Fertility Preservation: Has the Time Come? - Adam S. Howe, MD Pediatric Urology - 18th Annual Current Concepts in Men's ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Fertility Preservation:
Has the Time Come?
Friday August 9, 2019
Current Concepts in Men's Health, Saratoga, NY
Adam S. Howe, MD
Pediatric Urology
Albany Medical College
Albany, NY
Objectives 1. Assess the risk of infertility in patients undergoing iatrogenic gonadotoxic therapies 2. Understand the importance of onco-fertility and fertility preservation to patients and families undergoing cancer therapies 3. Explore different management options for fertility preservation (FP), including established, novel, and future therapies 4. Learn how to start up a fertility preservation program at your institution
Disclosures None

“No patient should be excluded for consideration
of discussion of fertility preservation for any
reason including age, prognosis, socioeconomic
status or parity”
American Society of Clinical Oncology, 2013

Iatrogenic Infertility
Cancer patients are surviving longer
Certain patients are at increased risk of infertility due
to side effects or complications of therapies treating
other conditions.
It is our duty as healthcare providers to discuss these
risks and offer management, if possible, to increase
the chance of fertility for these patients.
Conditions with increased risk of infertility
Oncology
Immunosuppression
– Hematologic
– Autoimmune / Rheumatologic / Nephrotic
– Transplant
Disorders of sex development and transgender
Trauma (eg, testicular/ovarian torsion)
Urological / Gynecologic
Estimation of Infertility Risk in Cancer
Challenging due to several factors:
the disease
stage
site
cumulative treatment dose (chemo + rad + sx)
age
gender
Chemotherapy that causes sub-fertility
in males (azoospermia)
- Chlorambucil* - Carmustine*
- Cyclophosphamide* - Lomustine*
- Procarbazine - Busulfan
- Melphan* - Ifosphamide*
- Cisplatin* - Nitrogen Mustard*
- Bleomycin
*Alkylating Agents!
Chemotherapy: Females (amenorrhea) High Risk: Intermediate Risk: Low Risk: - Busulfan* - Adriamycin - Actinomycin D - Chlorambucil* - Carboplatin* - Bleomycin - Cyclophosphamide* - Cisplatin* - 5-Fluorouracil - Ifosphamide* - Methotrexate - Melphalan* - Vincristine - Nitrogen mustard* - Procarbazine *Alkylating Agents!
Novel agents
Note:
Tyrosine kinase inhibitors, mTOR inhibitors,
and monoclonal antibodies have an unknown
risk to fertilityRadiation: Males - Testicular radiation > 1.2 Gy - Total body radiation > 12 Gy - Cranial radiation > 40 Gy
Radiation: Females
- Total body irradiation for bone marrow or stem cell txp
- Craniospinal radiation dose >25 Gy
- Pelvic or whole abdominal radiation dose:
– Pre-pubertal: >10-15 Gy
– Post-pubertal: >5-10 Gy
- Oocyte median lethal doseRisk of Sub-Fertility in Females
Acute Ovarian Failure
Occurs immediately following treatment
Associated with full abdominal or pelvic radiation or
hematopoietic stem cell transplant
Should counsel prior to starting therapy
Premature Ovarian Failure
Ovarian failure before 35 yo
Associated with alkylating agents
Should counsel survivors in late adolescencePatient Concerns
Discussions about fertility and preservation of this are of
great importance to patients
– Cancer survivors place great importance on having
children later in life and report psychological distress
related to fertility loss
Patients may make treatment decisions based on fertility
concerns
Parental influence in children and adolescentsFertility Preservation
All newly diagnosed cancer patients should be
informed of potential risk of compromised fertility
from the proposed treatment plan, along with being
informed of fertility preservation (FP) options
Fertility preservation procedures ideally should be
performed before the start of therapy
The decision to pursue FP is up to the patient and
family, declining to pursue FP is acceptable.Fertility Preservation Interventions
Options for Males Sperm banking Testicular biopsy for cryopreservation
Sperm banking
Suitable for boys Tanner stage 3 and above
60-86% success rates (pregnancy)
Referral to reproductive endocrinologist
Can be given a private room to produce a sample when
inpatient which will be immediately transported to storage
center
Can be collected via electro-ejaculation if requiredSperm banking
Botchan 2013
– Low usage rates (10%)
– Normal concentration but low motility
– Testicular cancer with worst semen qualities
– 66% conception rate
Kamischke 2004
– Low ejaculate volumes for ptsTesticular tissue for cryopreservation
Option for pre-pubertal boys and post-
pubertal boys who are unable to produce
a semen sample via ejaculation
Simple scrotal surgery under general
anesthesia with coordination of other
procedures
Contraindicated in patients with acute
leukemia not in remissionTesticular tissue for cryopreservation
Wu 2012
– Successful ICSI or natural mating in mice
Pietzak 2015
– 81% boys over 6mo had adult spermatogonia
– 44% over 6 yrs had primary spermatocytes
Sandri-Ardekani 2011
– Successful xenotransplantation from humans to miceHormonal therapy Gonadoprotection through hormone manipulation for FP has not been shown to improve recovery of spermatogenesis in men and is not recommended.
Options for Females Oocyte Preservation Ovarian Tissue Cryopreservation Ovarian Transposition
Oocyte preservation
Suitable only for post-pubertal females and considered established FP
method
60-87% live birth rates
Referral to reproductive endocrinologist
Ovarian stimulation (10-12 days, 4 different protocols)
GnRH antagonist-based protocols
May not be suitable for patients with conditions that preclude a delay
in starting therapy
Transvaginal ultrasound for retrieval of oocytesOocyte preservation
Wald 2019
– Oocytes yield doubled after back-to-back random-start
ovarian stimulation prior to chemo
– Mean time to complete 33 days
Relchman 2012
– Successful cryo of 18 mature oocytes in 13 year old
premenarchal female with myelodysplastic syndrome
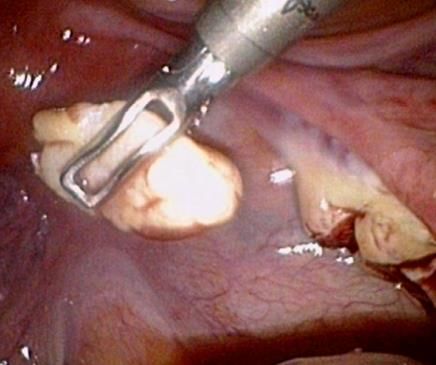
prior to chemoOvarian tissue for cryopreservation
For pre-pubertal girls and post-pubertal girls
who are unable to cryopreserve oocytes for
any reason
More than 60 cases of live births reported
Ovarian tissue biopsy or oophorectomy via
laparoscopic surgery under general anesthesia,
cryopreservation, and future reimplantation
(autotransplantation) or in vitro procedures
Future reimplantation contraindicated in
patients with leukemia
Vide
oOvarian tissue for cryopreservation
Donnez 2013
– 30% pregnancy and 20% live birth rate (natural and
IVF) after orthotopic reimplantation
Poirot 2019
– Better pregnancy and live birth rates (32% vs 0%) in
patients treated with chemo vs no chemo at 3 yrs
after orthotopic/heterotopic reimplantation
– Prior chemotherapy should no longer be a limitation to
ovarian tissue cryoOvarian transposition (oophoropexy)
Treatment strategy when pelvic
radiation is performed for cancer
treatment
Laparoscopic surgery under
general anesthesia placing the
ovaries outside of the pelvis
Preservation of ovarian function
in 90%Ovarian suppression therapy Gonadoprotection with GnRH analogs for FP in women show conflicting results and there is a lack of pediatric data. The ASCO does not support their use, therefore it is not recommended.
Conservative surgery
Strategy utilized to retain fertility by performing less radical
surgeries with the intent of sparing as much of the
reproductive organs as possible.
Examples:
Partial orchiectomy for mass in a solitary testis
Robotic trachelectomy for localized cervical cancerCosts of FP
1st year Annually thereafter
Sperm banking: ~$500 $400
Testicular tissue: ~$1,500 $400
Oocyte banking: ~$5,000 $400
Ovarian tissue: ~$2,000 $400
Oophoropexy: ~$1,000Costs
Currently, all costs are the responsibility of the patient/family
The LiveStrong fertility program is available for patients to apply online to
offset costs of coverage
www.livestrong.org/what-we-do/program/fertility
In 2017, Rhode Island and Connecticut became the first states to start
covering FP procedures for patients undergoing cancer treatmentLegislation
Recently, the Fertility Preservation Bill (formerly FAFTA
[Fair Access to Fertility Treatment Act), S719 and A2817,
has passed in New York state to add coverage for standard
fertility treatments for those facing iatrogenic infertilityAlbany Medical Center Fertility Preservation Program
Team members Urology Pediatric Hematology/Oncology Central NY Fertility (local site in Latham, NY)
Process
1. Hematology/Oncology initiates discussion of FP with patients before starting therapy
2. If patient desires and is a candidate for FP, referral to Urology for education with the
family and consent to FP intervention
3. Blood screen for transmittable disease markers (syphilis screen, Hep C virus serology,
Hep B antigen and antibody, HIV1/HIV2)
4. Referral to CNY (consent and arrangements for sperm banking, ovarian stimulation,
cryopreservation of samples)
5. Coordination of FP procedure with other surgeries (eg, mediport placement, bone
marrow biopsy)
6. Day of procedure: CNY brings transport media to AMC, urology notifies CNY when
biopsy or sample is finished and available for pickup
7. CNY sends report of biopsy to AMC (Urology & Heme/Onc)Potential
There are about 60 newly diagnosed pediatric
cancer patients that present to Albany Med per
year:
– 32 Male (20 prepubertal, 12 postpubertal)
– 28 Female (16 prepubertal, 12 postpubertal)Case
13 yo female with pelvic rhabdomyosarcoma and no
menses undergoing chemotherapy (vincristine,
dactinomycin, cyclophosphamide, and irinotecan)
Schedule to undergo pelvic radiation (total dose >50 Gy)
Underwent successful laparoscopic left ovarian
transposition and right ovarian cortex harvest for
cryopreservationBuilding a FP program at your institution
1. Strong connection between
oncologists and fertility specialists
Strong collaboration
Support and opinion of oncologist's “primary
care” can have significant impact on patient
decision making
Open communication crucial
– Especially with modification of treatment plans2. Building a FP team Reproductive endocrinologist Oncologist Anesthesia (experience with coordination) Pathologist (ovarian and testicular tissue) Lab personnel (experience with handling tissue banking) Genetic counselors Mental health professionals (help discuss ethical and legal issues) ***FP patient navigator (initial counseling and referrals)***
3. Design of FP consultation
Use of patient decision aids, brochures, and
websites
Follow-up visits (can be by phone or email too)
Additional contact with fertility specialistoncofertility.northwestern.edu
References
Ameri A, Novin K, Sourati A, Rshidi P. Awareness of female cancer patients about the risk of impaired
fertility. J Adolesc Young Adult Oncol, 2019 Jun;8(3):342-8.
Cakmak H and Rosen MP. Ovarian stimulation in cancer patients. Fertility and Sterility, 2013.
Cardozo ER, Huber WJ, Stuckey AR, Alvero RJ. Mandating Coverage for Fertility Preservation – A Step in
the Right Direction. NEJM, 2017.
Donnez J and Dolmans MM. Fertility Preservation in Women. NEJM, 2017.
Fallat ME and Hutter J. Preservation of Fertility in Pediatric and Adolescent Patients with Cancer.
Pediatrics, 2008.
Johnson EK, Finlayson C, Rowell EE, et al. Fertility Preservation for Pediatric Patients: Current State and
Future Possibilities. Pediatric Urology, 2017.
Loren AW, Mangu PB, Beck LN, et al. Fertility Preservation for Patients With Cancer: American Society of
Clinical Oncology Clinical Practice Guideline Update. Journal of Clinical Oncology, 2013.
Moawad NS, Santamaria E, Rhoton-Vlasak A, Lightsey JL. Laparoscopic Ovarian Transposition before
Pelvic Cancer Treatment: Ovarian Function and Fertility Preservtation. JMIG, 2017.Resources
www.allianceforfertilitypreservation.org
www.cms.gov
www.livestrong.org
www.nysenate.gov
Lisa Campo-Engelstein, PhD (Alden March Bioethics Institute at AMC)
SickKids Fertility Preservation Program (The Hospital for Sick Children, Toronto,
ON, Canada): Anne Marie Maloney, MSN, NP, CPHON (Pediatric
Hematology/Oncology) and Armando Lorenzo, MD, FRCSC (Pediatric Urology)
Southern California Reproductive Center (Los Angeles, CA, USA): Lina Akopians,
MD, PhD, FACOG (Reproductive Endocrinology)Thank You
You can also read