Fertility treatment options after vasectomy - BC Medical Journal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

March 2021: 63:2
Pages 49–96
Fertility treatment
options after vasectomy
IN THIS ISSUE
Evidence for extending the COVID-19
vaccine dosing schedule
Community physicians can remove erroneous
labels of childhood penicillin allergy
Benefits and limitations of ultrasound
in the diagnosis of rib fractures
Establishing a link between
antibiotics and asthma
in early life
In Plain Sight:
Elaboration on
the review
bcmj.org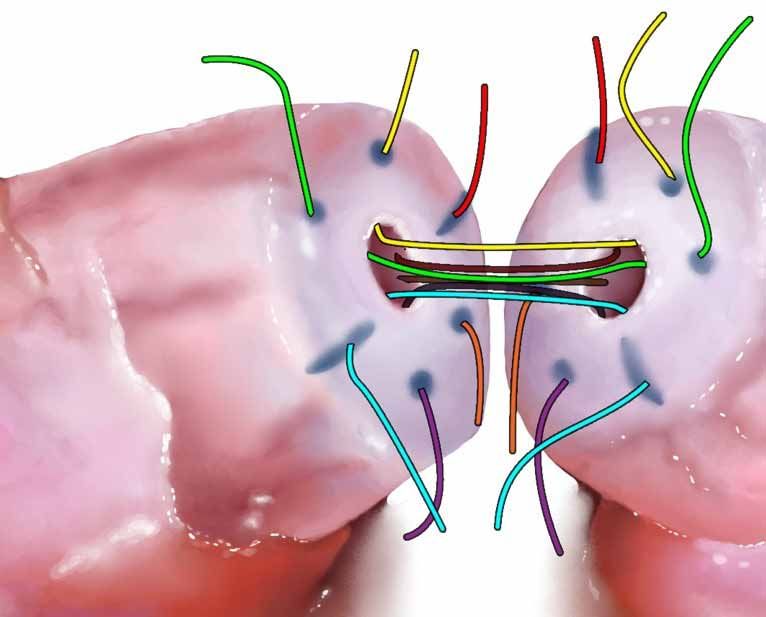
March 2021
Volume 63 | No. 2
Pages 49–96
There is increasing evidence that walking in nature can enhance immunity and improve chronic disease states. Read the Council on Health Promotion article on page 74.
The BCMJ is published by Doctors of BC. The journal
52 Editorials CLINICAL
provides peer-reviewed clinical and review articles Vaccines, David R. Richardson, MD
written primarily by BC physicians, for BC physicians,
along with debate on medicine and medical politics in
Searching for a silver lining 56 Empowering community
editorials, letters, and essays; BC medical news; career Cynthia Verchere, MD physicians to remove erroneous
and CME listings; physician profiles; and regular columns.
labels of childhood penicillin
Print: The BCMJ is distributed monthly, 54 President’s Comment allergy, Sean Duke, MSc, Tiffany
other than in January and August.
Great leadership during uncertain Wong, MD, Warda Toma, MDCM
Web: Each issue is available at www.bcmj.org.
times, Matthew C. Chow, MD
Subscribe to print: Email journal@doctorsofbc.ca.
Single issue: $8.00 62 Fertility treatment options after
Canada per year: $60.00 55 Letters to the Editor vasectomy, Luke Witherspoon, MD,
Foreign (surface mail): $75.00
n Re: Medical education during
Subscribe to notifications: Ryan Flannigan, MD
To receive the table of contents by email, visit COVID-19, Vielka Fernandez,
www.bcmj.org and click on “Free e-subscription.” Priscila Hernandez
67 What is the evidence for extending
Prospective authors: Consult the n Acknowledgment of referral
“Guidelines for Authors” at www.bcmj.org the SARS-CoV-2 (COVID-19)
Ben R. Wilkinson, MB
for submission requirements.
vaccine dosing schedule?
Tonia Tauh, MD, Michelle Mozel, MSc,
Paula Meyler, MD, Susan M. Lee, MD
On the cover Editor Managing editor Proofreader Printing
Fertility treatment David R. Richardson, MD Jay Draper Ruth Wilson Mitchell Press
options after vasectomy Editorial Board Associate editor Web and social media Advertising
Men who have had a Jeevyn Chahal, MD Joanne Jablkowski coordinator Tara Lyon
vasectomy have numerous David B. Chapman, MBChB Amy Haagsma 604 638-2815
Editorial and production
good options for achieving Brian Day, MB journal@doctorsofbc.ca
coordinator Cover concept and
a pregnancy with their Caitlin Dunne, MD
Tara Lyon art direction, Jerry Wong, ISSN: 0007-0556
female partner. Article David J. Esler, MD
Peaceful Warrior Arts Established 1959
Yvonne Sin, MD Copy editor
begins on page 62.
Cynthia Verchere, MD Tracey D. Hooper Design and production
Laura Redmond, Scout Creative
50 BC Medical Journal vol. 63 no. 2 | march 2021
71 News
n Book review: When Politics Comes
Before Patients: Why and How
Canadian Medicare is Failing
n COVID-19 recommendations from
the BCCDC and Ministry of Health
n MIND and Mediterranean diets
associated with delayed onset of
Parkinson disease
n New magazine from the JCCs
featuring stories of physician-led
innovations
73 WorkSafeBC
Occupational diseases and taking an
occupational history
Olivia Sampson, FRCPC
74 Council on Health Promotion
A walk in nature: The superfood of
physical activities
Ronald A. Remcik, MD
Although vasectomy is thought of as a permanent form of birth control, men who wish to attain fertility after having the
procedure may undergo a vasectomy reversal to achieve pregnancy with their partner. The highest reported success rate
75 Special Feature for vasovasostomy is the Goldstein microdot multilayer anastomosis, illustrated here. Article begins on page 62.
The benefits and limitations of
ultrasound in the diagnosis of
rib fractures from the emergency
department to the sports field: 83 Special Feature 91 Classifieds
A narrative review In Plain Sight: Elaboration on
Thomas S. Watson, MD the review, Mary Ellen-Turpel 94 Proust for Physicians
Lafond (Aki-kwe), JD, Laurel Dr Matthew Chow
79 Premise Lemchuk-Favel, MHA, Harmony
Establishing a link between Johnson (sɛƛakəs), MHA
antibiotics and asthma in early life
Hannah Lishman, PhD, Hind Sbihi, 89 Obituaries
PhD, Abdullah Al Mamun, MBBS, Dr Peter Coy
Drona Rasali, PhD, Emily Rempel,
PhD, Nick Smith, MPH, Stuart 90 CME Calendar
Turvey, MBBS, David M. Patrick,
MD
Environmental impact Postage paid at Vancouver, BC. Canadian Publications Mail, Product Sales Agreement #40841036. Return undeliverable copies
The BCMJ seeks to minimize its negative impact on the to BC Medical Journal, 115–1665 West Broadway, Vancouver, BC V6J 5A4; tel: 604 638-2815; email: journal@doctorsofbc.ca.
environment by:
Advertisements and enclosures carry no endorsement of Doctors of BC or BCMJ.
• Supporting members who wish to read online with an
e-subscription to bcmj.org © British Columbia Medical Journal, 2021. All rights reserved. No part of this journal may be reproduced, stored in a retrieval system, or trans-
• Avoiding bag use, and using certified-compostable plant-based mitted in any form or by any other means—electronic, mechanical, photocopying, recording, or otherwise—without prior permission in
bags when needed writing from the British Columbia Medical Journal. To seek permission to use BCMJ material in any form for any purpose, send an email to
• Working with Mitchell Press, ranked third in North America for journal@doctorsofbc.ca or call 604 638-2815.
sustainability by canopy.org Statements and opinions expressed in the BCMJ reflect the opinions of the authors and not necessarily those of Doctors of BC or the
• Printing with vegetable-based inks institutions they may be associated with. Doctors of BC does not assume responsibility or liability for damages arising from errors or omis-
• Using FSC-certified paper sions, or from the use of information or advice contained in the BCMJ.
• Printing locally in British Columbia The BCMJ reserves the right to refuse advertising.
BC Medical Journal vol. 63 no. 2 | March 2021 51
Editorials
Vaccines
25 January 2021
I
received my first dose of vaccine against with my new microchip. I am so glad they don’t on this scale is a challenge none of us has pre-
COVID-19 last week. A fellow physi- have to monitor my cellphone anymore. viously faced.
cian from another location injected me at I was given the Pfizer vaccine, as were three It is crucial that the vaccination process
a hospital vaccination clinic. For some reason of my office colleagues. My other three col- proceeds in an organized and speedy fashion
he avoided the bulk of my deltoid and aimed leagues received the Moderna vaccine, so we if we are going to control this virus and allow
for the acromion, causing him to hit bone. I are now divided into teams and are carefully life to return closer to normal. The longer the
do not think he gives many vaccines where watching each other. They must not have acti- virus reigns free, the greater the chance there
he normally works. One of my younger office vated the chips yet because I still must speak is for it to mutate and form a strain that is re-
colleagues pointed out that sometimes it is dif- out loud to converse with my fellow Pfizers. sistant to the current vaccines. Not only must
ficult to find the atrophied deltoid muscle of In truth, I feel privileged to be in the first the developed world be vaccinated, but efforts
the withered elderly. wave vaccinated against this horrible virus. I must be made to vaccinate poorer countries,
It burned going in, which I attribute to it stand in awe of the science behind these vac- both for humanitarian reasons and to ensure
not being room temperature. The next day I cines and the collective effort that led to their a large reservoir of potentially mutating virus
wondered if the vaccine had made me achy, speedy development. It is a testament to what does not exist.
but then I remembered that I am always achy. can be accomplished when humankind works There will likely be more bumps in the road
Apart from feeling like I had been punched in together. as this mass vaccination program gathers speed.
the arm for a few days, all is well. I hope this spirit of collaboration continues However, if we meet these adversities with pa-
I can already feel my DNA being altered and throughout this vaccine rollout process. It will tience and ingenuity, it is only a matter of time
am hoping for either the superpower of being be March before this editorial is published, before this pandemic will be behind us.
able to fly or become invisible at will (which and I remain optimistic that by the publication Above all, remember to be kind, because I
would you choose?). As an aside, when I ask pa- date a mass vaccination program will have been will receive my second dose in a few weeks and
tients this question, almost every child wants to outlined. There have been some missteps so could be watching. n
be able to fly, while most adults want invisibility far, such as wasted doses, supply issues, queue —David R. Richardson, MD
so they can go where they should not. Regard- jumping, and lack of transparency. However,
less, I am doing well and am making friends getting millions of doses into millions of arms
Available for streaming on
all podcast platforms
BURNOUT AND COVID-19
Warning signs
and when to act
with guests
Dr Jennifer Russel
and Dr Lawrence Yang
A Doctors of BC Podcast
52 BC Medical Journal vol. 63 no. 2 | march 2021
Editorials
Searching for the silver lining
W
e’ve missed so much this year. Many of us have taken time to be alone with and security of closeness and touch. At work
The directly tragic stories are of ourselves. We made walking in the street a des- there was perhaps some privilege in being a
families missing loved ones lost tination. Some learned to make bread or knit or woman of my generation to be able to socially
to or harmed by the virus, or those suffering write music or teach math. Partners have had touch patients. A hand on a shoulder, a shoulder
from isolation: poverty, loneliness, addiction, the opportunity to appreciate each other’s lives for tears, the nest of our arms holding a baby.
and mental illness. Overlying everything is the more fully. When we were publicly reminded From seconds after we are born, we strive for
“lessness” of our ability to give our patients and to be kind, we didn’t roll our eyes. We saw how skin-on-skin touch, and I see now that it never
loved ones full attention and care. others were affected and learned how to reach really left me. Touch feels warm, protective, and
I cannot emphasize enough how much re- out even when we were locked in. We were col- bonding. It can express grief, compassion, and
spect and gratefulness I have for my colleagues lectively moved by and shared things happening care where words fail. People let into a circle of
who face risk directly, looking after very sick pa- all over the world that we might have previously compassionate touch know that they are loved
tients. We who remain healthy and privileged to found mawkish—apartment-window-singing and cared for. The tacit exchange of vulner-
have safety nets in our lives and jobs have lived in Italy, pot-banging and applause marking abilities and comfort is otherwise difficult to
what should be a perspective-changing year. 7 p.m. everywhere. We realized that we were express, outside of poetry.
First, we must acknowledge that living in part of something affecting all of humanity, all Heartbreakingly, this year has made me
this province, with the particular leadership with equal jeopardy. As independent humans touch-averse. I automatically widely avoid peo-
decisions that have been made, and the luck we were forced to accept being reduced by an ple on sidewalks and in hallways, move away in
associated with the timing of spring break, has invisible force to the vagaries of biology that conversations, and even feel reflexively assaulted
left us in a better position than most. When we we all share. if someone comes too close or touches me. I
have needed our neighbors to do their part for Silver linings are personal touch points dur- wince during movies filmed pre-COVID-19
one another, we and our communities have, for ing a time of anxiety, for most of us. It’s in- at what now stands out as absolutely reckless
the most part, politely complied. And when we teresting to hear what people dream of doing casualness in contact and unprotected faces.
haven’t, the consequences have been frighten- when the pandemic is so-called over—eating My brain feels completely rewired: I’m in some
ing but, touch wood, not so catastrophic that inside a restaurant, enjoying a concert, taking a ways foreign to my basic nature.
we couldn’t continue our steady course through cruise, traveling in general, enjoying the breeze The moment we can once again experience
them. Watching the devastation across a politi- on an uncovered face. All of those sound won- the joy of social touch will be the time that I
cal border, our fortune is clearly spotlighted. derful, but for me, it’s experiencing the joy of define as things being back to right. It cannot
That spotlight also illuminates glimmers of touch again. come soon enough. n
silver linings. I am, to the base of my soul, a hugger. I —Cynthia Verchere, MD
We have been able to spend more time hadn’t realized how much I rely on the warmth
with our families in our homes, and to be cre-
ative with our time and energy in new ways.
By allowing ourselves to simply do the best
we could in the situation, we became open to
accepting things that were, maybe, not tradi-
tionally acceptable. It’s now clear that support-
ed, unfettered research can lead to successful
results—novel vaccines have been developed
with unprecedented speed and effectiveness.
Having technology that offers us inexpensive
face-to-face access to other people allows us to
feel closer to those we can’t be close to. Fewer
patients have had to travel the highways for
their follow-ups, and almost all of them are
grateful for the reduced risk and cost. These
silver linings will be long-term.
BC Medical Journal vol. 63 no. 2 | March 2021 53
president’s comment
Great leadership during
uncertain times
22 January 2021
I
t has now been a year since the COVID-19 the issues that were important to me. I needed The COVID-19 restrictions have limited the
pandemic reached our shores. During only 15 to 20 minutes per day to scan through opportunities for face-to-face interaction that
these uncertain times, we have seen first- the viewpoints of credible people, then I could is so critical for thoughtful debate and effective
hand how skillful leadership is more important get on with my life. I did have a good chuckle leadership. The restrictions have made it difficult
than ever. And while there have been volumes at some of the flame wars between people with for leaders to listen, to avoid distraction, and to
written on what constitutes great leadership, the contrary views, but it was liberating to not be demonstrate genuine care when they are limited
following three traits seem to be common to involved. My little experiment also revealed how to news releases, emailed communications, and
some of our most capable, effective, and trust- much social media warps people and complex brief townhalls. And they have made it difficult
worthy leaders. issues into oversimplified caricatures—great for for those who follow to stay engaged and con-
Great leaders are great listeners. Listening eliciting a highly charged emotional response nected. But we can overcome this by having
seems to be a lost art at a time when everyone but not conducive to effective debate. I often more leaders who are closer to the people they
is blasting away with 280 characters or less. wonder how much more progress people would serve and who can demonstrate these important
Listening takes time, focus, and intention. It make if they sent each other a discrete direct traits. I have seen this in doctors stepping up in
means stopping to make sure what has been said message or fired up a video chat rather than their communities to listen to their neighbors,
has been heard and understood. Unfortunately, exchanging volleys over Twitter. filter through all the conflicting medical infor-
listening is one of the first casualties in a crisis, Great leaders also show that they care about mation, and show they care. Some of the most
yet it is critical to successful leadership. There the people they lead. There are many ways to do effective leaders I have seen have no formal title,
are some obvious advantages to listening, such this, as we have seen during the pandemic. Some they simply saw a gap and filled it.
as gaining important perspectives and becom- leaders show their care through expressions of When I think about the challenges this next
ing aware of emerging risks, but I think there raw emotion, which break through their calm stretch of the pandemic will bring, I’m aware
is another reason why listening is so important. exterior—a little anger, a few tears, a departure that now more than ever we need more people
People do not want to follow people who don’t from their speaking notes. Others demonstrate to step up as leaders. We need to overcome a
listen. It’s a fundamental human need to be care through service, such as pinch hitting when continuous onslaught of noise and outright
heard. Great leaders know this. They take lis- staffing is short or volunteering for an undesir- misinformation. We need to convince more
tening as seriously as any other skill, meaning able task. And then there are those who express people to follow public health directions, even
they put in the time to become better listen- their care by how they address people, respond- as high-risk and vulnerable people become
ers, they practise constantly, and they measure ing with respect when it would be easier to be protected by vaccination. We need to combat
their progress. dismissive, meeting anger with compassion, prejudice and tribalism that still rears its head
While being great listeners, great leaders treating others as they would want to be treated. despite our vigilance. And, we need to take
also know how to tune out noise. During a All this presumes that a leader cares about the care of each other by listening to one another,
crisis, everything is urgent, and everything and people they are leading. Even children can tell by freeing ourselves from the distractions that
everyone demands immediate attention, but as the difference between someone who genuinely take us away from what’s important, and by
the saying goes, “when everything is a prior- cares for them and someone who merely says showing that we care. n
ity, nothing is.” Noise seems to be particularly they do. Great leaders genuinely care and they —Matthew C. Chow, MD
prevalent these days on social media. I was take pains to show it. Doctors of BC President
challenged to do an experiment where I sig- Anyone can learn and practise great listen-
nificantly curtailed my consumption of social ing skills, tune out the noise, demonstrate care
media for 2 weeks. Not only did I gain back for others, and become a great leader. Granted,
time for self-care, I was no less informed about it’s more challenging to accomplish these days.
54 BC Medical Journal vol. 63 no. 2 | march 2021
referral has been received. How long should a
Letters to the editor We welcome
original letters of less than 300 words; we may edit them for clarity
patient who hears nothing wait to discover that
the referral got lost?
I believe that all specialists’ offices should
and length. Letters may be emailed to journal@doctorsofbc.ca, submitted contact the patient as soon as they receive a
online at bcmj.org/submit-letter, or sent through the post and must include referral. The patient should be informed of the
your mailing address, telephone number, and email address. Please disclose office policy. They may be told that they should
any competing interests. expect a call in N weeks, when they will be given
an appointment, if this is how the office works.
—Ben R. Wilkinson, MB, FRCSC
Re: Medical education during topics, and educators can provide feedback on Yellow Point
COVID-19 their academic performance.4 As faculty mem-
bers must remain up-to-date on the use of vir- The BC College of Physicians and Surgeons has
The COVID-19 pandemic is a global health
tual interfaces, quarterly training sessions can published a guideline addressing the above concern
threat that has challenged medical schools
familiarize them to minimize anxiety due to in detail (www.cpsbc.ca/files/pdf/PSG-Referral
across the world to rapidly transition from con-
technological complexities.5 -Consultation-Process.pdf ). Briefly stated, the Col-
ventional classroom training to virtual learn-
In light of these challenging circumstances lege recommends that consulting physicians ac-
ing environments. As proposed by Dr Wong
in virtual learning, medical education must take knowledge receipt of referrals as soon as possible,
in his article (BCMJ 2020;62:170-171), the
advantage of innovative technologies to improve at the same time indicating if the referral is being
strategies posed to secure medical training dur-
student competitiveness and prepare them for accepted or rejected. The College also expects that the
ing this pandemic should be principle-based,
emerging health threats. consultant will promptly advise both the patient
forward-looking, and compassionate.1
As medical students in the Dominican Re- —Vielka Fernandez and referring physician of the date and time of the
public, we have witnessed firsthand the effects —Priscila Hernandez appointment. —Ed
Santo Domingo, Dominican Republic
of this pandemic in our professional formation.
New obstacles—such as limited access to reli-
References
able Internet connections, faculty members and
1. Wong RY. Medical education during COVID-19: Lessons
students without experience in virtual learning, from a pandemic. BCMJ 2020;62:170-171.
and feelings of anxiety due to isolation and the 2. Teachers Press Releases, Instituto Tecnológico de San-
unknown future—can affect the quality and to Domingo (INTEC). Claro and INTEC sign collabora-
tion agreement. Accessed 17 November 2020. www British Columbia
delivery of medical education. Medical Journal
.intec.edu.do/en/notas-de-prensa-profesorados/item/ @BCMedicalJournal
In low- and middle-income nations, avail- claro-e-intec-firman-acuerdo-de-colaboracion.
able resources can be scarce, and medical schools 3. Centers for Disease Control and Prevention. One Health British Columbia Medical Journal
should be creative when addressing the chal- basics. 2018. Accessed 18 November 2020. www.cdc
@BCMedicalJournal
lenges experienced by faculty members and .gov/onehealth/basics/index.html.
4. Merchant A, Chastain II P. Role of case reports in mod- BCMJ Blog: Five quick facts about COVID-19 and
students. To ensure access to reliable Internet ern medical education. Clin Case Rep Rev 2018;4:1-2. fertility
connections, some programs in the Dominican 5. AlRomi N. Human factors in the design of medical The Society of Obstetricians and Gynaecologists of
Republic have developed formal agreements simulation tools. Proc Man 2015;3:288-292. Canada released a statement that supports offering the
with telecommunication companies.2 Although vaccine to pregnant and breastfeeding women.
the long-term impact of these agreements is Read the post: bcmj.org/blog/five-quick-facts-about
unknown, they will surely offer valuable learn- Acknowledgment of referral -covid-19-and-fertility
ing opportunities to students from urban and As an old, retired specialist, I am driven nuts
rural areas alike, while also providing faculty by a certain policy among some specialists! I
members with the tools to strengthen teachers’ am referring to the policy of making no contact
skills. By fostering intersectoral cooperation with a patient who has been referred until an
between medical schools and telecommunica- appointment can be arranged. As I understand
tion companies, the One Health concept3 can this policy, each referral is filed, and when an
be applied in a practical setting. appointment time becomes clear, the patient is
Additionally, when virtual simulations are contacted. This policy assumes that the refer-
integrated into didactic coursework, medical ral process is infallible. It has been known for
students can enhance their problem-solving and referrals to get lost in cyberspace. This means
Follow us on Facebook for regular updates
decision-making abilities on essential clinical that the patient receives no recognition that a
BC Medical Journal vol. 63 no. 2 | March 2021 55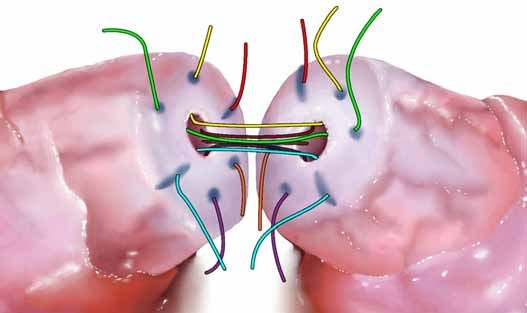
Clinical
Sean Duke, MSc, Tiffany Wong, MD, FRCPC, Warda Toma, MDCM, FRCPC, MPH
Empowering community
physicians to remove
erroneous labels of childhood
penicillin allergy
With adequate training and use of clinical guidelines, nonallergist
health care providers can help reduce the consequences of unverified
beta-lactam allergy and improve the capacity for allergy evaluation by
safely implementing direct oral provocation testing in children at low
risk of true allergy.
ABSTRACT: Childhood beta-lactam allergy is fre- allergy in a large proportion of children in favor of physician, remains the most frequent indica-
quently reported, but most of the children in these direct oral challenges that forgo traditional ante- tion for beta-lactam prescribing in children.5
cases can safely tolerate the antibiotics without cedent skin tests. A Canadian Paediatric Society Beta-lactam allergy is commonly misdiagnosed
adverse reaction. This discrepancy may be due statement from January 2020 recommends using in children, as over 90% of children with this
to the attribution of viral exanthems and drug- a clinical algorithm to administer a test dose of label are able to tolerate the antibiotics upon
virus interactions to beta-lactam hypersensitivity amoxicillin to children deemed to be at low risk of evaluation.6-8 Unverified beta-lactam allergy
without reliable evaluation. Erroneous beta-lactam true allergy, such that family physicians and gen- presents a major set of challenges related to
allergy labels confer substantial public health con- eral pediatricians may safely and reliably evaluate patient safety, antimicrobial resistance, and
sequences, including longer hospital admissions, unverified beta-lactam allergy—as long as they health care costs. We discuss the consequences
higher rates of antimicrobial resistance, and higher are equipped to carefully select patients, interpret of unverified beta-lactam allergy, highlight the
health care costs. These preventable outcomes, clinical findings, and manage adverse reactions, importance of beta-lactam allergy de-labeling,
stemming from the unnecessary withholding of including anaphylaxis. The involvement of non- and make suggestions for confronting this issue.
first-line antimicrobial therapy for several common allergist physicians can dramatically expand the
infections, have prompted several large-scale initia- capacity for evaluating childhood beta-lactam Erroneous beta-lactam allergy labels
tives that promote the widespread evaluation of allergy, a responsibility that has been shouldered in childhood
beta-lactam allergy. Recent studies have generated exclusively by pediatric allergists, and subsequently Drug allergy, a reproducible, immune-mediated
a shift in the routine evaluation of beta-lactam permit the use of first-line antimicrobial therapy response to a pharmaceutical in a sensitized
in a large group of patients. person,9 represents a minority of adverse drug
reactions to beta-lactams.10 Adverse drug reac-
B
Mr Duke is a medical student at the eta-lactams, particularly penicillins and tions to beta-lactams are common in children,
University of British Columbia. Dr their derivatives, are among the most with maculopapular exanthems occurring in
Wong is a clinical assistant professor in commonly prescribed medications for 5% to 10% of children prescribed amoxicillin
the Faculty of Medicine, Department children globally,1,2 with common indications or ampicillin.9
of Pediatrics, Division of Allergy & for the ambulatory, inpatient, and periopera- Pediatric beta-lactam allergy labels are fre-
Immunology, University of British tive settings. They are the antibiotics of choice quently acquired due to rashes that are reported
Columbia. Dr Toma is a clinical instructor for the treatment of many infectious illnesses by parents.10 Viruses are the most common
in the Faculty of Medicine, Department of due to their low toxicity, targeted spectra of cause of childhood maculopapular or urticarial
Pediatrics, University of British Columbia. activity, excellent distribution throughout the eruptions [Figure 1].2 A Swiss study involv-
body, and low cost.3,4 Acute otitis media, the ing 88 children with nonimmediate cutaneous
This article has been peer reviewed. most common cause of childhood visits to a eruptions after beta-lactam exposure revealed,
56 BC Medical Journal vol. 63 no. 2 | march 2021
Duke S, Wong T, Toma W Clinical
after a complete evaluation, that only 7% were
allergic to the antibiotics.2 A drug-viral inter-
action can result in a cutaneous reaction that
is misattributed to drug allergy,10 an example
being aminopenicillin-induced exanthema in
children with Epstein-Barr virus infection.2
Other signs and symptoms of illness, such as
cough and tachypnea, or coincidental events
unrelated to illness, such as headache, can also
be mislabeled as an allergic reaction.11 Predict-
able side effects of beta-lactams, such as gastro-
intestinal upset, may be misattributed to drug
allergy [Table 1].11
Despite the unverified status of most
beta-lactam allergy labels, this diagnosis often
persists into adulthood because many clini-
cians—fearing a severe allergic reaction—elect
to use alternative antibiotics, often without re-
ferral for evaluation.2 Individuals frequently
outgrow true penicillin allergy through the loss
of IgE-mediated sensitivity over time,12, 13 which
highlights the importance of reassessment.
Consequences of erroneous
beta‑lactam allergy labeling Figure 1. Viral exanthem in a child. Source: DermNet NZ (Creative Commons Licence: https://creativecommons
Mislabeling of beta-lactam allergy is associated .org/licenses/by-nc-nd/3.0/nz/legalcode).40
with significant public health concerns, includ-
ing health consequences to patients, antimicro- Table 1. Classification of drug allergy as it pertains to beta-lactams.
bial resistance, and higher health costs.3,9,14,15
Gell-Coombs Timing of
Direct consequences to patients include the classification onset
Clinical presentation Comments
needless reliance on second-line, more toxic,
Type I Immediate: Urticaria, angioedema, Penicillin is the most common cause
broader spectrum antibiotics such as fluoro (IgE-mediated) < 1 hour respiratory distress, of medication-induced anaphylaxis;30
quinolones, clindamycin, and vancomycin;14 hypotension, anaphylaxis however, the incidence of anaphylaxis
higher rates of multiple and parenteral antimi- to beta-lactams is reported to be < 1%.35
crobial therapy;14 and increased hospitalization.14 Type II Nonimmediate: Anemia,
A cohort study involving 51 582 participants (cytotoxic) 10 hours to thrombocytopenia
weeks
revealed that patients with unverified penicillin
allergy had nearly 10% longer stays in hospital Type III Nonimmediate: Serum sickness, tissue Beta-lactam antibiotics, particularly
and were 14.1% to 30.1% more likely to suffer (immune- 1–3 weeks injury cefaclor, have been implicated in serum
complex sickness-like reactions,36 which present
from Clostridium difficile, methicillin-resistant mediated) with fever, rash, and urticaria; however,
Staphylococcus aureus, and vancomycin-resistant unlike serum sickness, they do not
Enterococcus infections versus matched con- involve immune complexes, vasculitis,
or renal lesions.37
trols.14 Alternative antibiotics tend to be more
costly than penicillin derivatives3,16 and place Type IV Nonimmediate: Mild cutaneous: Nonimmediate reactions are the most
(cell- 2–14 days Maculopapular exanthema common reactions to beta-lactams
patients at risk of adverse events.17 mediated) Severe/systemic: Stevens- in children. They occur in 5%–10%
More widespread and routine evaluation Johnson syndrome, toxic of patients taking beta-lactams,9
of unverified beta-lactam allergy has become epidermal necrolysis, drug and typically present as mild, self-
rash with eosinophilia limited maculopapular or urticarial
a major public health goal and is recognized as
and systemic symptoms exanthemas;31 however, most of these
an essential component of antimicrobial stew- (DRESS) syndrome, reactions are attributed to an infectious
ardship,18 which is reflected in recent Canadian acute generalized cause, while the remainder are thought
Paediatric Society statements,19,20 in American exanthematous pustulosis to be cell-mediated.9
BC Medical Journal vol. 63 no. 2 | March 2021 57
Clinical Empowering community physicians to remove erroneous labels of childhood penicillin allergy
and Canadian Choosing Wisely initiatives,21,22 and colleagues demonstrated the limited sen- challenge14,20 because it contains the immuno-
and most notably in the Obama administra- sitivity of specific IgE (0%), intradermal testing logically relevant penicillin core structure.14
tion’s National Action Plan for Combating (67%), and patch testing (0%) in 88 children Individuals with histories consistent with ana-
Antibiotic-Resistance Bacteria.23 with histories of mild cutaneous reactions to phylaxis or severe delayed reactions are consid-
Economic projections have produced com- beta-lactams.2 International guidelines recom- ered to be at high risk of true allergy and are not
pelling data on the increased costs associated mend skin testing as first-line investigations for suitable candidates for direct oral provocation
with erroneous beta-lactam allergy. In reviewing penicillin allergy9,13 by virtue of its low risk11 and testing.9,20 Given the limited role of adjunctive
inpatient charts, an antimicrobial stewardship negative predictive value of nearly 100% with testing in pediatrics, direct oral provocation
program at a US tertiary hospital estimated standardized reagents in adults;30 however, re- testing appears to be more reliable20,27 in evalu-
an annual savings of US$82 000 from the cent studies suggest a substantial false-negative ating nonserious pediatric beta-lactam allergy
de-labeling of unverified penicillin allergy in than conventional clinical pathways, with recent
just 145 patients, accounted for by obviating evidence demonstrating a specificity of 100.0%,
several unnecessary measures, including intra- Beta-lactam allergy negative predictive value of 89.1%, and positive
venous therapy where oral beta-lactams were is commonly predictive value of 100.0%.7
deemed superior, PICC line insertion/removal, misdiagnosed in In recent studies, the safety of direct oral
routine drug-level testing, laboratory costs, and provocation testing for beta-lactams has been
children, as over
pharmaceutical drug calibration costs.15 Further, demonstrated in children identified as low risk
a case-control study of 118 randomly selected 90% of children with of true allergy.6,7,25,27-29 A Montreal prospective
inpatients with unverified penicillin allergy, and this label are able to study involving 818 children with suspected
the same number of matched controls, revealed tolerate the antibiotics amoxicillin-induced rash with low-risk fea-
a 63% greater mean cost of treatment in the tures employed a direct, graded two-step direct
upon evaluation.
penicillin-allergic group.3 amoxicillin challenge, which revealed tolerance
in 94% of participants.7 Of the remaining 6%
Evaluation of beta-lactam allergy in of participants, 17 children experienced mild
children rate in the pediatric population. A Canadian immediate reactions (urticaria), while 31 chil-
The conventional evaluation of penicillin al- study revealed that 94% of children with ob- dren developed mild nonimmediate reactions.7
lergy incorporates clinical history with con- served immediate reactions to an oral amoxicillin A Winnipeg chart review of 306 predominantly
firmatory testing, including skin testing and challenge had negative intradermal testing.7 The pediatric patients with suspected beta-lactam
oral provocation challenge in skin test-negative positive predictive value of skin testing in the allergy demonstrated tolerance to the culprit
individuals.12 Traditionally, diagnostic pathways evaluation of pediatric beta-lactam allergy is beta-lactam in 96% of patients via direct oral
for children have been extrapolated from adult reported as 36%,2 indicating a tendency to “over- challenge in low-risk patients or by oral chal-
guidelines, under the assumption that general call” beta-lactam allergy when a positive skin test lenge following negative intradermal testing
principles are applicable across age groups.24 is deemed sufficient for diagnosis. Aside from in those patients with vague histories or those
However, growing evidence over the past de- bearing diagnostic ambiguity, skin testing is suggestive of an IgE-mediated reaction.6 Of
cade has influenced a shift in routine practice, time- and resource-consuming, causes discom- those patients who had positive oral testing, one
which supports the use of direct—that is, with- fort, and is exclusively performed by allergists, experienced a possible Type I reaction (acute
out antecedent skin testing—oral challenges who have limited capacity for the increasing onset abdominal pain and emesis), while the
to beta-lactams in children with mild index demand for beta-lactam allergy evaluation. remainder experienced nonimmediate macu-
reactions to the antibiotics.2,6,7,25-29 lopapular exanthema. A prospective study that
Oral provocation testing used a graded five-step method of direct oral
Skin testing Oral provocation testing, the accepted gold testing with the culprit beta-lactam in 119 chil-
Despite longstanding use of tests adjunctive standard for evaluation of suspected beta-lactam dren with a history of nonimmediate mild cuta-
to oral challenges in the evaluation of adult allergy,1,7, 20 is relied upon for the confirmation neous reactions, followed by a 5-day, twice-daily
penicillin allergy, the diagnostic utility of such or exclusion of allergy in carefully selected in- extended course demonstrated tolerance in 97%
tests is not well established in the pediatric dividuals.7 However, there is no international of children, and only mild cutaneous symptoms
population.2,27 A recent systematic review re- consensus on how direct oral challenges are in the remaining children.25
vealed a lack of rigorous evidence to support best conducted. Investigations have employed Direct oral challenges can safely27 pre-
the use of specific IgE determination, intrader- a variety of methods ranging from single dose2 clude diagnostically unhelpful, uncomfortable,
mal testing, or skin prick testing for evaluating to graded dosing regimens7, 25, 28,29,31 in a single time-consuming, and costly skin testing prac-
pediatric beta-lactam allergy.27 In comparing day8 or with an extended course.25, 29, 31 Amoxi- tices in low-risk children. In light of growing
clinical pathways against oral testing, Caubet cillin is the recommended beta-lactam for oral evidence that supports direct oral challenges
58 BC Medical Journal vol. 63 no. 2 | march 2021Duke S, Wong T, Toma W Clinical
No penicillin allergy:
Same antibiotic has been taken without reaction
Safe to prescribe
No Low risk of
penicillin allergy:
Safe for direct oral
Symptoms of severe systemic or challenge with amoxicillin
Delayed symptoms (> 2 h since exposure):
cutaneous adverse reaction:
At least one symptom of:
• Mucous membrane involvement
• Macular rash
• Skin desquamation
• Maculopapular rash
• Arthritis/arthralgia
• Urticaria
• Lymphadenopathy
AND
Unverified • Unexplained fever
• Symptom duration > 24 h since discontinuing the antibiotic
penicillin • Kidney or liver involvement
allergy, not
previously
assessed by Yes
an allergist
Immediate symptoms (< 2 h since exposure):
At least one symptom of:
• Urticaria, angioedema Possible
• Wheeze, dyspnea, throat tightness/swelling, voice change penicillin
• Dizziness, syncope, hypotension allergy:
• Vomiting/diarrhea Avoid exposure
AND and refer to
• Symptom duration < 24 h after discontinuing the antibiotic an allergist for
assessment
Inadequate details, or does not fit into either category above
Figure 2. Algorithm for identifying pediatric patients at low risk of true penicillin allergy on the basis of history taking (adapted from Wong et al.20).
in this group, recent clinical guidelines have oral challenges, including recommendations for allergist. That being said, given the remote but
recommended direct oral testing in children in-office anaphylaxis preparedness, are outlined nevertheless important risk of anaphylaxis, it
with histories of mild nonimmediate reactions in Table 2. is critical for these physicians to possess the
to beta-lactams.20,24 knowledge, training, and experience to select
A new CPS Practice Point recommends Future directions suitable patients, interpret clinical features as-
an approach to the evaluation of suspected Pediatric allergists have limited capacity to sociated with allergen exposure, and manage
beta-lactam allergy in children, and provides meet the increasing demand for evaluating severe reactions should they arise in the of-
guidance on patient selection (with reference beta-lactam allergy. Given the high level of safe- fice setting.11 Regarding inpatients, one US
to a succinct algorithm [Figure 2]), test dosing ty of direct oral provocation testing in children hospital implemented a novel clinical guide-
with amoxicillin, and in-office monitoring.20 who are at low risk of true allergy, the burden of line with associated educational sessions for
Although the risk of anaphylaxis is remote evaluating beta-lactam allergy in this group can various inpatient providers, including internal
for carefully selected children, practitioners be eased by the involvement of nonallergist phy- medicine specialists, surgical specialists, nurse
who perform direct oral challenges must be sicians, such as general pediatricians and family practitioners, and physician assistants to aid
prepared to manage these life-threatening physicians. In adhering to the recommendations in the prescription of antibiotics to inpatients
events. Proximity to a hospital is necessary to outlined in the CPS Practice Point,20 primary with reported beta-lactam allergies.32 The clini-
optimize successful outcomes in anaphylaxis. care providers can safely and reliably challenge cal pathway implemented direct two-step oral
Stepwise recommendations for the evaluation a well-defined group of children to oral amoxi- test doses for low-risk patients—a procedure
of childhood beta-lactam allergy with direct cillin in the community, without referral to an that was previously ordered exclusively by
BC Medical Journal vol. 63 no. 2 | March 2021 59Clinical Empowering community physicians to remove erroneous labels of childhood penicillin allergy
Table 2. Steps for evaluating suspected pediatric beta-lactam allergy in the community. allergy labels and prompt appropriate referrals.10
Counseling for patients and their families on
1. Prepare the clinic Anaphylaxis protocol: the implications of drug allergy test results,
for anaphylaxis • Clinic staff should be familiar with a printed, highly visible anaphylaxis protocol
along with appropriate discharge paperwork
management. that has been tailored specifically for the office via input from multidisciplinary
team members.38 and dissemination of results (e.g., pharmacy,
• The protocol should include medication dosages, flow sheets for managing primary care provider), are necessary compo-
respiratory distress and hypotension, and contact information for allied health nents of the de-labeling process.33 A Montreal
services (e.g., ambulance, local emergency department).38
study revealed that 18% of parents refused peni-
In-office anaphylaxis simulation scenarios: cillins for their children despite negative skin
• Regular rehearsal of the anaphylaxis protocol is strongly recommended in testing and drug challenge within the past 4
international guidelines.39
• Roles for providing treatment, calling emergency services, and conducting years.34 In following up with 88 families with
treatment logging should be established. children who had tolerated oral challenges to
• Medical professionals who will be providing treatment should be able to beta-lactams 1 year previously, Vyles and col-
quickly locate and assemble the necessary supplies (e.g., epinephrine, oxygen).
leagues found that 52% of children retained a
Ensure certifications for medical professionals are up to date (e.g., Advanced beta-lactam allergy label on their primary care
Cardiovascular Life Support, Pediatric Advanced Life Support). provider’s electronic medical record, while 28%
Assemble an easily accessible, regularly maintained anaphylaxis cart. of parents reported being less than “comfort-
Essential components: able” with their children receiving beta-lactam
• Injectable aqueous epinephrine (1:1000 solution) with needles and syringes, or
antibiotics, mostly for fear of an allergic re-
epinephrine autoinjector (preferred)
Consider including: action.33 De-labeling strategies must aim to
• Personal protective equipment provide succinct, clear messages to patients and
• Stethoscope their families to avoid erroneous re-labeling of
• Blood pressure cuffs (pediatric and adult sizes)
• Pulse oximeter drug allergy.
• Oral second-generation antihistamine
• Salbutamol metred-dose inhaler with spacer Summary
• Airway adjuncts (e.g., oral or laryngeal mask airway) Unverified beta-lactam allergy in children is
• Oxygen and equipment for administration
• One-way valve face mask with oxygen inlet port
a major public health issue, conferring direct
• Intravenous fluids and equipment for administration patient harm, administrative burdens for hos-
• Automatic electric defibrillator pitals, and health care overspending as the re-
2. Carefully select Figure 2 provides an algorithm for identifying pediatric patients who are at low sult of the needless withholding of first-line
patients for direct risk of true penicillin allergy and are safe for direct oral challenge with amoxicillin. treatment for a large group of patients. This
oral challenge. has led to initiatives to encourage the wide-
3. Conduct direct oral Low-risk individuals can safely undergo a single test dose of amoxicillin (15 spread evaluation of patients with unverified
challenge. mg/kg, max 500 mg), followed by a 1-hour observation period in the clinic to beta-lactam allergy. Direct oral challenges are
confirm tolerance.20 Signs of immediate hypersensitivity should prompt urgent safe in a well-defined group of children com-
assessment and consideration for initiating the anaphylaxis protocol.
prising most cases of unverified beta-lactam
4. Document the Medical records (e.g., community, pharmacy, and hospital records) should be allergy, which obviates the requirement for
outcome. updated. time- and resource-consuming—not to men-
tion painful—antecedent skin testing in this
group. With adequate training and use of clini-
allergists—which resulted in nearly a sevenfold limited evidence of the safety and effectiveness cal guidelines, nonallergist health care providers
increase in beta-lactam challenges, and thereby of nonallergist-implemented direct oral chal- can safely implement direct oral challenges in
improved antimicrobial management with no lenges in children appears encouraging, further low-risk patients and thereby improve capac-
increase in the rate of adverse drug reactions or research is required. ity for beta-lactam allergy evaluation. This will
consultation with allergy subspecialists.32 The Education for health care providers, pa- permit the use of first-line antimicrobial therapy
implementation of antimicrobial stewardship tients, and families is critical in mitigating the in a large group of patients, and subsequently
programs across Canadian centres that simi- ongoing misdiagnosis of beta-lactam allergy. improve patient safety, reduce contributions to
larly empower nonallergist physicians to order Understanding drug hypersensitivity and how antimicrobial resistance, and improve health
test doses would improve rates of de-labeling it differs from nonimmunological adverse drug care costs. n
among inpatients, and thereby improve patient reactions, how to interpret and accurately docu-
safety, mitigate antimicrobial resistance, and ment index events, and how to properly obtain Competing interests
reduce health care costs. Although the existing a drug allergy history will reduce erroneous None declared.
60 BC Medical Journal vol. 63 no. 2 | march 2021Duke S, Wong T, Toma W Clinical
amoxicillin without prior skin testing. J Allergy Clin Im- 30. Lieberman P, Nicklas RA, Oppenheimer J, et al. The
References munol Pract 2019;7:236-243. diagnosis and management of anaphylaxis practice
1. Abrams EM, Atkinson AR, Wong T, Ben-Shoshan, M. The 19. Le Saux N. Position statement: Antimicrobial stew- parameter: 2010 update. J Allergy Clin Immunol 2010;
importance of delabeling β-lactam allergy in children. ardship in daily practice: Managing an important re- 126:477-480.
J Pediatr 2019;204:291-297. source. Canadian Paediatric Society; 2020. www.cps 31. Mori F, Cianferoni A, Barni S, et al. Amoxicillin allergy
2. Caubet J-C, Kaiser L, Lemaître B, et al. The role of peni- .ca/documents/position/antimicrobial-stewardship. in children: Five-day drug provocation test in the di-
cillin in benign skin rashes in childhood: A prospective 20. Wong T, Atkinson A, t’Jong G, et al. Practice point: Beta- agnosis of nonimmediate reactions. J Allergy Clin Im-
study based on drug rechallenge. J Allergy Clin Immu- lactam allergy in the paediatric population. Canadian munol Pract 2015;3:375-380.
nol 2011;127:218-222. Paediatric Society; 2020. www.cps.ca/documents/ 32. Blumenthal KG, Shenoy ES, Varughese CA, et al. Impact
3. Sade K, Holtzer I, Levo Y, Kivity, S. The economic bur- position/beta-lactam-allergy. of a clinical guideline for prescribing antibiotics to in-
den of antibiotic treatment of penicillin-allergic pa- patients reporting penicillin or cephalosporin allergy.
tients in internal medicine wards of a general tertiary Ann Allergy Asthma Immunol 2015;115:294-300.e2.
care hospital. Clin Exp Allergy 2003;33:501-506. 33. Vyles D, Chiu A, Routes J, et al. Antibiotic use after
4. Wright AJ. The penicillins. Mayo Clin Proc 1999;74: Primary care providers removal of penicillin allergy label. Pediatrics 2018;
290-307.
5. Vergison A, Dagan R, Arguedas A, et al. Otitis media can safely and reliably 141:e20173466.
34. Picard M, Paradis L, Nguyen M, et al. Outpatient peni-
and its consequences: Beyond the earache. Lancet In- challenge a well-defined cillin use after negative skin testing and drug chal-
fect Dis 2010;10:195-203.
6. Abrams EM, Wakeman A, Gerstner TV, et al. Prevalence group of children to lenge in a pediatric population. Allergy Asthma Proc
2012;33:160-164.
of beta-lactam allergy: A retrospective chart review of oral amoxicillin in the 35. Kaufman DW, Kelly, JP. Risk of anaphylaxis in a hospi-
drug allergy assessment in a predominantly pediatric tal population in relation to the use of various drugs:
population. Allergy Asthma Clin Immunol 2016;12:4-9. community, without An international study. Pharmacoepidemiol Drug Saf
https://doi.org/10.1186/s13223-016-0165-6 referral to an allergist. 2003;12:195-202.
7. Mill C, Primeau M-N, Medoff E, et al. Assessing the 36. Heckbert SR, Stryker WS, Coltin KL, et al. Serum sickness
diagnostic properties of a graded oral provocation in children after antibiotic exposure: Estimates of oc-
challenge for the diagnosis of immediate and non- currence and morbidity in a health maintenance orga-
immediate reactions to amoxicillin in children. JAMA 21. Choosing Wisely Canada. Infectious disease. Five things nization population. Am J Epidemiol 1990;132:336-342.
Pediatr 2016;170:e160033. physicians and patients should question in infectious 37. Knowles SR, Uetrecht J, Shear NH. Idiosyncratic drug
8. Vyles D, Adams J, Chiu, A, et al. Allergy testing in chil- disease. Accessed 1 June 2020. https://choosingwisely reactions: The reactive metabolite syndromes. Lancet
dren with low-risk penicillin allergy symptoms. Pedi- canada.org/infectious-disease. 2000;356:1587-1591.
atrics 2017;140;e20170471. 22. Choosing Wisely. American Academy of Allergy, 38. Wallace DV. Anaphylaxis in the allergist’s office: Pre-
9. Joint Task Force on Practice Parameters; American Asthma & Immunology: Ten things physicians paring your office and staff for medical emergen-
Academy of Allergy, Asthma and Immunology; Ameri- and patients should question. Accessed 1 June 2020. cies. Allergy Asthma Proc 2013;34:120-131. https://doi
can College of Allergy, Asthma and Immunology; Joint www.choosingwisely.org/societies/american .org/10.1016/j.jaci.2009.10.028
Council of Allergy, Asthma and Immunology. Drug -academy-of-allergy-asthma-immunology. 39. Simons FER, Ardusso LRF, Bilò MB, et al. World aller-
allergy: An updated practice parameter. Ann Allergy 23. White House Office of the Press Secretary. National gy organization guidelines for the assessment and
Asthma Immunol 2010;105:259-273. Action Plan for combating antibiotic-resistant bac- management of anaphylaxis. World Allergy Organ J
10. Norton AE, Konvinse K, Phillips EJ, Broyles, AD. Antibi- teria. March 2015. Accessed 1 June 2020. www.cdc 2011;4:13-37.
otic allergy in pediatrics. Pediatrics 2018;141:e20172497. .gov/drugresistance/pdf/national_action_plan_for 40. DermNet NZ. Exanthems. Accessed 26 July 2020. https://
11. Lang DM, Castells MC, Khan DA, et al. Penicillin Allergy _combating_antibotic-resistant_bacteria.pdf. dermnetnz.org/topics/exanthems.
in Antibiotic Resistance Workgroup. Penicillin allergy 24. Gomes ER, Brockow K, Kuyucu S, et al. Drug hyper-
testing should be performed routinely in patients with sensitivity in children: Report from the pediatric task
self-reported penicillin allergy. J Allergy Clin Immunol force of the EAACI Drug Allergy Interest Group. Allergy
Pract 2017;5:333-334. 2016;71:149-161.
12. Solensky R. Allergy to β-lactam antibiotics. J Allergy Clin 25. Vezir E, Misirlioglu ED, Civelek E, et al. Direct oral provo-
Immunol 2012;130:1442-2.e5. https://doi.org/10.1016/ cation tests in non-immediate mild cutaneous reac-
j.jaci.2012.08.021 tions related to beta-lactam antibiotics. Pediatr Allergy
13. Khan DA, Solensky R. Drug allergy. J Allergy Clin Im- Immunol 2016;27:50-54.
munol 2010;125:126-137. 26. Arnold A, Sommerfield A, Ramgolam A, et al. The role of
14. Macy E, Contreras R. Health care use and serious in- skin testing and extended antibiotic courses in assess-
fection prevalence associated with penicillin “allergy” ment of children with penicillin allergy: An Australian
in hospitalized patients: A cohort study. J Allergy Clin experience. J Paediatr Child Health 2019;55:428-432.
Immunol 2014;133:790-796. 27. Marrs T, Fox AT, Lack G, du Toit G. The diagnosis and
15. Rimawi RH, Cook PP, Gooch M, et al. The impact of management of antibiotic allergy in children: System-
penicillin skin testing on clinical practice and antimi- atic review to inform a contemporary approach. Arch
crobial stewardship. J Hosp Med 2013;8:341-345. Dis Child 2015;100:583-588.
16. Solensky R. Penicillin allergy as a public health mea- 28. Mattheij M, de Vries E. A suspicion of antibiotic allergy
sure. J Allergy Clin Immunol 2014;133:797-798. in children is often incorrect. J Allergy Clin Immunol
17. Xie H, Chen H, Hu Y, et al. Clindamycin-induced acute 2012;129:583.
kidney injury: Large biopsy case series. Am J Nephrol 29. Chambel M, Martins P, Silva I, et al. Drug provocation
2013;38:179-183. tests to betalactam antibiotics: Experience in a paedi-
18. Iammatteo M, Alvarez Arango S, Ferastraoaru D, et atric setting. Allergol Immunopathol 2010;38:300-306.
al. Safety and outcomes of oral graded challenges to
BC Medical Journal vol. 63 no. 2 | March 2021 61Clinical
Luke Witherspoon, MD, MSc, Ryan Flannigan, MD
Fertility treatment options
after vasectomy
Couples who wish to achieve a pregnancy following a vasectomy
should discuss the various treatment options with their specialists
and consider the differences in pregnancy rates, timing to pregnancy,
cost, and invasiveness to patient and partner.
M
ABSTRACT: Canadian men and their female part- en have been having vasectomies history (specifically, hernia repairs), time since
ners are increasingly turning to vasectomy as a for more than 200 years.1 Every vasectomy, and erectile and ejaculatory func-
means of birth control. Although vasectomy is year, approximately 6% of men tion should be assessed. His current and recent
thought of as a permanent form of birth control, (500 000) in the United States undergo a vasec- medication use should also be fully reviewed,
men who wish to attain fertility after having the tomy.2 In Canada, approximately 15% of men with a focus on the use of any anabolic steroids
procedure may undergo a vasectomy reversal to have the procedure, as the shift away from fe- or testosterone supplementation. Discussion
achieve pregnancy with their partner or undergo male sterilization continues.3 However, the in- about the couple’s family planning is likely war-
sperm retrieval and in vitro fertilization/intra crease in vasectomy rates has led to an increased ranted, and should include the number of chil-
cytoplasmic sperm injection (IVF/ICSI). Vasectomy need for fertility options following vasectomy, dren desired and the future desire for sterility.6
reversal patency rates are typically 90.0% to 99.5% as approximately 7.4% of men ultimately regret A focused physical examination should in-
when gold standard surgical techniques, such as having a vasectomy and pursue some type of clude an exam of the inguinal region for sur-
the Goldstein microdot multilayer anastomosis, fertility assessment.4 Four treatment options gical scars, and a full assessment of the testes
are used. Cumulative pregnancy rates with IVF/ exist: vasectomy reversal; sperm retrieval and and scrotal contents. The entire cord structure
ICSI range from 18.2% to 69.4%, depending on in vitro fertilization (IVF) with intracytoplas- should be palpated, with the location of the va-
the female partner’s age. However, sperm retrieval mic sperm injection (ICSI); acquisition of a sectomy identified. The presence of granulomas
procedures and IVF/ICSI, or vasectomy reversal pro- sperm donor for intrauterine insemination or on the testis side of the vas deferens should be
cedures can yield similar efficacy for appropriately IVF/ICSI; or child adoption. Approximately noted, as it may reflect a positive prognosis.6
selected couples. 60% of men who request a vasectomy reversal Most men who undergo vasectomy reversal
are in a new relationship; the rest are in the have a history of fertility,7 but if a man has
same relationship they were in when they had no documented fertility prior to undergoing a
a vasectomy.5 We review the considerations, vasectomy, a formal fertility workup, including
Dr Witherspoon is a sexual medicine and prognostic factors, and outcomes associated hormonal profile, may be undertaken.8
infertility fellow in the Department of with vasectomy reversals and sperm retrieval An assessment of the female partner is also
Urologic Sciences, University of British with IVF/ICSI as potential fertility options required. Although there are no clear guide-
Columbia, and the Department of for couples seeking fertility after a vasectomy. lines about which women require full fertility
Urology, Ottawa Hospital, Ontario. assessments, some guidelines suggest that all
Dr Flannigan is an assistant professor Evaluation and considerations women over 35 years of age should be offered
in the Department of Urologic Sciences, Both partners who are proceeding with a fertil- an expedited fertility evaluation.9 Prior docu-
University of British Columbia, and an ity assessment after vasectomy should have a mented fertility, especially if it was within the
adjunct clinical assistant professor in thorough history taken and undergo a physical same relationship in which they achieved a prior
the Department of Urology, Weill Cornell examination to determine if additional causes pregnancy, is a positive prognostic factor for
Medicine, New York. of infertility may be present. In addition, the pregnancy and live births in couples undergoing
male partner’s fertility history (previous associ- vasectomy reversal.10
This article has been peer reviewed. ated pregnancies and children), inguinal surgery
62 BC Medical Journal vol. 63 no. 2 | march 2021You can also read

















































