ALTERNATIVE HAT FOR IRRITABLE BOWEL SYNDROME - Judy Huang Gastroenterologist
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ALTERNATIVE HAT
FOR
IRRITABLE BOWEL SYNDROME
Judy Huang
Gastroenterologist
Objectives ■ What is Irritable Bowel Syndrome? ■ Management for irritable bowel syndrome ■ Alternative management for irritable bowel syndrome – Complementary and Alternative Medicine
■ First described 1771
■ Most common GI condition
• 20-25% of general population
• Up to 50% of all referrals to Gastroenterologists
• Male: Female= 1:2
• 50% < than 35 years old
• Huge health burden
• >200 billion USD world wide per year
What is Irritable Bowel Syndrome?
■ Uncertain
■ Multifactorial
■ A gastrointestinal syndrome characterized by chronic pain and altered bowel
habits in the absence of any organic cause”
• Gastrointestinal motility
• Visceral Hypersensitivity
• Inflammation
• Alteration of gut flora
• Small Intestinal Bacterial Overgrowth (SIBO)
• Food intolerance
• Genetics
• Psychological
Initial assessment Rome IV
• Recurrent abdominal pain at least 1
• History day/week in the last 3 months,
• Rome IV criteria associated with two or more of the
following criteria:
• Alarm symptoms
• Related to defecation
• Weight loss, PR bleed, nocturnal symptoms • Associated with a change in
• IBD red flags frequency of stool
• Associated with a change in form
• Family history: colon cancer, IBD, coeliac (appearance) of stool
• Diet
• Medication
• Blood tests: coeliac serology, TFTs, CRP, Calcium
• Faecal spec: calprotectin, MC&S, C diff
Conventional treatments ■ IBS-C – Increase soluble fibre – Osmotic laxative ■ IBS-D – Decrease fibre – Loperamide – Rifaximine – Cholestyramine ■ IBS-Mix ■ Anti-spasmodics ■ TCAs and SSRI ■ Diet ■ Psychotherapy
Any Alternatives?!? ■ Herb ■ Peppermint ■ Turmeric ■ Acupuncture ■ Probiotics ■ Psychotherapy ■ Hypnotherapy

Complementary and Alternative Medicine
(CAM)
■ CAM refers to healthcare systems, practices and products that are not
considered part of conventional medicine. ( NCCAM)
■ Complementary: use of CAM as adjunct to conventional medicine
■ Alternative: use of CAM as a substitute for conventional medicine
■ Increasingly accepted
– 50% of IBS patients use CAM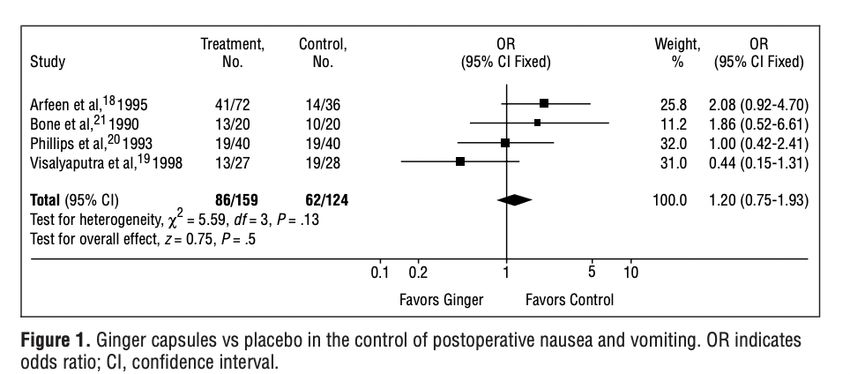
Traditional Chinese Medicine
• In TCM, IBS is classified as “abdominal pain,” “Xiexie” and
“Yuzheng.” The etiology of IBS is summarized as abnormal of
emotion, diet, and external evil. Liver depression and spleen
deficiency, kidney yang deficiency, cold, and heat are regarded as
the key factors of IBS.
• Traditional Chinese Medicine
– Tong Xie Yao Fang: up to 20 Chinese herbal ingredients
– Feng feng, Xiang Fu, Chai Hu, Bai Zhu
• Acupuncture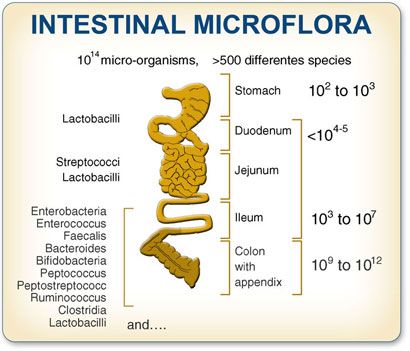
• Most studies have major flawed design. Poor quality studies. Conflicting results
• Chinese study. Randomized double blinded study. TCM vs Placebo
• TCM with 11 herbs vs Placebo for 8 week
• 119 patients: TCM ( 60), Placebo (59)
• Week 8: 35% vs 44% p=0.38, week 16:31.7% vs 33.9%, p=0.62
• TCM did not improve IBS symptom
The American Journal of Gastroenterology 101, 1574-1580 (July 2016)Herbal medicine
• Evidence
– Blinded. Randomised control study: 116 IBS patients
– Australian study
– Standard vs individualised vs placebo
– 5 capsules 3 times day for 16 weeks
– Assessed every 2 weeks with TCM and Gastroenterologists
• Both standard and indiviualised were equally effective at end of the treatment
• But only individualised group sustained the response after 3 months
JAMA. 1998;280:1585-1589.Iberogast • Developed in Germany in 1961 • STW5: liquid formula of 9 herbs • Herbs: bitter candytuft (Iberis amara), angelica root (Angelicae radix), milk thistle fruit (Silybi mariani fructus), celandine herb (Chelidonii herba), caraway fruit (Carvi fructus), liquorice root (Liquiritiae radix), peppermint herb (Menthae piperitae folium), balm leaf (Melissae folium) and chamomile flower (Matricariae flos) • Regulations of peristalsis, reduces acid and gas productions, local anaesthetic effect • NZ: 50mls, $47.60. 20 drops TDS
• Literature review summarizes safety and efficacy data of 12 clinical trials using STW 5 in IBS since 1990 • On average, Iberogast to treat symptoms 20% better than placebo, and the proportion of patients with complete relief was more than 50% greater than placebo • ADRs: 0.04% hypersensitivity reaction
Peppermint
• Oil extract of the Mentha piperita Linnaeus plant
• Active ingredient is menthol which is a cyclic monoterpene, it acts a smooth muscle relaxant
• Antispasmodic
• IBS and dyspepsia treatment
• ACG recommendation
– “We suggest the use of peppermint to provide relief of global IBS symptoms. Conditional
recommendation; low quality of evidence.”• Significant improvement in abdominal pain, IBS symptoms and improve quality of life • Safe profile • Heartburn and perianal burning sensation
Ginger Aloe vera
■ Used for nausea and vomiting ■ IBS-C
■ No improvement over placebo group ■ Anthraquinones
■ ? Prevent seasickness and hyperemesis ■ No data
Turmeric
■ Asian spice
■ 72mg vs 144mg daily for 8 weeks
■ Improve IBS symptoms but not QoL.
■ lack of double blinded placebo controlAcupuncture ■ Used in China for 5000 years history for various condition ■ Theory: channels of internal energy ( Qi), run through the body. through meridians. Hence body or organ function can be regulated by activating Qi with needle applications at acupoints.
• Poor quality study. Little information available. • Therapeutic value is unclear. Difficult to design “ control/placebo” group • Multiple small studies have reported that acupuncture increase pain threshold and improve IBS n QoL • Acupuncture vs sham acupuncture
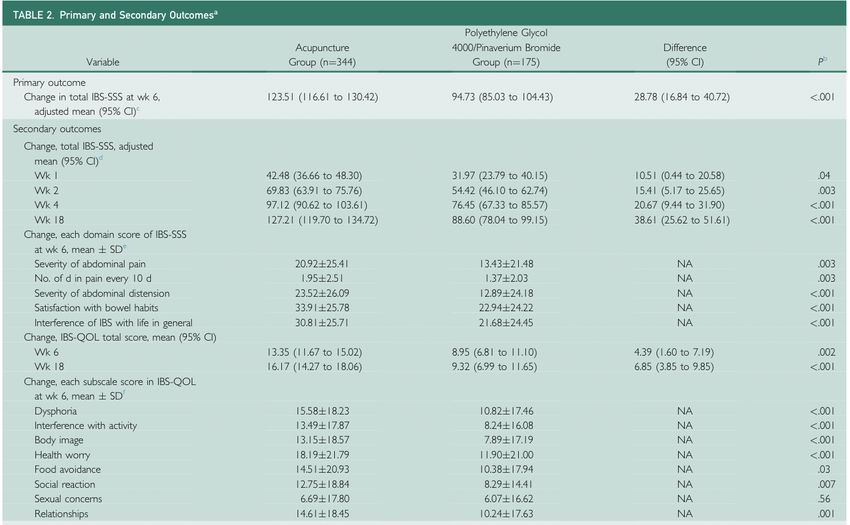
Effect of Acupuncture in Patients With Irritable Bowel
Syndrome: A Randomized Controlled Trial
■ Multicenter RCT
– 7 hospitals in China
– May 2015 to June 2018
■ Rome III
■ Acupuncture 18 sessions
■ IBS-C: PEG, IBS-D: pinaverium bromide
■ Total of 519 patients
– 344 vs 175
Mayo Clin Proc. 2020;95(8):1671-1683■ Study on 230 IBS patients
■ RCT
– Acupuncture, sham acupuncture
or waiting list
■ in the first 3 weeks, both true and
sham received ”only sham”,
■ Questionnaire at week-3 and week3
Am J Gastroenterol. 2009 Jun;104(6):1489-97CA TREATMENT TRIAL OF ACUPUNCTURE IN IBS PATIENTS
■ Results
■ Acupuncture vs Sham:
■ IBS-GIS: 41% VS 32% P=0.25
■ Acupuncture, Sham vs Waitlist
– IBS-GIS: 37% vs 4%, pYoga
■ Few trials
■ 25 adolescents 8 weeks of yoga v waitlist
– 1hr session, followed by 4 weeks of video practice
– Reduced GI symptoms and anxiety
– Improved QoL
■ 21 male IBS-D: yoga vs loperamide
– Overall GI symptoms reducedPsychotherapy and Hypnotherapy
■ Cognitive Behavior Therapy?
■ Gut-directed hypnotherapy: focusing on improving both psychological wellbeing and GI
symptoms
■ Most of the therapy consisted of 12 sessions in 3 months
■ Effectiveness has been supported by trials and and literature reviews
■ ACG
– We suggest that gut-directed psychotherapies be used to treat global IBS symptoms.
Conditional recommendationsGut Flora
■ Community of microbiome
– 300 - 1000 different bacterial
species
■ Composition of colonic microbiome is
altered and become unstable in IBS
■ Function
– Direct inhibition of pathogens
– Developing intestinal epithelium
– Metabolism
– Gut brain axisProbiotics
■ Live microorganisms which can alter colonic fermentation and stabilize gut flora
– Deliver healthy benefit
■ Growing interest in public and medical field: role of microbiome
■ ACG and Many international guidelines
■ “ We suggest against probiotics for the treatment of global IBS symptoms. Conditional recommendation; very low level
of evidence”■ Metanalysis ( 37 trials)
– Does it work?
– Combination probiotics demonstrated a pooled effect (RR 0.79, CI 0.68–0.91) for symptom
improvement, but there was evidence of significant heterogeneity (I2 5 72%) and publication bias
– What specie?
– Single species studies were less impactful
– Lactobacillus spp., Bifidobacterium spp., and Saccharomyces spp. did not seem to have a
significant pooled benefit.
– What strains?
– Bifidobacterium infantis 35,624 (106 , 108 , and 110 cfu/mL) or placebo (153). Symptom
improvement was reported in the group receiving 108 cfu/mL
– because the lack of dose response was challenging to explain.
– Symptoms targeting?
– Modest improvement in abdominal pain , no improvement in bloatingFaecal transplant
■ ONLY approved indication if for severe refractory C.Diff colitis
– Failed metronidazole and oral vancomycin
■ Literature Reviews and Metanalysis
– Patients who received donor FMT reported a 49.3% response rate compared with a
51% response rate in those who received placebo FMT. No significant difference
was noted in global IBS symptoms in patients who received FMT compared with
placebo (RR 0.93; 95% CI 0.48–1.79, P 5 0.83).
– FMT group could leave more IBS-D and bloating
■ Not enough evidence to support it. More research is required.
■ Risk vs benefit
■ ACG
– We recommend against the use of faecal transplant for the treatment of global IBS
symptoms. Strong recommendation; very low quality of evidencePotential Benefit with Complementary and Alternative
Medicine in Irritable Bowel Syndrome: A Systematic Review
and Meta-analysis
■ For overall response in IBS, herbal therapy, dietary supplements, and mind-body–
based therapy were significantly better than placebo or sham (relative risk range,
1.6–2).
■ For abdominal pain, herbal therapy was the only intervention with significant benefit
(standardized mean difference [SMD], 0.47), although mind-body–based therapy
showed a benefit with borderline statistical significance (SMD, 0.29).
■ Body-based and energy-healing therapies were no better than placebo or sham for
overall response or abdominal pain.
■ Overall evidence quality was rated as poor, with significant heterogeneity for most
analyses.
Charles J. Kahi, MD, MS, reviewing Billings W et al. Clin Gastroenterol Hepatol 2020 Sep 19Summary ■ Irritable Bowel syndrome is common and can be debilitating ■ Important to rule out organic cause ■ Although small studies, some data available ■ For overall response in IBS, herbal therapy, dietary supplements, and mind-body–based therapy were better than placebo or sham
You can also read