Ventilation Non-Invasive (VNI) post opératoire, spécificités du Syndrome d'Apnée du Sommeil (SAS)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Ventilation Non-Invasive
(VNI) post opératoire,
spécificités du Syndrome
d’Apnée du Sommeil (SAS)
Samir JABER
Département d’Anesthésie-Réanimation
Hôpital Saint Eloi; CHU-MONTPELLIER
INSERM U1046 Université de Montpellier; France
ANESTH’REA SLEEP - Nîmes 8 Mars 2019
Liens d’intérêts en relation avec la communication (Loi Santé 2016-41)
Conflict of interest
*Consultants with honorarium
- Fisher-Paykel
- Dräger
- Xenios
- Medtronic
- Baxter
*Intensive Care Medicine Journal
- Deputy Editor
https://www.transparence.sante.gouv.fr
Post-operative N.I.V and S.A.S 1. Background 2. Rationale for use high-flow oxygen ; CPAP and NIV 3. In post-operative S.A.S patients 4. Bedside application : main optimal settings ?

Rational for use NIV in post-operative period:
Main modifications of respiratory function
↓ Cough
Residual ↓ Upper
effects of Pain
Fluid anesthesia-
airway
overload analgesia
HYPOXIA, Decrease of
Respiratory
Failure
lung volumes: Surgery
Pneumonia… î VC ; î FRC ; î VT
Diaphragmatic
Atelectasis dysfunction
Warner. Anesthesiology 2000
Jaber Anesthesiology 2011
Atélectasie et anesthésie en décubitus dorsal
Avant induction
Les atélectasies : ennemi public n° 1
Parties postéro-basales
(dependent parts of the lungs)
Après induction L. Magnusson. BJA 2003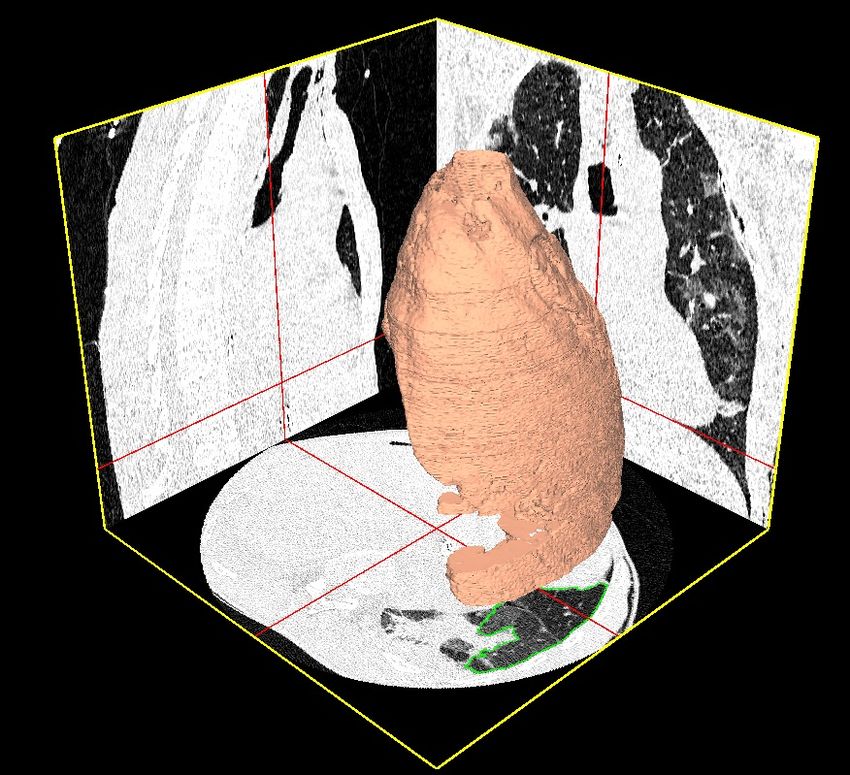
Mortality after surgery in Europe: a 7 day cohort study
Rupert M Pearse, Rui P Moreno, Peter Bauer, Paolo Pelosi, Philipp Metnitz, Claudia Spies, Benoit Vallet, Jean-Louis Vincent,
Andreas Hoeft,Andrew Rhodes, for the European Surgical Outcomes Study ( EuSOS) group for the Trials groups of the
European Society of Intensive Care Medicine and the European Society of Anaesthesiology* Lancet 2012; 380:1059-1065
Prospectively collected data from 46 539 patients undergoing inpatient surgery in 498 hospitals across 28
European nations
Overall crude mortality:
4%
Postoperative mortality was much
more higher than expected in non-
cardiac surgery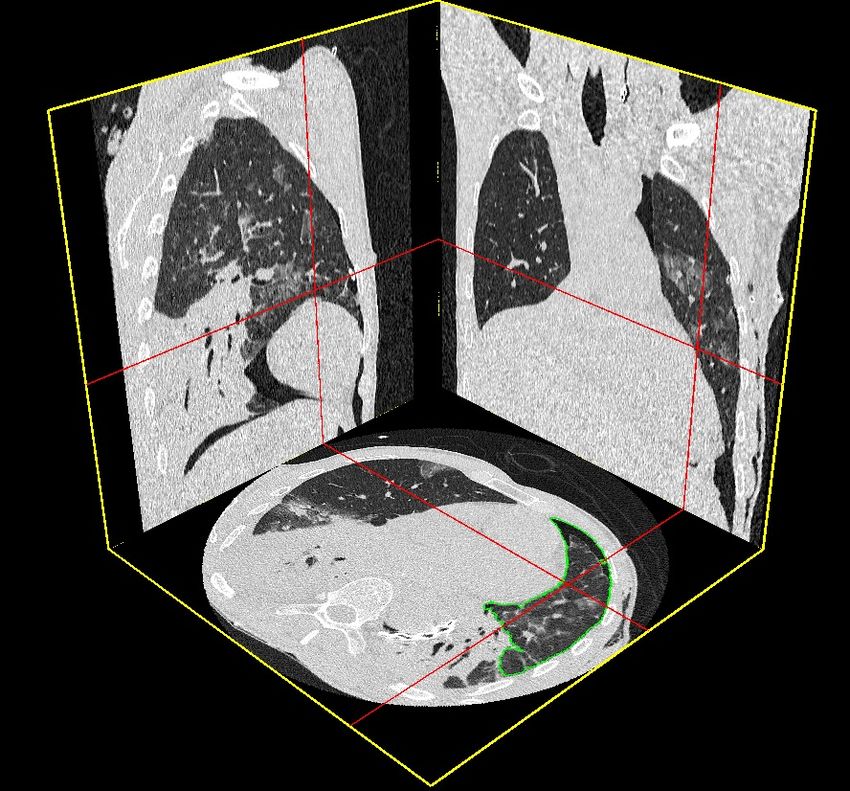
Risk and consequences of postoperative pulmonary complications
29,924 patients
Brueckmann et al. Anesthesiology 2013
Re-intubation for postoperative ARF increases risk for hospital death (×72)
Mortality ARF: 16% vs Non-ARF: 0,3%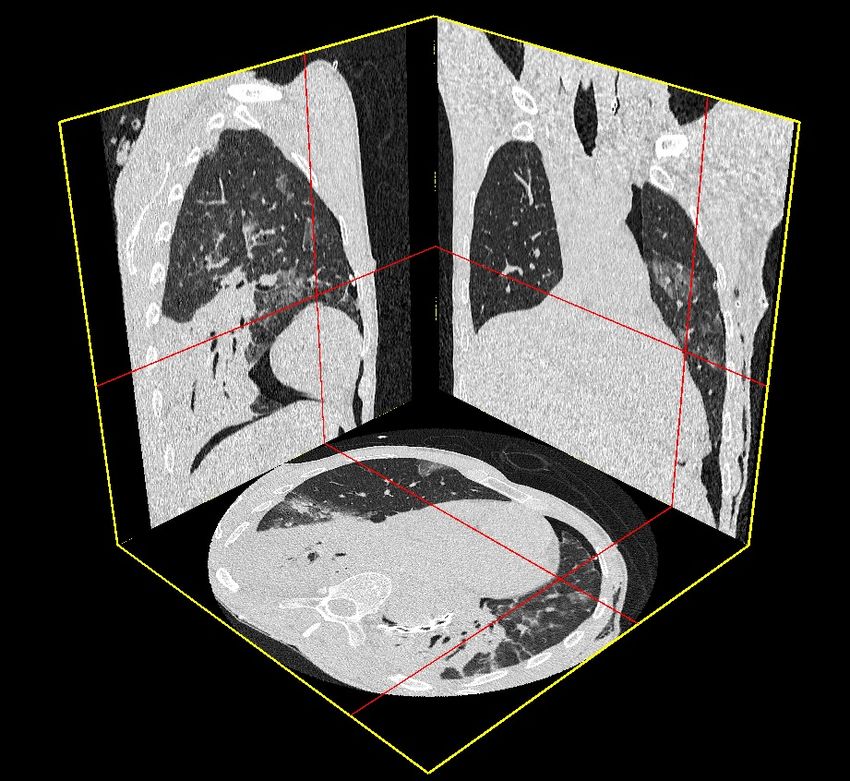
Perioperative Risk Factors of
Postoperative Pulmonary Complications (PPCs)
“Patient” risk “Surgical” risk “Anesthetic” risk
factors factors factors
Age > 70 Thoracoabdominal procedures General anesthesia
Obesity Upper abdominal incision Pain
Tabac Muscle disruption Fluid excess
Alcool use Muscle dysfunction Ventilatory strategy
Steroid use Emergency procedure
Denutrition Duration > 2-3 hours
Preoperative anemia Pneumoperitoneum
Respiratory disease Body positioning
COPD Transfusion > 4 units
SAS
Recent infection Others
Low preoperative SpO2
Others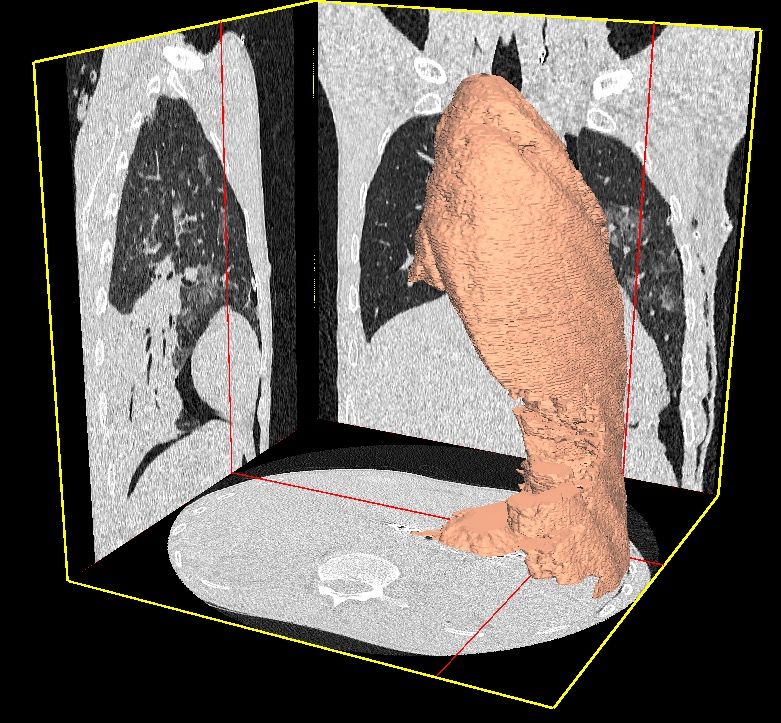
What are the main Ventilatory Support
after surgery and extubation to prevent reintubation ?
Paw
(PSV+PEEP) = +15
PSV = +7
PEEP= +8
PEEP= 0
Standard-
Oxygen
High-Flow
Oxygen
CPAP NIV
Spontaneous Spontaneous (=PEEP=8) (PSV+PEEP)
Breathing breathing
Flow
Ventilatory Support Management
after surgery to prevent reintubation
Curative Grey Prophylactic
zone (preventive)
ARF : yes (Present) ARF : no (not present…at risk!)
Objectif : to avoid intubation ! Objectif : to avoid the development of ARF
High Flow CPAP NIV High Flow CPAP NIV
Oxygen (1 pressure level) (2 pressure levels)
Oxygen (1 pressure level) (2 pressure levels)
(1 low pressure ) (1 low pressure )
Jaber et al. ICM 2014Post-operative N.I.V and S.A.S 1. Background 2. Rationale for use high-flow oxygen ; CPAP and NIV 3. In post-operative S.A.S patients 4. Bedside application : main optimal settings ?
Ventilation vs Oxygenation 1. Oxygenation Measured by : PaO2 ; SaO2 Determined by : FiO2 ; PEEP 2. Ventilation Measured by : PaCO2 ; EtCO2 Depends from minute ventilation VE = RR x VT (in reality VE= (Ti/Ttot) x (VT/Ti) every combination of RR x VT relates to same VE and PaCO2
ICM 2016
Rationale for use High-Flow Oxygen Therapy to prevent or treat acute
respiratory failure after surgery
Main effects of High-Flow Oxygen Therapy
1.Effect High FiO2
2.Effect Positive Pressure – PEEP (CPAP-like)
3.Effect : Humidification oxygen ++
4.Effect : comfort improvement
5.Effect : Dead space washout
6.Effect : Work of breathing (WOB) decreaseRespiratory Insufficiency Mechanisms ?
1. Gas exchanges 2. Ventilatory Pump
(Lungs) (Muscles - diaphragm)
Isolated Hypoxemia Hypoxemia + Hypercapnia
Oxygenotherapy Ventilation
(Improve PaO2 and SatO2) ( ↓ PaCO2 et ↑ pH)The major 5 Keys for NIV success
3.
2. Correct SETTINGS :
EXPERTISE - Limited insufflation pressure (no leaks)
- Limited Tidal Volume (VTeRationale for use NIV to prevent or treat acute
respiratory failure after surgery
Main effects of Non Invasive Ventilation (NIV)
1. Increased FiO2
2. Decrease Work Of Breathing (WOB)
3. Increased minute ventilation
4. Decreased dyspnea and comfort improvement
5. Alveolar recruitment : decreased atelectasis
6. Maintain patency of upper airway
7. Improve cardiac outputOxygenation Oxygenation
Ventilatory Support after extubation +
ventilation
Oxygenation (oxygen) Failure = Ventilation (Capnia) Failure =
Exchange (lung) failure Pump (muscles) failure
CPAP Intubation
(mask) +
Invasive ventilation
O2 canulae High Flow Oxygen NIV
(Low flow < 5 L/min)
(Bi-PAP)
O2 Invasive
Mask high
Concentration
Ventilation
(High flow > 10 L/min) (Intubation-tube)Post-operative N.I.V and S.A.S 1. Background 2. Rationale for use high-flow oxygen ; CPAP and NIV 3. In post-operative S.A.S patients 4. Bedside application : main optimal settings ?
Lancet Resp Med 2016
Lancet Resp Med 2016
®
The P.O.P Ventilation concept
A multifaceted bundle of Perioperative Positive Pressure
Futier E, Jaber S. Anesthesiology 2014The P.O.P® Ventilation concept
A multifaceted bundle of Perioperative Positive Pressure
IMPROVE Study NEJM 2013NEJM 2013
Postoperative Pulmonary
and Extra-pulmonary
Complications
0.50
0.40
Probability of event
28 % Non-protective ventilation 1. VT= 11 ml/kg/PBW
0.30
2. PEP= 0 cmH2O
3. No - Recruitment
0.20
1. VT= 7 ml/kg/PBW
11% Lung-protective ventilation 2. PEP= 7 cmH2O
3. Recruitment+ (RM)
0.10
Log$rank)test,)PAbdominal Surgery
NIV effects (30 min - PSV+15; PEEP+5) on pulmonary volumes
(recruitement - atelectasis) in a patient with ARDS at D3 peritonitis surgery
Before NIV After NIV
Jaber . Anesthesiology 2010Volumetric analysis of the CT-scans
- Three-dimensional reconstruction
and volumetry of CT data.
- Specifically designed software
according to methods previously
described (semi-automatic).
- Time acquisition of the whole
lung: 3 - 4 s.
Before NIV After NIV
Jaber . Anesthesiology 2010Volumetric analysis of the CT-scans
Before NIV After NIV
-900/ -1000
-1000 / -900 : Hyperinflated
-600/ -900
-500 / -100 : Poorly aerated
-200/-600
0/-200
-900 / -500 : Normally aerated -100 / +100: Non aeratedPostoperative NIV decreases work of breathing (WOB)
in the post-operative period
Spontaneous Ventilation (SV) NIV (PSV+10)
1.0
0.5 0.5
Flow
0.5
0
Flow
Flow
L/s
0.0
L/s
0.5 0.0
-0.5
-0.5
0
-1.0 0
0.0 5 0.0
Pes
10
10
-5.0
cmH2O
-5.0
cmH2O
Pes
Pes
-10 -10
-15 -15
25
20 10 10
15
5
cmH2O
cmH2O
5.0
Paw
10
Paw
Paw
5.0
0.0
0 0.0
-5.0
-10 -5.0
15
15
10 10 10
CMH2O
CMH2O
Pgas
Pgas
Pga 5.0 5 5.0
0.0
0 0.0
0.0 10 20 30 40 50 0.0 10 20 30 40 50
seconds seconds
0 10 20 30 40 50 0 10 20 30 40 50
ARF in a patient who developed ARF two days after hepatic surgery↑ airways obstruction / SAOS = CPAP ?
1. Lung
2. Upper
AirwayPost-operative N.I.V and S.A.S 1. Background 2. Rationale for use high-flow oxygen ; CPAP and NIV 3. In post-operative S.A.S patients 4. Bedside application : main optimal settings ?
The 5 main ventilatory settings in Non-Invasive Ventilation (NIV)
3. Pressure Support level
Pressure 2. Slope
(Paw) 5 < PSV < 15 cmH2O
Mild to max
4. Expiratory Trigger (cyclage I/E)
Cycling expiratory flow : 50%
Cycling time : 1,0 < Ti max < 1,2 s
Auto-track = automatic
5. PEEP
5 < PEEP < 10 cmH2O
Time
1. Inspiratory trigger
More sensitive without auto-triggering
(-1 to – 2l/min or -1 à -2 cmH2O)Case scenario
Quel(s) ventilateur(s)
Utiliser en VNI en réanimation ?
Prophylactic NIV after extubation in post-operative period in
Obstructive Sleep Apnea (O.S.A) obese patientJ1 post-extubation. Respirateur de domicile
(du patient, CPAP nocturne auto-set)
Patient coopérant
Respirateur de réanimation
(module VNI)
AI+PEP : journée en discontinueDurée des séances de VNI en post opératoire
Curative Prophylactique (preventive)
1. Initial (D1-D3 post-operative day)
Période de 60 à 90 min à Période de 30 min (15 à 45 min)
2 à 3 h d’intervalles à 4 à 6 h d’intervalles
(total 6-12h / jour) (total 1-4h / jour) (arrêt la nuit)
En cas de S.A.S :
1) Débuter le plus précocement possible la VNI en post-opératoire.
2) Faire des séances de durée plus prolongée la journée.
3) Appliquer la VNI (ou CPAP) toute la nuit/ Adapter réglages.
2. Suivi
Diminution progressive :
- Amélioration clinique
- Echanges gazeux
- Guérison de la pathologie initiale…Positioning at 30-45º promotes better
respiratoty function (avoid 0º or 90º)
Upright positioning of the patient is strongly recommended so that the
excess body tissue on the chest and against the diaphragm is displaced
caudad, which will reduce the WOB and increase the FRC.
- Burns et al. “Effect of body position
on spontaneous respiratory effort
and tidal volume in patients with
obesity, adominal distension and
ascites”. Am J Crit Care
1994;3:102-106
- Neill et al.”Effects of sleep posture
on upper airway stability in
patientswith obstructive sleep
apnea”. Am J Respir Crit Care
Med 1997;155:199-204S.A.S / Obese – position
Beach chair position
improves
Respiratory fonctionNIV in Upright position
2016
Acute Respiratory Failure (ARF)
within 7days of the surgical procedure
Curative NIV
1. Patients > 18 y
2. Laparoscopic or non-laparoscopic elective or non-elective abdominal surgery
3. ARF : - dyspnea (RR ≥30 c/min),
- clinical signs of respiratory muscle fatigue
4. hypoxemia : PaO2PRIMARY OUTCOME = Re-intubation at D-7
Cumulative Incidence of Intubation n=145
n=148
D-7
46 vs 33 %
Re-intubation
(p= 0.03)
P=0.027 by log-rank test
Figure = Kaplan–Meier Plots of the Cumulative Incidence of Intubation from Randomization to Day 30.MORTALITY
D-90
22 vs 15 %
Mortality (D90) (p= 0.148)
P=0.145 by log-rank testSECONDARY OUTCOMES
Standard
Oxygen Noninvasive P Value
Therapy Ventilation
Variable (N = 145) (N = 148)
Healthcare-infections to Day 30 – no. (%) 63 (49) 43 (31) 0.003
Lung 38 (30) 20 (15) 0.003
Urinary tract 13 (10) 8 (6) 0.193
Catheter 1 (1) 2 (2) 0.999
Bacteriemia 16 (13) 11 (8) 0.229
Surgical-site infection 20 (16) 18 (13) 0.564
Service utilization
Duration of invasive mechanical ventilation in 30 days 4±7 3±6 0.053
Invasive ventilation free days in the 30 days 23±11 25±9 0.039Cardio- Thoracic Surgery
High Flow Oxygen vs NIV after cardiothoracic surgery
• Multicenter, randomized,
noninferiority trial
• 830 pts after cardiothoracic surgery
• 1. Pts with post-extubation ARF
(curative strategy), or
Similar reintubation rate (13.7% vs
2. pts at risk for developing ARF
14%)
(preventive strategy)
• HFNT (50 L/min) or NIV (i8/e4)
• PRIMARY OUTCOME: treatment Post-hoc analysis
failure (ETI, switch, or stop) within 7
Curative
days
strategy: similar treatment failure rate (27% vs 28%)
Preventive strategy: lower treatment failure with High Flow Oxygen (6% vs 13%)TAKE HOME MESSAGES
- Post-operative ARF = always eliminate a surgical complication
- High Flow Oxygen and/or NIV should not delay "the time of reintubation"
No Clinical and gas
Clinical and gas
exchange
NIV exchange
improvement ? improvement
OK STOPDelayed intubation increases mortality
Carrillo A et al. Intensive Care Med 2012;38:458-466Late high flow oxygen failure intubation may cause harm
Ju Kang et al. Intensive Care Med 2015;41:623-32
175 pts with NHF failure: 130 early (≤48h), 45 late (>48h)
Early intubation associated with:
-↓ ICU mortality (39.2 vs 66.7%)
-↑ extubation success (37.7 vs 15.6%)
-↑ ventilator weaning (55.4 vs 28.9%)
-↑ ventilator-free days (8.6 vs 3.6)Take Home Message (1/2)
1. NIV (BIPAP) requires training and motivation of all the
medical teams (surgeons and others) and paramedical
teams (nurses,kine, physiotherapists…)
2. CPAP more easy to use and could be first-line therapy to
prevent and/or treat “hyopxemia”
3. High Flow Oxygen could be proposed
- As first-line therapy to prevent and/or treat “hyopxemia”
(except severe hypercapnia)
- As an alternative to CPAP/BIPAP in selected patientsTake Home Message (2/2) - S.A.S : early and prolonged (night+) post-operative NIV/CPAP - Post-operative ARF = always eliminate a surgical complication - High Flow Oxygen and/or NIV should not delay "the time of reintubation"
Merci
You can also read