Emocomponenti per uso non trasfusionale: aspetti biologici e nuove applicazioni cliniche - Maria Cristina Tirindelli Unità di Ricerca Ematologia ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Emocomponenti per uso non trasfusionale:
aspetti biologici e nuove applicazioni
cliniche
Maria Cristina Tirindelli
Unità di Ricerca Ematologia Trapianto Cellule Staminali
Medicina Trasfusionale e Terapia Cellulare
Università Campus BioMedico di Roma
Emocomponenti per uso non trasfusionale (EMCnT) Prodotti biologici ottenuti dal sangue umano omologo (da donatore sano) o autologo (dal paziente) Ai fini della qualità e sicurezza i processi di raccolta, preparazione, qualificazione biologica, caratterizzazione, tracciabilità del prodotto e rilascio per uso clinico avvengono in Strutture Trasfusionali accreditate Normativa Italiana per le attività trasfusionali EDQM Standard - ed. 18° - 2014 EMCnT : 1. Gel di fibrina 2. Plasma ricco in piastrine/Gel di piastrine (PRP/GP)
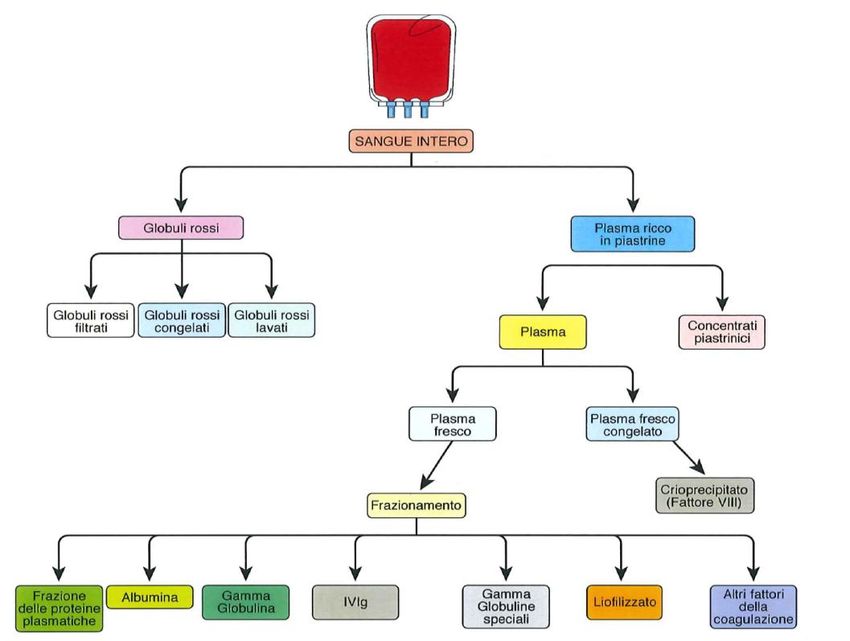
Emocomponenti per uso non trasfusionale (EMCnT)
Concentrati
Plasma Piastrinici
Trombina / Ca++ Trombina / Ca++
Gel di fibrina Gel di piastrine
Terapia Medicina
Trasfusionale rigenerativa
Gel di fibrina
Plasma/ Gel ricco in piastrine
Fattori di crescita delle piastrine
Emocomponenti per uso non trasfusionale (EMCnT)
PubMed search PubMed search
Item: Platelet Rich Plasma Item: Fibrin Glue
400 250
350
200
300
250 150
200
n. papers n. papers
150 100
100
50
50
0 0
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Totale 2373; 205 CRT Totale 1675; 155 CRT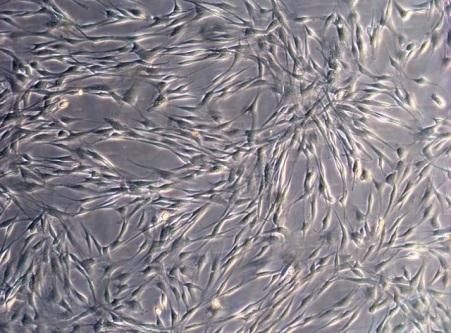
Emocomponenti per uso non trasfusionale (EMCnT)
Background dell’Unità di Ricerca e Ambiti di applicazione
Ematologia Ematologia
Area
Trapianto CSE Trapianto CSE
UdR Chirurgia Scienze
Rome Urologia Rome Oncologia Radioterapia
Ortopedia Plastica e Infermieristiche
Transplant Transplant
Ricostruttiva
Network Network
PRP PRP/GP PRP/GP/GF PRP PRP/GP/GF PRP PRP/GP PRP/GP/GF
Cistite
Malattie Cistite
Ulcere Attinica Mucosite Mucosite Mucosite Assistenza e
apparato emorragica
cutanee indotta da Indotta da indotta da monitoraggio
muscolo postrapianto
croniche Cistite CHT alte dosi CHT Radioterapia pazienti
scheletrico Allo CSE
interstiziale
Fase clinica Fase sperimentale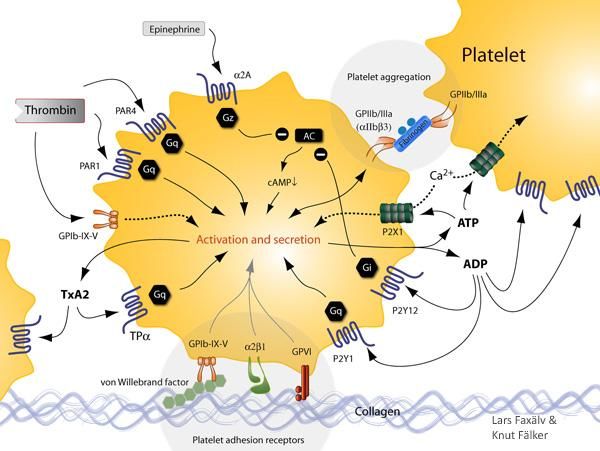
“Platelet Rich Plasma in treating CHT and RT induced mucositis” Mucositis of the gastrointestinal tract (GIM) caused by chemotherapy (CHT) and or radiation therapy (RT) occurs in approximately 20% to 40% of patients receiving conventional CHT and 80% of patients receiving high-dose CHT as conditioning for hematopoietic stem cell transplantation (HSCT). Oral mucositis presents as erythema and or ulceration of the mucosa. It is very painful, requiring opioid analgesics, and impairs nutritional intake and quality of life. Reduction in CHT regimen or treatment break can negatively influence prognosis. Economic Impact: nutritional support, secondary infection, hospitalization
OM and GIT mucositis WHO Grade 3 WHO Grade 4
“Platelet Rich Plasma in treating CHT and RT induced mucositis”
Relation to Horizon 2020 Work Program
The project refers to PHC 15 -2014/2015: Clinical research on regenerative medicine.
Specific challenge: Translating basic knowledge on regenerative effect of PRP into the clinic is the
main purpous of the project.
Scope: The proposal focuses on regenerative PRP based therapy which is ready for in-patient
research.
Specific research: WP1 Preclinical phase; WP2 Clinical phase
Regulatory requirements :for the use of PRP in clinical setting has been met with the release of
several laws by competent authority of Minister of Health in 2005 , 2007 and 2010 concerning
collection, manipulation, biological validation, labeling, storage, transport and intended clinical use of
human blood and his components.
Safety, efficacy and repeatability of PRP treatment will be tested in a preliminary clinical study
Stimulate the interest and growth of European small enterprise or industries operating in the
plasmaderivative sector is a further objective.Emocomponenti per uso non trasfusionale (EMCnT) “Platelet Rich Plasma in treating CHT and RT induced mucositis” Proprietà biologiche Rigenerazione e rimodellamento tessutale (K. Bieback Transfus Med Hemother 2013) Attività antimicrobica (Edelblute CM et al. Platelets 2014) Attività antinfiammatoria, antidolorifica (van Buul GM et al. Am J Sprt Med 2011)
Emocomponenti per uso non trasfusionale (EMCnT)
Scheme of the Work Plan
WP 1 Biological phase WP 2 Clinical phase
Collection of Platelet by apheresis Preliminary clinical study
Preparation of PRP (0.8-1.2 x106 plts/) PRP oral formulation tested in preliminary
Biological Validation of PRP clinical study in restricted number of
Characterization of PRP: hematologic and oncologic patients with
GFs (PDGF, VEGF, EGF, FGF, IGF, TGFβ) severe grade >2 OM complication
CK pro (TNFα, IL6,IL 8) /antinflamatory
(IL1-IL4, TNF RI, IL 10) Prospective randomized clinical study
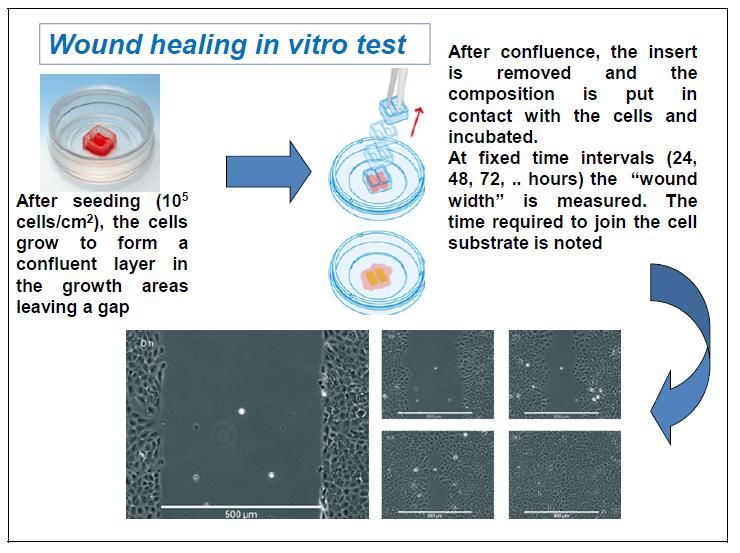
Evaluation of proliferative effect of PRP PRP oral formulation vs conventional
in MSC culture treatment will be used for
Formulation of oral PRP gel prophylaxis and treatment of OM an GIM
Release of PRP Formulation as product in 130 oncologic and hematologic patients
for topical use URs involved: RU 1,2,3,4,5,6
URs involved: RU 1 e 6Emocomponenti per uso non trasfusionale (EMCnT)
1500
Espressione GF (ELISA) 1000
VEGF
500
0
pg/ml PRP Lisato PRP PRP
sacca Regen da CB
4000
PDG-AB
2000
0
PRP Lisato PRP PRP
pg/ml
Espressione CK (FACS)
sacca Regen da CB
200 IGF-1
100
0
PRP Lisato PRP PRP da
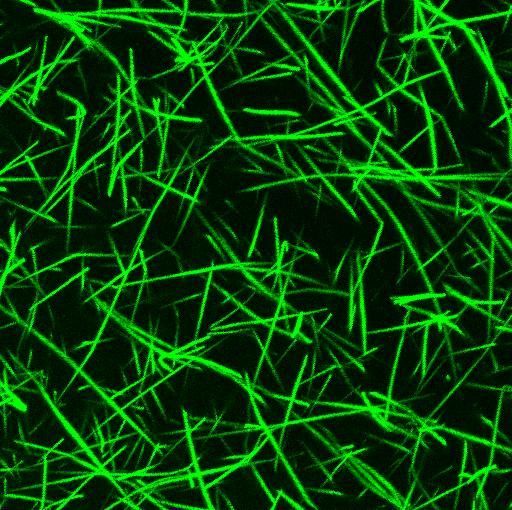
Colture cellulari MSC,
sacca Regen CB
fibroblastiEmocomponenti per uso non trasfusionale (EMCnT)
“Fibrin Glue therapy for severe haemorrhagic cystitis
after allogeneic stem cell transplantation”.
La cistite emorragica post trapianto, in particolare nella sua forma
refrattaria ai trattamenti convenzionali, è una complicanza maggiore del
trapianto allogenico di cellule staminali ematopoietiche.
Con sintomi che si esprimono da ematuria isolata fino all’insufficienza
renale, questa complicanza compromette in modo significativo la qualità di
vita dei pazienti, prolunga di settimane o mesi la loro ospedalizzazione e
nelle forme intrattabili può condurre il paziente all’exitus.Transplant Related Haemorrhagic Cystitis
– Incidence
12-25%
– Risk Factors
Allo HSCT
MUD/CB/Haplo
Myeloablative Conditioning (Cy-Bu)
Acute-GVHD >2nd grade
BK viruria +++
highly immunosuppressive regimensIncidence of HC as a function of donor type
L. De Padua Silva et al. Hematologica 2010
17Patients with BKV-HC required a significantly longer duration of
hospitalization (PTreatment HC Toxicity
Limited number
of patients
Different results
No established
criteria for
response
ToxicityJACIE Metropolitan Transplant Program
Coordinator:
William Arcese
University “Tor Vergata”, Rome
Ospedale
Sant’Andrea
ROME
Ospedale
Bambino Gesù Ospedale
SanGiovanni-Addolorata
Policlinico Universitario
Tor Vergata
Istituto Regina Elena
Ospedale
Sant’Eugenio Policlinico Universitario
Campus BiomedicoTransplant activity
January 2006 - December 2014
1698 HSCT
Pediatric
277 (16%)
Adults
1421 (84%)
Autologous Allogeneic
1005 (71%) 416(29%)Incidence of HC in Allogeneic Transplant
Allogeneic
416 HSCT – 407 Patients
Haemorrhagic Cystitis
85 (21%)
HLA SIB MUD UCB HAPLO
19/176 (11%) 19/101 (19%) 13/33 (40%) 34/98 (35%)
grade ≥ 2 HC
54
HLA SIB MUD UCB HAPLO
9/176 (5%) 13/101 (14%) 6/33 (18%) 25/98 (26%)
FIBRIN GLUE
YES NO
41 (76%) 13 (24%)Post engraftment HSCT- HC >2 grade
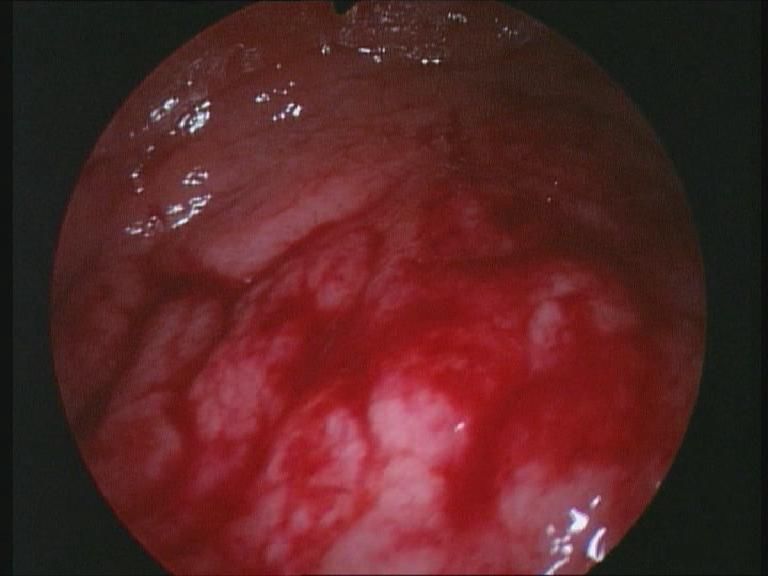
Transverse US image
through the bladder shows Cystoscopy
echogenic intravesicular debris
and diffuse bladder wall thickeningPatient and Transplant Characteristics
(n=41)
Age median (range) 35 (18-60)
Male 19 (46%)
Diseases:
Lymphoid 24 (59%)
Myeloid 17 (41%)
Conditioning not including CTX 37 (90%)
GVHD Prophylaxis
CSA ± MTX ± ATG ± MMF 23 (56%)
+ Basiliximab (Haplo) 18 (44%)
Acute GVHD ≥ II grade 13 (32%)
Engraftment median day (range) 18 (12-46)
Update
Tirindelli M.C. & Arcese W., Biol Blood Marrow Transpl., 2014Patient and HC Characteristics
(n=41)
Days to HC onset median (range) 34 (8-146)
HC Clinical Grade
Grade II 13 (32%)
Grade III 25 (61%)
Grade IV 3 (7%)
Neutrophils x 103 mL median (range) 5.2 (0.1 – 34.5)
Platelets x 109/L median (range) 29 (3-170)
Hb g/dL median (range) 8.7 (6.9-13)HC SupportiveTherapy prior to FG Therapy Patients % Hyperidration 24 59% Bladder irrigation 35 85% Cidofovir i.v. 16 39% Tranexamic acid 21 51% Transfusions RBC median 4 U (1-27) 37 90% PLTs median 18 doses (2-60) 35 85%
Fibrin Glue
Topical hemo-component Applicator
Human plasma derived
Mouldable matrix
Bioresorbable Processing unit
Matrix for cellular growth
Haemostasis
Tissue adhesion
Tissue sealing
Spray Fibrin
Vivostat SystemFibrin Glue Cystoscopy Procedure
Vivostat System
Applicator
Processing
unit
Spray Fibrin
Procedure Parameters
Type of Anesthesia Sedation and O2 Ventilation
Time for Cystoscopy 45 min (35-90)
Fibrin Glue Volume 12 ml30
Fibrin glue endoscopic application
A B C
D E FFibrin Glue Treatment
RESPONSE CRITERIA
Discontinuation of lower abdominal pain, dysuria,
Clinical Response
urge and frequency.
Regression of all symptoms and Absence of
Complete Remission haematuria.
Persistence of haematuria without reduction of HC
No Response
clinical grade.Fibrin Glue Therapy for ≥ 2 grade HC (n=41)
Pain Discontinuation Catheter Removal
97±3% 94±4%Fibrin Glue Cystoscopy Procedure
Applications Patients Responders No Responders Relapse
1 28 25 (89%) 3 7
2 10 8 (80%) 2 1
3 or + 3 2 (67%) 1 1
Total 41 35 (85%) 6 9Fibrin Glue Therapy for ≥ 2 grade HC
Complete Response Relapse
(n=41) (n=35)
85±3%
26±7%HC TRM and OS
HC and TRM HC and OS
Hassan Z, et al. Clin Transplant 2007 Cesaro et al. 2008, BMT 41: 363 35Matched Pair Analysis FG-HC vs No HC
FG-HC n = 35
No HC n = 35
No HC: 37±11%
FG-HC: 32±9%
p-value: NSConclusions
Fibrin Glue Therapy
for > grade 2 haemorrhagic cystitis
is a feasible, safe, not invasive,
easily repeatable, short consuming time
and slightly expensive procedure.Rome Transplant Network
HC-FG 2015 Study
Prospective, Multicentric, One Arm Trial
for Treating ≥ 2 grade Haemorrhagic Cystitis
with Endovesical Fibrin Glue
in Allogeneic Hematopoietic Stem Cell Transplant
(Prot. 23/15 ComEt CBM del 24/03/2015).
Gruppo Italiano per il Trapianto di Midollo
Osseo, cellule staminali emopoietiche e
terapia cellulareAknowledgements
Rome Transplant Network Centers
Urology Unit and Transfusion Medicine Service
Policlinico Campus Bio-Medico University
Urology Unit and Transfusion Medicine Service
Policlinico Tor Vergata University
RTN Data CenterEmocomponenti per uso non trasfusionale (EMCnT)
Ringraziamenti : Unità di Ricerca UCB – Unità Cliniche
Collaboratori:
Ematologia Trapianto Cellule Staminali Medicina Trasfusionale e Terapia Cellulare
Prof. Giuseppe Avvisati Medici: Carolina Nobile
Medici: Ombretta Annibali Fabiola Landi
Marianna De Muro Stefano Spurio
Elisabetta Cerchiara Biologhe: Barbara Giannetti
Chiara Sarlo Chiara Gregorj
Daniele Armiento Anna Maria Morgia
Alessandra Scardocci Tecnici: Melania Di Cerbo
Valeria Tomarchio Angela Calaciura
Specializzandi: F. Chiodi, S. Ferraro, P.Berti, Infermiere: F. Armeti, M. Nigro, S. Vaccaro,
M.Tafuri, A. Pagano Segreteria: Cecilia Tavani
Infermiere: Marzia Mazzaroni e
Team Infermieristico IEstYou can also read