Oral Health in Primary Care: A Framework for Action - American Association for Community Dental Programs National Oral Heath Conference, April ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Oral Health in Primary Care:
A Framework for Action
American Association for Community Dental Programs
National Oral Heath Conference, April 2015
Kathryn E. Phillips, MPH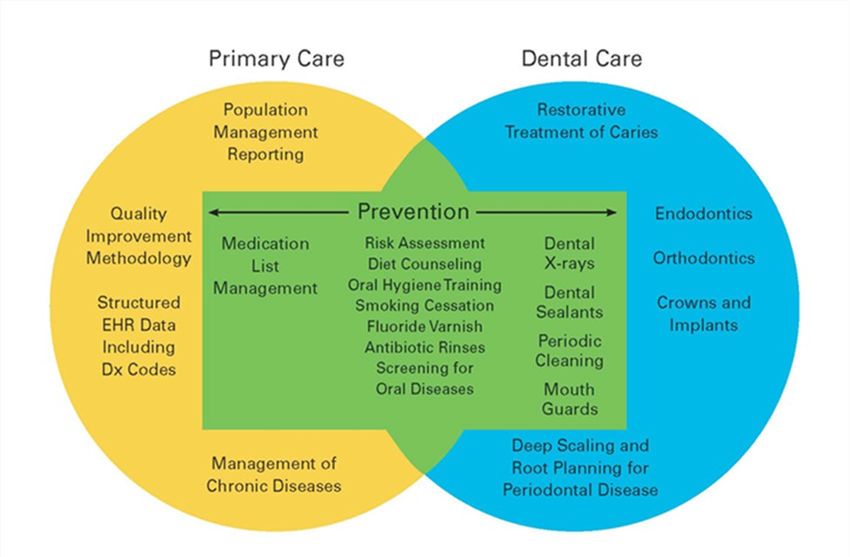
Who We Are
Qualis Health is one of the nation's leading population health care
consulting organizations. We work with public and private sector clients
to advance the quality, efficiency, and value of health care.
Kathryn E. Phillips, MPH, Program Director
Jeff Hummel, MD, MPH, Medical Director
Practice Transformation
Phone: (206) 288-2462 | Cell: (206) 619-7723
Toll-free: 1 (800) 949-7536 x 2462
e-mail: kathrynp@qualishealth.org
2
Objectives
• Describe the benefits of integrating oral health
preventive care in routine medical care
• Present an organizing framework for delivering
oral health preventive care in the primary care
setting
• Offer ideas on actions dentists can take to support
uptake
3
What Is the Problem We Are
Trying to Solve? A Prevention
Gap
• Oral disease is preventable
• Nationwide we have an unacceptably high burden of disease
• Little improvement in oral health status
• The oral health care system, as currently configured, fails to
reach the populations with the highest burden of disease,
resulting in significant and pervasive health disparities
4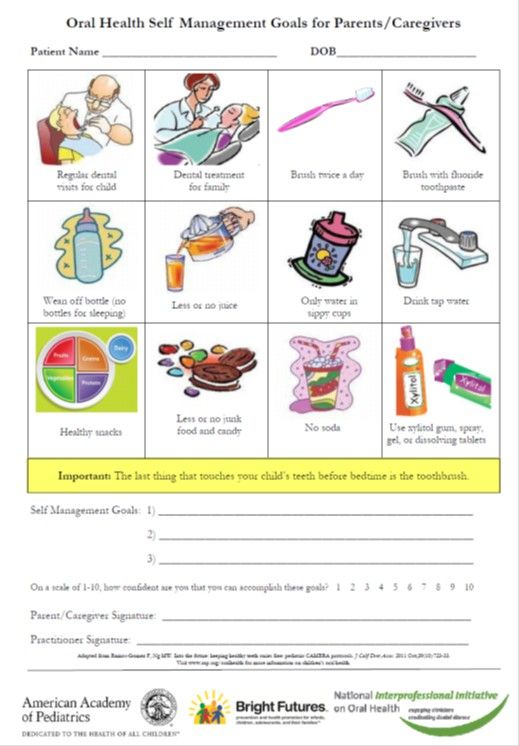
Access and Affordability Challenges
Dental care is the most common unmet health need
40% of the population lacks dental insurance
2.5x the % who lack medical insurance
• Even with insurance, dental care is often not
affordable
• 47 million people live in dental shortage
areas
5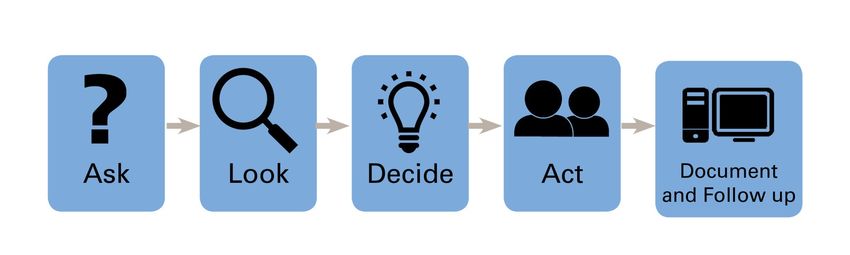
Results?
• Unnecessary complications
• Late-stage interventions
– Waste valuable resources
– Introduce significant risk for patients
– Do not address underlying cause of disease: bacteria
fueled by an unhealthy diet and ineffective hygiene
•Reliance on emergency department
• 2.1 million visits for non-traumatic oral
problems (2011)
6
So What’s the Answer?
Increasing access to affordable dental care is
important, but unlikely to reduce the burden of oral
disease–the need is simply too great.
We need another solution—
An upstream solution
• Incorporate oral health in routine medical care
• Apply a population-health-management-approach
to oral disease
• Find new ways to engage patients and families in
the prevention of oral disease 7
Why Primary Care?
Access
• Frequent contact with patients across the
lifespan, particularly high-risk groups:
Children, pregnant women, adults with
diabetes
Skills
• Prevention
• Patient engagement
• Care coordination
• Population-health-management approach
8
It’s a Natural Extension of What Primary
Care Teams Already Do
• Measure BMI and provide information about healthy diet
• Advise on sunscreen, look for suspicious moles, refer
• Screen new moms for depression
• Common problem, serious consequences
• Patient and family behavior (self-care) is key
• Most problems can be recognized early and treated to reduce
impact
9
Partners in Prevention
10What Will It Take to Change the
Standard of Care?
• Clear definition of what can be done in the primary care
setting to protect and promote oral health
• Streamlined process for fitting oral health into an already
packed primary care workflow
• Practical model for a close collaboration between medicine
and dentistry
11Oral Health in Primary Care Project
Informed by a technical expert panel
Primary care and dental providers; medical and dental
associations; payors and policymakers; patient, family, public
health advocates
Sponsor: Consultant:
Funders:
12Oral-Health-Delivery Framework
Solve the challenge:
How to fit oral health into an already packed workflow, in a way that:
1. Maximizes the value of the service to the patient and his/her family.
2. Minimizes disruption to all of the other priorities that a busy care
team is expected to manage.
3. Is perceived to be feasible across diverse primary care settings.
DRAFT 13Oral Health Delivery Framework
Symptoms & Risk
Signs of Disease
Factors
– Dry mouth
– Pain, bleeding – Chalk marks
– Burning, dry mouth – Obvious caries
– Dietary patterns – Inflammation
– Adequacy of fluoride – Exposed roots
– Oral hygiene – Mucosa abnormalities
– Time since last dental visit
On the most appropriate action using standardized criteria
based on the answers to the screening and risk assessment
questions and findings of the oral exam, and the values,
preferences, and goals of the patient and family.
DRAFT 14Oral-Health-Delivery Framework
Offer Intervention to Reduce Risk and/or
Refer for Treatment
1. Make changes in the medication list to protect the
saliva, teeth, and gums
2. Offer fluoride therapy
3. Offer dietary counseling to protect the teeth and gums
4. Demonstrate and coach good oral hygiene, for example
by using teach-back to model brushing and flossing
5. Offer therapy for tobacco, alcohol, or drug dependency
6. Refer for treatment
DRAFT 15Oral-Health-Delivery Framework
Document Findings and Measure Care
Processes
– Structured data
– Reporting functionality
– Measures to gauge impact on patients, families, practice
as a whole
DRAFT 16Who Will Do This New Work?
It depends.
• FQHCs with co-located dental practices or additional
resources will have additional options
17Structured Referral
• Many patients screened in the course of a primary care
visit will need care that only a dentist can provide
• Referrals to dentistry ought to be as smooth as
referrals to medical specialists:
– Referral network able to serve diverse patients
– Referral agreements to clarify expectations
– Tracking and care coordination processes
– Logistical support
– Connectivity; ability and commitment to
transfer information
DRAFT 18Importance of Structured Referrals
• The burden should not be on the patient and family to
transmit information between his/her primary care provider
and dentist
• Key lessons from behavioral health integration efforts:
– Primary care providers don’t want to uncover a problem
they can’t solve
– Must develop capacity for referral and treatment
– Screening results in increased referrals
DRAFT 19Why Now?
All the pieces are there.
• Delivery system “transformation”—advanced primary care
New expectations for how we engage and support patients
New staffing resources, new skills
Value-oriented payment on the horizon
• Oral health is the next frontier: opportunity to fulfill the
commitment to comprehensive, “whole-person” care
• Basic resources in places
Oral Health Delivery Framework provides action plan
20Conceptual Model
• Built on sound clinical concepts
• Informed by experience from recent efforts to integrate
behavioral health services
• Activities within scope of practice for primary care
Incremental Approaches
• Advanced practices have capacity to implement in full
• Others can take incremental approach while they continue
to build their capacity: process, population of focus
All primary care practices can take meaningful steps to
improve patient and family oral health 21Field-Testing a Conceptual Framework
12+ diverse primary care practices
Private practices (4) Safety net sites (2) with FQHCs (5)
adults with diabetes and co-located dental offices peds and adults with
pregnant women peds & all well visits diabetes
Project design under way: Kansas Association of the Medically Underserved (FQHCs)
Oregon Primary Care Association (FQHCs) 22Resources to Guide the Way
1. White paper—articulating the case for change (June 2015)
–. The Oral Health Delivery Framework
–. Case examples from early leaders
2. Implementation guide—toolkit for primary care practices
(2016)
–. Sample workflows
–. Referral agreements
–. Risk assessment/screening questions
–. Patient-education resources
–. Clinical-training resources
–. Case studies and impact data
Available at: www.safetynetmedicalhome.org
23What Can Dentists Do?
• Be a supportive referral partner
– Become a champion
– Offer your expertise
• Activate and support patients and families
– Raise awareness of the oral-systemic disease
connection
– Help reset social norms
– Ask: “What did your doctor say the last time she
checked your mouth?”
– Validate the role patients play in managing their own
oral health
24Supporting Actions from Stakeholders
• Assess adequacy of payment for oral health
preventive care; add payment for care
coordination
• Invest in research to strengthen the evidence base
for oral health preventive care:
– Validated screening questions to identify and monitor salivary
dysfunction, risk of caries in adults, and periodontal disease
– Clinical decision support tools to assist providers in managing
medication lists to reduce iatrogenic salivary dysfunction
– Benefits of fluoride varnish for adults
25Questions?
Reactions?
Ideas to share?
26You can also read