Evaluating Suspected Psychosis - Webinar | April 3, 2021 Aditi Sharma, MD - Seattle Children's
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Evaluating Suspected Psychosis
Aditi Sharma, MD
Webinar | April 3, 2021
Patrick
By the end of this presentation, the learner will be able to:
1. Define “psychosis”
2. Describe three possible causes of psychotic symptoms
3. Provide a differential diagnosis for suspected psychosis
• Objectives
4.
5.
Identify common features of prodrome of psychosis
Know when to refer for evaluation for early onset schizophrenia
Arabel
Case
• Zoe is a 12-year-old girl referred for an evaluation.
She and her family recently moved across the
country. Since that time, Zoe has been complaining
of headaches and stomachaches and has missed
several days of school due to not feeling well.
• Prior to this, Zoe had never been in mental health
treatment. She has a normal IQ and no learning
problems. Her academic and social functioning are
normal.Case continued
• On intake, Zoe endorsed many features of anxiety, sleep
problems, and hearing voices and her mother also
reported concerns about anxiety and sleep problems.
• Her parents were alarmed to learn that Zoe endorsed
hearing voices and expressed the fear that she might have
schizophrenia.Poll Question
Q. What percentage of 12-year-olds endorse
hallucinations when surveyed?
A. 17% (Kelleher et al)Are hallucinations the same as psychosis?
• No!
• 17% of kids and 8% of adolescents will answer “yes”
when asked if they see or hear things that other people
do not see or hear
• That does not mean they are psychotic
• But they are likely to have some kind of psychiatric
disorder
• The most common cause of hallucinatory experiences in
kids and adolescents?
• AnxietyWhat is psychosis?
• Loss of touch with reality, or impairment in reality testing
• This can look like:
• Hallucinations
• Delusions
• Disorganized thinking
• Disorganized behavior and speechHallucinations - definition • Sensory experiences that are generated by a person’s mind rather than something in the environment. • Common examples include hearing voices or seeing things
Delusions - definition • Fixed false irrational or bizarre beliefs – that lie outside the context of shared cultural and religious beliefs and experiences • Eg: “Knocking on wood” – not a delusion
Disorganized speech and behavior
• You know it when you see it
• Think of this when you are having trouble following
what a patient is saying, or getting a history of
symptomsCase, revisited
• At the initial interview, Zoe reports that she sees two
figures who speak to her. Their names are “Kyle” and
“Janie.” She describes them vividly and feels their
presence more strongly when she feels anxious and
when she goes to school.Case, revisited On interview, Zoe is well groomed and well spoken. She does not appear internally preoccupied. Her speech and thoughts are organized. Zoe is able to tell the examiner her birthday, the current date, and her new address. She has a euthymic affect when describing her hallucinations. She reports missing her old school and friends and is quite anxious about attending the new school and meeting new people. When the clinician suggests that she cannot miss more school, Zoe starts crying.
What features argue for psychosis? • Hallucinations
What features argue against psychosis?
• Good premorbid functioning
• Organized presentation, speech
• Intact self-care
• Hallucinatory experiences change based on context
• More common disorder would explain the
symptomsCase Wrap Up Clinical interview and historical features not consistent with a primary psychotic disorder: • Age (onset of true psychosis below age 13 years is rare) • High premorbid and current functioning (no learning disorders, no social problems) • Organized thinking on the mental status exam • Articulate and organized speech and behaviors • Intact self-care (good grooming and hygiene) • Highly organized description of the hallucinations • Report of hallucinations that are situationally specific (e.g., worse with anxiety and when she goes to school)
Psychosis is a symptom, not a diagnosis
• Just like pain
• You need to find the cause before you can choose a
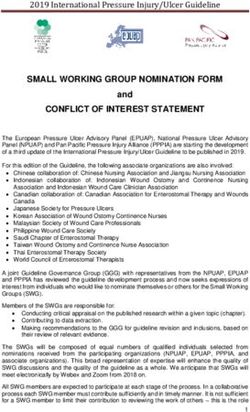
treatment (or at least have a working hypothesis)Assessment of Suspected Psychosis - Framework
Hallucinations,
"delusions," "paranoia"
Psychosis Psychosis mimicker
Medical Psychiatric Anxiety Depression
Mood disorder
delirium (e.g. bipolar Trauma Behavioral
disorder)
Primary psychotic
substance
disorder (e.g.
intoxication
schizophrenia)
genetic disorders
*This is conceptual and not intended to capture all
possible causes of hallucinations / delusionsPsychosis mimickers • Anxiety • Internal monologue / dialogue • Depressive ruminations • Borderline personality disorder • Trauma
Causes of Psychosis
Medical
• Delirium (acute)
• Autoimmune disorders (acute)
• Genetic disorders (more likely chronic)
Substances
• Cannabis (controversial)
• Stimulants
• Hallucinogens
• Alcohol withdrawal (hallucinations are a symptom
of life-threatening alcohol withdrawal)Causes of psychosis (2)
Psychiatric
• Depression (rare)
• Mania
• Primary psychotic disorder/schizophrenia
• Schizoaffective disorderOnce you know the symptoms are psychiatric in origin • Your goal should be to identify, is it a primary psychotic disorder, or is the psychosis (or quasi-psychosis) related to another mental disorder? • This matters because it affects treatment • Eg: You don’t want to treat “hallucinations” related to trauma with antipsychotic medications if you can help it.
What is a primary psychotic disorder? • Schizophrenia or schizophrenia spectrum disorder • Meaning, the core symptoms are the psychotic symptoms
Schizophrenia
• A chronic and severe disorder of neurodevelopment
• Onset occurs in adolescence or early adulthood
• Worldwide prevalence between 0.23-1%
• Childhood onset (< age 13) is rare
• If you find yourself diagnosing schizophrenia in a
patient 13 or younger, ask yourself how compelling
the case is
• Much more likely to be something else
• Three main categories of symptoms: positive, negative,
and disorganizationRisk Factors for Schizophrenia • Childhood disruptive behavior disorders • Academic challenges • Speech and language disorders • Social deficits
Positive Symptoms • Hallucinations • Delusions
Negative Symptoms Problems with thinking and functioning • Lack of motivation • Lack of speech • Flat affect Difficult to separate from comorbid depression Don’t respond very well to first-line medication
Disorganization • Disorganized speech • Loose associations • Tangential speech • Bizarre behavior • Poor attention • Catatonic behavior (general lack of response to one’s environment)
Case 2 Dan, a 17-year-old young man with a history of attention- deficit/hyperactivity disorder (ADHD) is brought to the pediatrician by his mother because he has become more withdrawn and isolated over the past 6 months. He rarely engages with friends and seems to go days without speaking to his parents. Dan’s grades have deteriorated, and he is no longer completing homework assignments. His grandmother, visiting from out of state, has noticed that his hair seems greasy and wonders if he has been changing his clothes. Dan seems to be awake late at night and spends a lot of time playing video games on his computer and reading message boards online.
Thoughts so far on Dan? • Speak up or write in the chat
Case 2 continued • On initial interview, Dan speaks quietly and makes little eye contact. He is disheveled and wearing clothes that are quite wrinkled. He answers questions briefly using one- to two-word answers and endorses feeling depressed, with decreased interest in previously enjoyed activities and low energy. • Dan’s pediatrician diagnoses him with depression and prescribes fluoxetine, an antidepressant medication. The pediatrician asks him to follow up in 6 weeks.
Case 2 continued • At the 6 week follow-up visit, Dan appears more disheveled and is slightly malodorous. He makes little eye contact and seems distracted. He takes a long time to answer questions. Some of the conversation is hard to follow because Dan’s sentences do not always make sense. He does not always seem to register what others say to him. His affect is flat. Dan’s weight is down 4 pounds since the initial visit. His mother shares that at the parent–teacher conference, his teacher commented that when he comes into the classroom, he seems confused and often takes a while to find his seat. Dan has been observed talking and laughing to himself at home and in school. His mother asks if his antidepressant needs to be increased or changed.
Case 2 wrap up
•• Features
Features of initial
of initial assessment
assessment thatevolving
that suggest suggestpsychosis.
evolving
psychosis.
• History: marked deterioration in functioning, social relatedness, and self-care
•areHistory: marked
all hallmark deterioration
prodromal symptoms ofinpsychosis.
functioning, social
relatedness,
• Observation: and Dan’s
On MSE, self-care areofall
paucity hallmark
speech prodromal
and lack of engagement is a
symptoms
sign of psychosis.
of developing thought disorder, and also might represent paranoia.
• Observation:
• At the follow-up
On both
visit,
MSE,history
Dan’s paucity
and exam
ofprovide
speech aand lack picture
clearer
of
engagement is a sign of developing thought disorder, and also
of psychosis.
might represent paranoia.
• Disorganized thought is demonstrated by Dan’s difficulty finding his seat in
• At the follow-up visit, both history and exam provide a
class and on exam by his speech pattern.
clearer picture of psychosis.
• Delayed responses to questions may reflect thought blocking.
• Disorganized thought is demonstrated by Dan’s difficulty
• More overthis
signs include others seeing Dan talking to himself, weight loss,
finding seat in class
and further decline in self-care
and on exam by his speech pattern.
• Delayed responses to questions may reflect thought blocking.
• More overt signs include others seeing Dan talking to himself,
weight loss, and further decline in self-care
Refer to psychiatry!Prodrome • Functional deterioration that presents before the onset of obvious symptoms • Social withdrawal and isolation • Decreased self-care • Odd or bizarre preoccupations and behaviors • Academic decline
Treatment • Effective treatment is a combination of psychosocial interventions and medications • Psychosocial interventions help with functional deficits • Vocational training • Social skills training • Independent living support • Medications may help reduce core symptoms
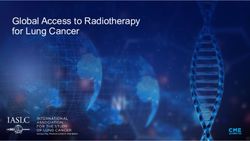
Assessment of Suspected Psychosis - Framework
Hallucinations,
"delusions," "paranoia"
Psychosis Psychosis mimicker
Medical Psychiatric Anxiety Depression
Mood disorder
delirium (e.g. bipolar Trauma Behavioral
disorder)
Primary psychotic
substance
disorder (e.g.
intoxication
schizophrenia)
genetic disorders
*This is conceptual and not intended to capture all
possible causes of hallucinations / delusionsSummary • True psychosis in children is extremely rare • Diagnosis should be made based on history and observation, and should be re-evaluated regularly • Underlying causes for psychosis should be ruled out before making a diagnosis of a primary psychotic disorder like schizophrenia • Treatment is multimodal
• Objectives – did we achieve?
By the end of this presentation, the
learner will be able to:
1. Define “psychosis”
2. Describe three possible causes of
psychotic symptoms
3. Provide a differential diagnosis for
suspected psychosis
4. Identify common features of
prodrome of psychosis
5. Know when to refer for evaluation
for early onset schizophrenia
ArabelAny Questions?
OliviaYou can also read