926-8006
Darcy Heron
Shared Health
1-204-237-2707
Email to
bmsclinical@wrha.mb.caAcknowledgements Transfusion Reaction Algorithm • Dr. Charles Musuka • Dr. Debra Lane • Dr. Arjuna Ponnampalam • Darcy Heron • Lee Grabner • Shana Chiborak • Provincial Nurses Resource Working Group
Questions?
References
• Dr. Kerry Gunn – Aukland District Health Board Blood transfusion Committee Chair- April 2013
• Kirkey, S. (2013). Health experts confront the hidden hazards of blood transfusions. Retrieved from
http://o.canada.com/news/blood-hazards
• Daw, Z., Padmore, R., Neurath, D., Cober, N., Tokessy, M., Desjardins, D., Olberg, B., Tinmouth, A., & Giulivi A. (2008).
Hemolytic transfusion reactions after administration of intravenous immune (gamma) globulin: a case series analysis.
Transfusion, 48(8), 1598-1601. doi: 10.1111/j.1537-2995.2008.01721.xFor the complete PDF education
package please go to
www.bestbloodmanitoba.caThank you!
You can also read