Emergence of multidrug-resistant Salmonella enterica serotype Typhi with decreased ciprofloxacin susceptibility in Bangladesh
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Epidemiol. Infect. (2006), 134, 433–438. f 2005 Cambridge University Press
doi:10.1017/S0950268805004759 Printed in the United Kingdom
Emergence of multidrug-resistant Salmonella enterica
serotype Typhi with decreased ciprofloxacin susceptibility
in Bangladesh
M. R A HM A N *, A. K. S ID DI Q U E, S. S HO M A, H. R A S HI D, M. A. S A L A M,
Q. S. A HM E D, G. B. N A I R A N D R. F. B R E IM A N
ICDDR,B :Centre for Health and Population Research, Dhaka, Bangladesh
(Accepted 22 April 2005, first published online 29 July 2005)
SUMMARY
During 1989–2002, we studied the antimicrobial resistance of 3928 blood culture isolates of
Salmonella enterica serotype Typhi (S. Typhi) in Dhaka, Bangladesh. Overall 32 % (1270)
of the strains were multidrug-resistant (MDR, resistant to chloramphenicol, ampicillin and
trimethoprim–sulphamethoxazole) ; first detected in 1990 (rate of 8 %), increased in 1994 (44 %),
declined in 1996 (22 %, P434 M. Rahman and others
decreased susceptibility to ciprofloxacin, and resistant clinical microbiology laboratory cultures blood from
to nalidixic acid (MICo32 mg/ml) was detected in in-patients with diarrhoea and fever as determined
1991 resulting in treatment failure in a patient who by the centre’s physicians as well as from outpatients
had recently returned to the United Kingdom from who are referred to the this laboratory by physicians
India. Such strains were subsequently isolated in in Dhaka city.
many countries resulting in suboptimal clinical re-
sponses and therapeutic failures [13–16]. An epidemic Bacterial strains
caused by similar type of strain of S. Typhi (R type :
We studied all isolates of S. Typhi from blood
ApCmSXTCp) has been reported in Tajikistan [17].
cultures of sporadically occurring enteric fever cases
Nalidixic acid-resistant S. Typhi with decreased sus-
reporting to the ICDDR,B hospital in Dhaka be-
ceptibility to ciprofloxacin is now endemic in Vietnam
tween 1989 and 2002. Blood was cultured by standard
[18], India [13, 19] and neighbouring countries com-
methods, as previously described [8]. All micro-
plicating the treatment of typhoid fever. Recently,
biological and epidemiological information was collec-
ciprofloxacin treatment failure in a patient with
ted.
typhoid fever caused by a MDR strain of S. Typhi
having decreased susceptibility to ciprofloxacin
Antimicrobial susceptibility testing
(MICo0.25 mg/ml), has been reported for the first
time in the southern part of Bangladesh [16]. Thus, In vitro susceptibilities to chloramphenicol, trimetho-
the detection of decreased susceptibility to cipro- prim-sulphamethoxazole, ampicillin, ciprofloxacin
floxacin in the laboratory is essential for treating and ceftriaxone were performed by the disk diffusion
typhoid fever. The commonly used disk diffusion method [8, 20] during 1989–2002 using commercial
technique is not useful for detecting decreased sus- antimicrobial disks (BBL, Baltimore, MD, USA) with
ceptibility to ciprofloxacin, and determination of the Escherichia coli ATCC 25992 as the control strain
MIC of ciprofloxacin is the gold standard for detect- following the guidelines of the National Committee
ing decreased susceptibility to ciprofloxacin [13, 14]. for Clinical Laboratory Standards (NCCLS), USA.
When compared with the disk diffusion technique, MIC of antimicrobial agents was determined for
determination of MIC in the laboratory is expensive selected isolates. Since decreased ciprofloxacin sus-
and needs trained personnel to perform the test. ceptibility was first reported in 1990 [15], 132 S. Typhi
Moreover, the facility for determination of MICs strains isolated in years 1990 (25 isolates), 1995
is not available in many laboratories of developing (25 isolates), 2000 (25 isolates), 2001 (25 isolates)
countries where MDR typhoid fever is endemic. and 2002 (32 isolates) were randomly selected for
Thus, a disk diffusion technique for detecting de- determining MIC without pre-existing knowledge
creased susceptibility to ciprofloxacin would be easy, of their antimicrobial susceptibility patterns. The
less expensive and a user-friendly means for helping isolates were subcultured from glycerol stock
physicians to administer the proper treatment for (x80 xC) in 2002 and tested for susceptibility to the
typhoid fever. We, therefore, studied the present above-mentioned antimicrobial agents and nalidixic
trends in antimicrobial resistance of S. Typhi in acid by disk diffusion method, and by E tests
Dhaka, the capital of Bangladesh, to define optimal (AB-Biodisk, Solna, Sweden) or agar dilution tech-
therapeutic strategies in this impoverished setting nique (only for nalidixic acid) to obtain the MIC
with particular reference to the emergence and de- values of these antimicrobial agents.
tection of decreased ciprofloxacin susceptibility in The inhibition zone diameters obtained by disk
prevalent MDR S. Typhi isolates. diffusion method, and MIC values were compared
by scattergram to determine zone diameter for de-
tecting decreased susceptibility to ciprofloxacin by
MATERIALS AND METHODS disk diffusion method.
Resistance simultaneously to three or more differ-
Clinical samples
ent groups of antimicrobial drugs was defined as
The study was conducted in Dhaka Clinical Research MDR ; decreased ciprofloxacin susceptibility was
and Service Centre (CRSC), of ICDDR,B :Centre defined as an isolate with ciprofloxacin MIC within
for Health and Population Research, Bangladesh. the range of 0.25–1 mg/ml and ciprofloxacin resistant
It serves 100 000 diarrhoeal patients annually. The if the MIC was o4 mg/ml.
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 06 Feb 2021 at 13:28:16, subject to the Cambridge Core terms of use, available at https://www.cambridge.org/core/terms
. https://doi.org/10.1017/S0950268805004759Decreased susceptibility to ciprofloxacin in MDR S. Typhi 435
50 44 30
45 42
41 40
40 36 25
35 31 30 31
29
Percentage
30 24 20
22 23
25
Number
20 15
15
10 8
10
5 0
0
5
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
(61) (99) (231) (309) (479) (547) (582) (375) (226) (306) (174) (153) (212) (173)
0
Years (number tested) 1990 (25) 1995 (25) 2000 (25) 2001 (25) 2002 (32)
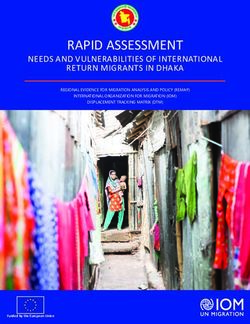
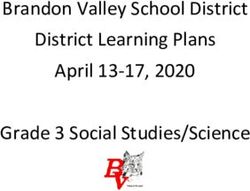
Fig. 1. Percentage of Salmonella Typhi isolates from blood Year
cultures simultaneously resistant to ampicillin, chloram- Fig. 2. Number of Salmonella Typhi strains resistant to
phenicol and trimethoprim–sulphamethoxazole (MDR ampicillin, chloramphenicol and trimethoprim–sulpha-
S. Typhi), 1989–2002. methoxazole (MDR) and strains with decreased cipro-
floxacin susceptibility. %, Susceptible S. Typhi ; , MDR
RESULTS S. Typhi ; , MDR with decreased ciprofloxacin suscepti-
bility ; &, decreased ciprofloxacin susceptibility (non-
The proportion of MDR S. Typhi isolates increased MDR).
to a peak of 44 % in 1994 from 8% in 1990, then
decreased and ranged from 22 to 31 % during 1995–
2000, increased again to 36 % in 2001, and to 42 % a ciprofloxacin inhibition zone of f24 mm resulted
in 2002 (Fig. 1), suggesting the emergence, decline in 98% sensitivity and 100% specificity. None was
and re-emergence of MDR S. Typhi in Bangladesh. completely resistant to ciprofloxacin or ceftriaxone
Other resistance patterns such as resistance to one by NCCLS criteria. Two out of 25 (8 %) isolates
and two drugs were low (5–7 %). All isolates were (Fig. 2) exhibited decreased ciprofloxacin suscep-
susceptible to ciprofloxacin (inhibition zone diameter tibility in 2000, seven (28 %) in 2001 and 15 out of
of o21 mm) and ceftriaxone by the disk diffusion 32 (47 %) in 2002 (P436 M. Rahman and others
Table. Ciprofloxacin and nalidixic acid disk diffusion results as indicators for ciprofloxacin MICs in
Salmonella Typhi (n=132) for detecting decreased ciprofloxacin susceptibility
Disk diffusion results of
(NCCLS)# Proposed zone diameter Range of MIC (MIC90)* mg/ml of
for detecting decreased
No. of Nalidixic Cipro- ciprofloxacin Nalidixic
strains acid floxacin susceptibility acid Ciprofloxacin
107 S S S (o25 mm) 2–8 (8) 0.008–0.064 (0.016)
1 I S S (o25 mm) 16 0.125 (0.125)
24 R S R (f24 mm) 128 to >256 0.25 (0.25)
(>256)
* MIC90 was calculated separately for 108 nalidixic acid-susceptible and 23 nalidixic acid-resistant strains.
# S, Susceptible ; I, intermediate ; R, resistance.
phenotype in more than 50% of 49 S. Typhi isolates alternatives although the optimum treatment of these
suggesting the dissemination of the MDR strains in infections is still unclear [25].
the community [22]. Recently, a similar prevalence With the increasing prevalence of MDR strains
of MDR S. Typhi has been reported in Kolkata, that have decreased ciprofloxacin susceptibility and
India [23] confirming its re-emergence in the Indian resistance to nalidixic acid, there is a need for care-
subcontinent. A high (52–82 %) prevalence of MDR ful observation of outcome of therapy for typhoid
S. Typhi has also been reported in Kenya and fever. Failure of ciprofloxacin treatment of typhoid
Ghana [24]. fever occurred due to infection with such S. Typhi
In 2000, typhoid fever caused by strains of S. Typhi strains in Bangladesh, as in many other countries
exhibiting nalidixic acid resistance and decreased [13, 14, 16, 21]. These strains appear susceptible
ciprofloxacin susceptibility was detected for the when subjected to ciprofloxacin susceptibility testing
first time in Bangladesh. The isolation of such strains by disk diffusion method, or by current MIC break-
seemed to increase sharply in 2002. In addition, a points by NCCLS criteria but treatment failure still
large number of MDR S. Typhi isolates also exhibited occurs [13, 14]. To address this problem, many studies
decreased ciprofloxacin susceptibility in Bangladesh. have shown nalidixic acid resistance as a surrogate
Recently, MDR S. Typhi strains with decreased marker for decreased ciprofloxacin susceptibility
ciprofloxacin susceptibility, and strains exhibiting among S. Typhi [14, 21, 24]. But, recently, strains of
decreased ciprofloxacin susceptibility only have been S. Typhi with decreased ciprofloxacin susceptibility
reported in India [13], Bangladesh [16] and Kenya but susceptible to nalidixic acid were reported [24]
[24]. In Bangladesh, 74 % of S. Typhi strains iso- questioning the utility of nalidixic acid resistance
lated with decreased ciprofloxacin susceptibility were for detecting such strains. However, in our study
MDR compared to 50 % in the United Kingdom [14]. the ciprofloxacin (5 mg) disk diffusion test with inhi-
On the contrary, no association between decreased bition zone diameters of f24 mm as break-point
ciprofloxacin susceptibility and MDR phenotype had very good sensitivity and specificity for detecting
was observed among S. Typhi in a recent study in decreased ciprofloxacin susceptibility of S. Typhi
Kenya [24]. unlike ofloxacin disk that had low specificity [26].
With the decline of the MDR typhoid epidemic Thus, ciprofloxacin disk could be used to detect
in the mid-1990s in Bangladesh, it was expected that decreased ciprofloxacin susceptibility in S. Typhi,
the first-line conventional antimicrobial agents which appears to be a useful and easy screen for its
might once again become drugs of choice for the detection and future studies should evaluate clinical
treatment of typhoid fever [8]. With the recent outcome of treatment of typhoid fever caused by
emergence of MDR strains that have decreased sus- strains that show decreased susceptibility to cipro-
ceptibility to ciprofloxacin, however, therapy of floxacin. Moreover, the method is easily available in
typhoid fever in Bangladesh has become even more the laboratory, less expensive and user-friendly for
complicated. In such cases, ceftriaxone or cefixime guiding physicians to the proper treatment of typhoid
or azithromycin could be considered as possible fever.
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 06 Feb 2021 at 13:28:16, subject to the Cambridge Core terms of use, available at https://www.cambridge.org/core/terms
. https://doi.org/10.1017/S0950268805004759Decreased susceptibility to ciprofloxacin in MDR S. Typhi 437
Ciprofloxacin is widely used in Bangladesh to treat 4. Ahasan HN, Rafiqueuddin AKM, Chowdhury MAJ,
many infections without prescription and is likely to Azhar MA, Ara M, Farazi MA. Complications of
enteric fever encountered in medical wards. J Dhaka
result in high prevalence of resistance, limiting its
Med Coll 1993 ; 2 : 32–33.
utility [23, 27, 28]. A recent observation of R plasmid- 5. Wang F, Gu X, Zhang M, Tai T. Treatment of typhoid
mediated quinolone resistance in Enterobacteriaceae fever with ofloxacin. J Antimicrob Chemother 1989 ;
[29] is of great concern since this resistance gene 23 : 785–788.
could be disseminated rapidly across bacterial popu- 6. Jesudasan M, John TJ. Multiresistant Salmonella typhi
lations by conjugation. Hence, further studies are in India. Lancet 1990 ; 336 : 252.
7. Rowe B, Ward LR, Threlfall EJ. Spread of multi-
needed to detect mechanisms for decreased cipro-
resistant Salmonella typhi. Lancet 1990 ; 336 : 1065.
floxacin susceptibility of strains from Bangladesh. 8. Rahman M, Ahmad A, Shoma S. Decline in epidemic of
Finally, the development of resistance to cipro- multidrug resistant Salmonella Typhi is not associated
floxacin has been suggested as being due to exposures with increased incidence of antibiotic-susceptible strain
of these organisms to ciprofloxacin concentrations in Bangladesh. Epidemiol Infect 2002 ; 129 : 29–34.
9. Wallace M, Yousif AA. Spread of multiresistant
near their MICs [30]. With an increase in MIC of
Salmonella typhi. Lancet 1990 ; 336 : 1065.
ciprofloxacin in Bangladesh and other countries, 10. Rowe B, Ward LR, Threlfall EJ. Multidrug-resistant
effective use may require parenteral or higher Salmonella typhi : a worldwide epidemic. Clin Infect Dis
dosages to achieve serum levels required for effective 1997 ; 24 (Suppl 1) : S106–S109.
therapy ; however, the latter could have unwanted 11. Kariuki S, Gilks C, Revathi G, Hart CA. Genotypic
health consequences. Studies are necessary to address analysis of multi-drug-resistant Salmonella enterica
serovar typhi, Kenya. Emerg Infect Dis 2000 ; 6 :
these important issues. Continuous surveillance for
649–651.
the susceptibility patterns of S. Typhi isolates by 12. Zenilman JM. Typhoid fever. J Am Med Assoc 1997 ;
disk method is useful and easy if one uses a new 278 : 847–850.
break-point zone diameter of ciprofloxacin in evalu- 13. Chandel DS, Chaudhury R. Enteric fever treatment
ating the role of ciprofloxacin in the treatment of failures : a global concern. Emerg Infect Dis 2001 ; 7 :
762–763.
MDR typhoid fever. An effective programme to pro-
14. Threlfall EJ, Ward LR. Decreased susceptibility to
mote rational use of antimicrobial agents is essential ciprofloxacin in Salmonella enterica serotype Typhi,
to avoid a realistic threat of untreatable MDR United Kingdom. Emerg Infect Dis 2001 ; 7 : 448–450.
typhoid fever. 15. Rowe B, Ward LR, Threlfall EJ. Ciprofloxacin-resistant
Salmonella typhi in the UK. Lancet 1995 ; 346 : 1302.
16. Haque SMZ, Haq JA, Rahman MM. Nalidixic acid-
ACKNOWLEDGEMENTS resistant Salmonella enterica serovar Typhi with de-
creased susceptibility to ciprofloxacin caused treatment
The research was funded by ICDDR,B:Centre for failures : a report from Bangladesh. Jpn J Infect Dis
Health and Population Research, which is supported 2003 ; 56 : 32–33.
by countries and agencies which share its concern 17. Murdoch DA, Banatvala NA, Bone A, Shoismatulloev
BI, Ward LR, Threlfall EJ. Epidemic ciprofloxacin-
for health problems of developing countries and
resistant Salmonella typhi in Tajikistan. Lancet 1998 ;
USAID, Washington, DC, USA. We are grateful 351 : 339.
to all laboratory staff of Clinical Microbiology, 18. Parry CM, Wain J, Chinh NT, Vinh H, Farrar JJ.
ICDDRB, Dhaka, Bangladesh for their help in the Quinolone-resistant Salmonella typhi in Vietnam.
preparation of this manuscript. Lancet 1998 ; 351 : 1289.
19. Rodrigues C, Mehta A, Joshi VR. Salmonella typhi
in the past decade : learning to live with resistance.
Clin Infect Dis 2002 ; 34 : 126.
REFERENCES
20. Baur AW, Kirby VMM, Sherris JC, Turck M.
1. Thong KL, Puthucheary S, Yassin RM, et al. Analysis Antibiotic susceptibility testing by a standard single
of Salmonella typhi isolates from Southeast Asia by disk method. Am J Clin Pathol 1996 ; 45 : 493–496.
pulsed-field gel electrophoresis. J Clin Microbiol 1995 ; 21. Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ.
33 : 1938–1941. Typhoid fever. N Engl J Med 2002 ; 347 : 1770–1782.
2. Pang T, Buttha ZA, Finlay BB, Altwegg M. Typhoid 22. Anon. Incidence of typhoid fever, Dhaka 2001. Health
fever and other salmonellosis : a continuing challenge. and Sci Bull 2003 ; 1 : 13–14.
Trends Microbiol 1995 ; 3 : 253–255. 23. Mandal S, Mandal DM, Pal NK. Antimicrobial resist-
3. Akbar MS. Evaluation of chloramphenicol and ance pattern of Salmonella typhi isolates in Kolkata,
cotrimoxazole in the treatment of enteric fever. India during 1991–2001 : a retrospective study. Jpn
Bangladesh J Child Health 1986 ; 10 : 11–14. J Infect Dis 2002 ; 55 : 58–59.
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 06 Feb 2021 at 13:28:16, subject to the Cambridge Core terms of use, available at https://www.cambridge.org/core/terms
. https://doi.org/10.1017/S0950268805004759438 M. Rahman and others
24. Kariuki S, Revathi G, Muyodi J, et al. Characterization dysenteriae type 1 by PCR. Antimicrob Agents
of multidrug-resistant typhoid outbreaks in Kenya. Chemother 1994 ; 38 : 2488–2491.
J Clin Microbiol 2004 ; 42 : 1477–1482. 28. Piddock LJ, Ricci V, Pumbwe L, Everett MJ, Griggs
25. Parry CM. The treatment of multidrug-resistant DJ. Fluoroquinolone resistance in Campylobacter
and naldixic acid resistant typhoid fever in Viet species from man and animals : detection of mutations
Nam. Trans R Soc Trop Med Hyg 2004 ; 94 : 413– in topoisomerase genes. J Antimicrob Chemother 2003 ;
422. 51 : 19–26.
26. Mandal S, Mandal MD, Pal NK. Ofloxacin minimum 29. Tran JH, Jacoby JA. Mechanism of plasmid-mediated
inhibitory concentration versus disk diffusion zone quinolone resistance. Proc Natl Acad Sci USA 2002 ;
diameter for Salmonella enterica serovar Typhi isolates : 99 : 5638–5642.
problems in the detection of ofloxacin resistance. Jpn 30. Cullman W, Steiglitz M, Baars B, Opferkuch W.
J Infect Dis 2003 ; 56 : 210–212. Comparative evaluation of newly developed quinolone
27. Rahman M, Mauff G, Levy J, et al. Detection of 4- compounds, with a note on the frequency of resistant
qunolone resistance mutation in gyrA gene of Shigella mutants. Chemother 1985 ; 31 : 19–28.
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 06 Feb 2021 at 13:28:16, subject to the Cambridge Core terms of use, available at https://www.cambridge.org/core/terms
. https://doi.org/10.1017/S0950268805004759You can also read