Juvenile Idiopathic Arthritis: Patterns, Problems, and Prognosis Disclosures - Ohio Association of Rheumatology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

9/1/2021
Juvenile Idiopathic Arthritis:
Patterns, Problems, and
Prognosis
Ohio Association of Rheumatology
August 21, 2021
Ed Oberle, MD RhMSUS
Pediatric Rheumatology
1
Disclosures
• None
2
1
9/1/2021
Objectives
• Define the clinical subtypes of JIA and recognize the similarities
to and differences from adult forms of arthritis.
• Describe the current treatment options and management of
patients with JIA.
• Predict potential complications associated with JIA as to best
manage them through their transition to adult rheumatology
care.
3
Primary inflammatory arthritis
Adapted from Nigrovic 2013
4
2
9/1/2021
Juvenile Idiopathic Arthritis
• Arthritis lasting longer than 6 weeks
• Age of onset before age 16 yo
• Diagnosis of exclusion
• Umbrella term for group of disorders that share arthritis
• Chronic, unregulated inflammation resulting in synovial
proliferation and bony destruction
5
JIA
• Most common rheumatic disease in childhood
• Prevalence 1/1000 children* (likely underestimated)
– 300,000 infants to teens in the US
• Can cause permanent damage to joints and eyes
• For > 60% JIA is a life-long illness with a high risk of
disease and treatment related morbidity
Guzman 2014
6
3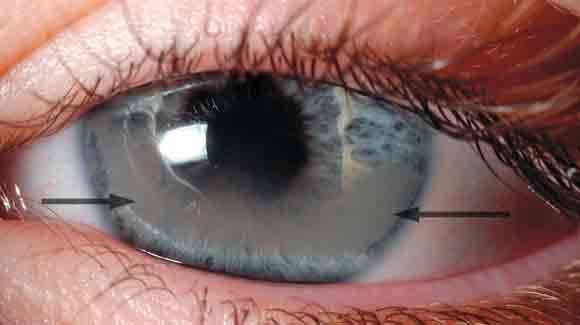
9/1/2021
Incidence
Girls Boys
Krause 2016
7
Classification Schemes
8
4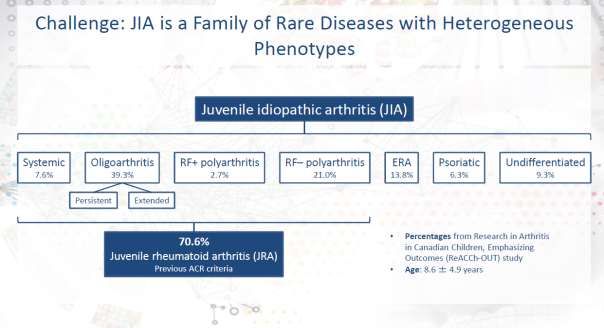
9/1/2021
Slide repurposed from R. Yeung 2019
9
Oligoarticular
Gowdie 2012
10
5
9/1/2021
Oligoarticular
• Most common of all JIA, ~40%
• Peak age: 2-4 yo
• F >>> M
• HLA associations – A2, DRB1, DQA1
• Highest ANA positivity
• Normal labs
Ravelli 2007
11
Oligoarticular - Natural course
1. Monophasic
2. Persistent oligo
– Remains 4 or less joints
– Less destructive
– Persists into adulthood < 25%
3. Extended oligo
– Spreads to 5 or more joints
– Behaves like Poly JIA
– Predictors of evolution: high ESR, upper extremity involvement, symmetry
– Persists into adulthood = 60%
12
6
9/1/2021
Polyarticular
13
Polyarticular
• Rheumatoid Factor – Negative (80%)
– ~20% of all JIA
– Biphasic Subsets
• Early 2-4 yo, F >>M 1) Similar to Oligo: young, ANA,
asymmetrical, uveitis
• Later 8-12 yo, F>M
2) Seronegative adult RA: symmetric, large
– HLA associations: DRB1 and small, elevated ESR, neg ANA
– Various joint distribution
– Remission by adulthood = 20%
14
7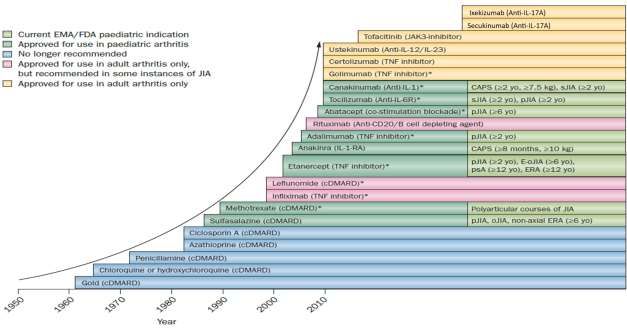
9/1/2021
Polyarticular
• Rheumatoid Factor – Positive (20%)
– 2-7% of all JIA
– F >> M, early adolescence
– Nodules possible
– Symmetrical, erosive
– Rarely remits before adulthood
– CCP positivity
– HLA DR4 and DR1
15
Psoriatic
Gowdie 2012
16
8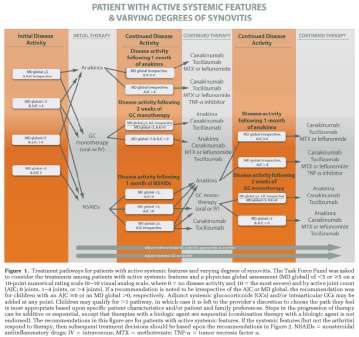
9/1/2021
Arthritis and psoriasis, or arthritis and at least 2
of the following:
Psoriatic 1. Dactylitis
2. Nail pitting or onycholysis
3. Psoriasis in a first-degree relative
• 2-11% of all JIA
• Biphasic
– 2-4 yo then 9-11 yo
– F>M
• Monoarticular
• Polyarticular
• Sacroiliitis
17
Enthesitis Related Arthritis
enthesis.info 2015
juvenilearthritisinfo Poggenborg 2015 ARD
18
9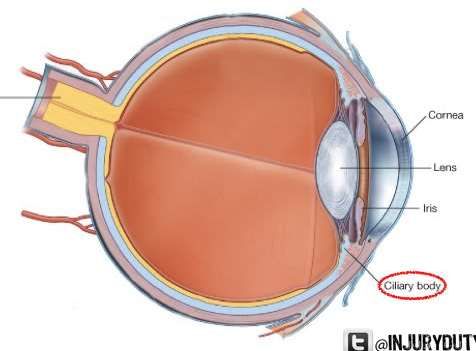
9/1/2021
Enthesitis Related (ERA)
Arthritis and enthesitis, or arthritis or enthesitis with at least 2
of the following:
1. The presence of or a history of sacroiliac joint tenderness
and/or inflammatory lumbosacral pain
2. The presence of HLA-B27 antigen
3. Onset of arthritis in a male over 6 years of age
4. Acute (symptomatic) anterior uveitis
5. History of ankylosing spondylitis, enthesitis related arthritis,
sacroiliitis with inflammatory bowel disease, Reactive
Arthritis, or acute anterior uveitis in a first-degree relative
19
ERA
• 3-11% of all JIA
• Late childhood or adolescence
• M >> F
• Chronic arthritis of axial & peripheral skeleton
• Uveitis usually acute, symptomatic, unilateral & recurrent
• Lower likelihood of remission, HLAB27 positive patients
20
109/1/2021
Systemic
• High CRP and ESR
• Leukocytosis
• Thrombocytosis
• Microcytic Anemia
• Transaminitis
Ravelli 2007
21
Systemic
Arthritis in one or more joints with or preceded by fever of at least 2
weeks’ duration that is documented to be daily (“quotidian”) for at
least 3 days, and accompanied by one or more of the following:
1. Evanescent erythematous rash
2. Generalized lymph node enlargement
3. Hepatomegaly and/or splenomegaly
4. Serositis
22
119/1/2021
Systemic Onset
• 4-17% of all JIA
• Any age
• F=M
• Unclear etiology
23
Biphasic Course
Nigrovic 2014
24
129/1/2021
Genetic Basis
Nigrovic 2018 A&R
25
26
139/1/2021
27
New proposed classification scheme 2019
• A) Systemic JIA
– Quotidian fever for at least 3 consecutive days, recurring over at least
2 weeks, and accompanied by 2 major criteria or 1 major and 2
minor criteria
– Major: (1) Evanescent rash; (2) arthritis
– Minor: (1) Generalized lymph node enlargement or Hepato- or
splenomegaly; (2) serositis; (3) arthralgia lasting at least 2 weeks; (4)
leukocytosis > 15,000/mm3 with neutrophilia
28
149/1/2021
• B) RF-positive JIA
– Arthritis for 6 weeks
– RF positive x 2 or CCP positive x 1
• C) Enthesitis/spondylitis-related JIA.
– Peripheral arthritis and enthesitis, or
– Arthritis or enthesitis, plus ≥ 3 months of inflammatory back pain
and sacroiliitis on imaging, or
– Arthritis or enthesitis plus 2 of the following:
• (1) sacroiliac joint tenderness; (2) inflammatory back pain; (3) presence of
HLA-B27 antigen; (4) acute (symptomatic) anterior uveitis; and (5) history of a
SpA in a first-degree relative.
29
• D) Early-onset ANA-positive JIA
– Arthritis beginning before the seventh birthday and accompanied by
a positive antinuclear antibody (ANA) at a titer of ≥ 1:160, twice at
least 3 months apart.
• E) Other arthritis
– Arthritis for ≥ 6 weeks
– Does not fit criteria for disorders A to D Psoriatic????
• F) Unclassified arthritis
– Arthritis for ≥ 6 weeks
– Fits > 1 disorder A-D
30
159/1/2021
Treatment
https://juvenilearthritisnews.com/2018/08/02/juvenile-arthritis-making-injections-easier/
http://www.pmmonline.org/page.aspx?id=1471
31
Early Referral = Better Outcomes
Wallace 2014 J Rheum
32
169/1/2021
Getting patients started on treatment
ED
PT
EcErlane 2016 Rheum
Adib 2008 Foster 2007 A&R
33
Treatment
• Goals of treatment
– Regain/Retain function
– Reduce/Eliminate inflammation
– Pain management
• Foundation: Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
34
179/1/2021
Evolution of Treatment
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
35
cDMARDs – Conventional Disease Modifying Anti-rheumatic Drugs
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
36
189/1/2021
Dose
=
Methotrexate -- recommended initial therapy with polyarticular disease
- often in conjunction with other biologic DMARDS
- generally well tolerated (nausea)
- no significant risk of infection or hepatitis
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
37
Start of the Age of Biologics – Infliximab 1998
- Revolutionized treatment of inflammation by
directly targeting component of inflammatory
cascade.
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
38
199/1/2021
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
39
V
Hinze 2015 Nat Rev Rheum
Physical Therapy
Corticosteroids – Oral, IV, Intra-articular
NSAIDs
40
209/1/2021
Consensus Treatment Plans
Ringold 2018 A&R
41
CARRA
• Investigator led research network for pediatric
rheumatology, started 2002
• 71 active sites, >600 members
▪ >90% of pediatric rheumatologists in North America
▪ Trainees, coordinators, stakeholders, researchers
• Strategic partnership with Arthritis Foundation
since 2015
• Parent/Patient engagement in all facets of
research
• Registry > 11,000 patients (10k JIA)
• Biorepository
Updated 3/2021
42
219/1/2021
Systemic JIA Treatment
• Initiation of IL-1 inhibitor in 9 soJIA patients (x-axis in months)
Pascual 2005 JEM
43
44
229/1/2021
Monoarticular Arthritis
• NSAIDs alone
• NSAIDs followed by IACI if not resolved by 2 months
• Initial IACI
• Probability of remission in first month on NSAIDs = 5%
– 16% by 2 months
• NNT to avoid IACI 3.8
• Additional cost of 6.7 months of active arthritis
Beukelman 2008 A&R
45
Polyarticular = Early Aggressive Treatment
MTX, Etanercept, and rapid steroid wean
MTX monotherapy
Wallace 2012 A&R Tynjälä 2010 ARD
46
239/1/2021
New POLY JIA Guidelines
• Arthritic Care & Research
• Arthritis & Rheumatology
47
Enthesitis or Sacroiliitis
+ NSAID
+ TNF inhibitor
-skip methotrexate
+ Sulfasalazine if TNF contraindicated
48
249/1/2021
Clinically Inactive Disease
1) no active joints
2) no fever, rash, serositis, splenomegaly or generalized lymphadenopathy attributable
to JIA
3) no active uveitis
4) normal ESR and/or CRP
5) PhysGA that indicates no disease activity = 0
6) duration of morning stiffness of ≤15 minutes
Clinical remission on medication - the criteria for inactive disease on medication had to
be fulfilled for a minimum of 6 continuous months
Wallace 2011
49
When to stop treatment?
Horton 2017 J Rheum
50
259/1/2021
Likelihood
to stop by
subtype
Horton 2017 J Rheum
51
How long to wait when How to stop?
clinically inactive?
Horton 2017 J Rheum
52
269/1/2021
Relapse is common 75% flared(range 3-109 m)
After 1 year, only 31% still in remission
- median to flare after 1 year = 53 months
349 patients treated with biologics
135 (38.6%) achieve remission 6 months
87 Etanercept
27 Adalimumab
12 Infliximab
7 Anakinra
1 Rituximab
1 Abatacept
68% children also on MTX
20 month median time period disease inactivity
53
54
279/1/2021
JIA extending into adulthood
RF positive Poly
RF negative Poly
Proportion of
Systemic
patients NOT in
Oligo
remission
Oen 2002
55
Complications of JIA
56
289/1/2021
Uveitis
Cornea
Lens
Iris
Choroid Ciliary
body
57
Uveitis
• Risk Factors:
– ANA +
– High ESR
– Young
•Oligo, persistent 16-18%
•Oligo, extended 25-30%
•Poly, RF neg 4-14%
•Poly, RF pos 0-2%
•Psoriatic 10%
•Systemic 1%
Saurenmann 2007
58
299/1/2021
Active Uveitis
• Chronic, non-granulomatous, anterior uveitis
• Affects iris and ciliary body
• Can lead to permanent blindness
• Insidious, asymptomatic
• Unilateral or bilateral
• Relapsing or chronic, does not parallel arthritis
59
Ravelli 2007
60
309/1/2021
61
Uveitis
62
319/1/2021
Uveitis Screening
3 months
Oligo/Poly/PsA ANA +
onset ≤ 6 yo ANA –
6 months
ANA +
onset > 6 yo
ANA –
12 months
Systemic/ERA Any
Heiligenhaus 2007
63
Disordered Growth
• Arthritis < age 9 = Excess growth
– Affected leg ≤ 3 cm longer
• Arthritis > age 9 = Premature closure
– Affected leg ≤ 6 cm shorter
Ansell 1956 Ann Rheum Dis
Simon 1981 JBJS
64
329/1/2021
Asymmetric Growth
65
Magni-Manzoni 2012 Nat Rev Rheum
66
339/1/2021
Growth Retardation
67
Woo P (2006)
68
349/1/2021
Osteopenia
69
Micrognathia
70
359/1/2021
Spinal Fusion
71
Extraarticular Complications
• Eye disease
• Amyloidosis
• Reproduction
• Cardiovascular Risk
• Associated Autoimmunity
72
369/1/2021
Psychosocial
• Social dysfunction
• Poor self body-image
• Vocational failure
• Anxiety/depression
• Adult patients with JIA often cope with illness more poorly
than like-aged patients with arthritis of adult onset
73
Mortality
– As adults, mortality rate of 0.27 deaths per 100 years of patient
follow up
– Compared expected rate of 0.068 deaths
– Complications of Chronic autoimmune hepatitis, CVID, Insulin-
Dependent Diabetes, Grave’s disease, Lymphocytic
myocarditis, malignancy
– Macrophage Activation Syndrome: 10-20% risk mortality
French 2001
74
379/1/2021
75
“Luminous beings are we,
not this crude matter." -Yoda
76
389/1/2021
Summary
• JIA is a complex condition with many overlapping domains
• Can cause permanent damage to joints and eyes
• Treatments are drastically improving quality of lives, but flares
are common with stopping therapy
• Treat early and aggressively
77
Thanks!
78
39You can also read