Focus on Health Workforce Consequences of Long-term Worklessness New! Training in Research and Medical Education Facts and Figures on Refugee ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Royal Australasian Volume 30 no. 4 AUGUST 2010 College of Physicians Focus on Health Workforce Consequences of Long-term Worklessness New! Training in Research and Medical Education Facts and Figures on Refugee Health High Court Decision on Medical Negligence
Purchase your own
premises
Without a deposit
If you’re thinking about purchasing your own practice
premises, it’s time to talk to Medfin about our
NO DEPOSIT option.
For approved customers, Medfin can lend up to
100% of the purchase price of your practice premises,
leaving your savings free for other investments.
Compare the prices
It’s possible that Medfin’s monthly loan repayments
are similar to your current rental costs.
Want more information?
Contact your local Medfin Relationship Manager
today on 1300 361 122 .
Don’t have time to phone? Visit medfin.com.au
and request a quote.
Important information: Because we do not know your personal
circumstances please consider whether this product is
appropriate for your circumstances. Approved customers only.
Subject to credit assessment. Fees and charges may apply.
Medfin Australia Pty Limited ABN 89 070 811 148. A wholly
owned subsidiary of National Australia Bank Limited, and part
of the NAB Health specialist business. (RACP8/10)
Medfin – finance for your: Car • Equipment • Practice • Property • Cash flow needs
2 RACP News August 2010
Contents
WORKFORCE
5 Long-term worklessness: health risk equivalent to smoking
10 packs of cigarettes a day
7 Towards a sustainable, affordable and fit-for-purpose New Zealand health workforce
9 Managing the medical workforce
11 International Medical Graduates in the Australian and NZ workforce
12 eHealth News! Healthcare Identifiers
EDUCATION
14 Physician Readiness for Expert Practice (PREP): Advanced Training
16 New! Advanced Training in Academic Medicine
17 Introducing PREP into Advanced Training: a trial of formative assessment
in Advanced Training in Geriatric Medicine
18 Supervisor Workshops
18 Upcoming Advanced Training Supervisor Workshops
18 Education policy
19 What are our trainee physicians telling us? Insights from the 2009 Basic
and Advanced Trainee Surveys
20 CPD—Where to from here?
20 What are your MyCPD credits really worth?
21 Easy access to National Prescribing Curriculum Modules for trainees
and Fellows
21 Specialist Training Program
22 Darwin and Alice Springs PREP Roadshow
23 Online Medical Education Community of Learning
YEAR OF THE TRAINEE
31 Postcard from Oxford
31 Procrastination—our enemy and friend
Emperor penguin parents and chicks at Auster Rookery,
50 km east of Mawson Station in the Australian
RESEARCH AND EDUCATION FOUNDATION Antarctic Territory.
35 Please help our young physician researchers achieve their goals
36 Applications now open for the 2011 Jacquot Awards Cover photo by Gary Dowse, Public Health Physician,
who works in communicable disease control in the
ARTICLES AND INFORMATION Department of Health, Western Australia.
4 Letter from the President
6 History of Medicine Library Lectures 2010
12 Get RACP News delivered straight to your in box
12 Send in your poetry
13 RACP Congress 2011 Darwin
24 Broader protection, not just border protection
26 RACP (Paediatrics & Child Health Division) and the National Health and
Hospital Reform Agenda
28 The role of non-pecuniary interests in medical decision making: Send us your photos
excerpt from a conversation
29 Medical negligence—no recovery for loss of chance claim Please send us your interesting digital
30 A thank you photographs to be considered for publication
32 Sydney offices on the move—creating a better College for everyone in RACP News.
33 Dr Geoffrey Robinson’s farewell
File formats of 300dpi, at A4 size, can be
34 Queen’s Birthday Honours 2010
36 Fellow commended in Victorian Premier’s Medical Research Awards emailed as jpegs to racpnews@racp.edu.au
36 Fellows welcome to submit articles to RACP News
37 A leading physician Allan Kerr Grant AO
38 Book reviews
40 Letter to the Editor
41 After Hours: Labyrinth building—a new dimension to walking in circles
43 Territory Horizons
44 Classifieds
A publication of The Royal Australasian College of Physicians A.C.N. 000 039 047 ISSN 1444-6324 145 Macquarie Street, Sydney NSW 2000. http://www.racp.edu.au
Project Editor: Kathryn Lamberton | Advertising Officer: Fay Varvaritis | Editorial Board: Professor John Kolbe, Dr Jennifer Alexander, Professor Kevin Forsyth, Dr Gervase Chaney,
Dr Jemma Anderson, Sasha Grebe. Circulation Approximately 17,000 Fellows and trainees of The Royal Australasian College of Physicians, including the Faculties of Public
Health, Rehabilitation, and Occupational and Environmental Medicine and the Chapters of Palliative Medicine, Addiction Medicine and Sexual Health Medicine. Subscribers
represent over 20 medical specialties. The magazine is distributed throughout Australia, New Zealand and 47 countries throughout the world.
Advertising Booking Copy mm deep x * Australian advertisers will
Issue Dates Deadlines Deadlines Size mm wide $* be charged an additional 10%
October 2010 26 August 2010 6 September 2010 Full page 297 x 210 3,200 GST. Multiple-issue discounts are
December 2010 26 October 2010 5 November 2010 1/2 page landscape 116 x 172 1,600 available. 20% discount for RACP
1/2 page portrait 240 x 84 1,600 Fellows. Inserts are accepted and
1/4 page 116 x 84 800 can be tailored to suit your
1/8 page 58 x 84 400 distribution needs.
Premium Positions: Inside front cover or outside back cover, Full Page: $3,400
More information www.racp.edu.au Tel: +61 2 9256 5482 Fax: +61 2 9256 9697 racpnewsads@racp.edu.au
Articles, Letters to the Editor, etc:
Contact details RACP News, RACP, 145 Macquarie St, Sydney NSW 2000 Tel: +61 2 9256 5444 Fax: +61 2 9256 9697 racpnews@racp.edu.au
The views expressed in RACP News are not necessarily the views of the College. Publication of advertisements does not constitute endorsement
The Royal Australasian
by The Royal Australasian College of Physicians of the products advertised. Designed and produced by Weavers Design Group www.weavers.com.au College of Physicians
RACP News August 2010 3
Letter from the President
ADDRESSING THE CHALLENGES
developing closer working relationships Director of Education since 2006, Kevin
with other Colleges, both nationally and has made an enormous contribution to
internationally. education and to the College as a whole.
When Kevin was appointed, the College
Following the appointment of new senior was facing enormous challenges in the
members of staff at the College, the CEO, form of the AMC accreditation process and
Jennifer Alexander, has established a very the need for education in the College to
capable and enthusiastic Senior Leadership conform to medical education best practice.
Group (SLG). Among the various activities The changes in education introduced
being undertaken by this group is the by Kevin have been characterised by
review of all the By-laws of the College. innovation, academic underpinning and a
Following the Governance Review, By- coordinated and comprehensive approach.
laws were developed for most but not Kevin instilled a culture that strives to ensure
all College committees. The expectation that our education standards are the highest
was that an overhaul would be necessary possible and that we maintain our focus
after a year or two to ensure harmony and on world’s best practice. He has moved the
consistency across the College, to embrace College to the ‘cutting edge’ of vocational
changes that had become necessary and to education. Initially, the major focus was
C
reflect more accurately the activity of the on PREP; the current focus is on PREP
ongratulations to those trainees committees.
who have recently passed their AT while acknowledging that the major
College examinations. This At its next meeting the Board will consider focus now needs to shift to CPD and the
the new By-laws for the Board and the need to address challenging issues such as
seems an opportune time to
Board Executive as well as the generic revalidation and assessment of competence.
inform the Fellowship that the Board has
Aspects of these new programs, including
commissioned a review of all assessments By-laws that will apply to all committees
but not limited to the Professional Qualities
undertaken by the College. The review of the College (unless specified otherwise).
Curriculum, the integrated PREP program,
team has not yet been finalised but most Importantly, this body of work will include
instruments such as the Professional
likely will include medical education the development of By-laws for State and
Qualities Reflection, and the establishment
experts from several overseas Colleges. Territory Committees. It is my hope that
of an academic SAC, have drawn highly
This review is to determine whether our these will reflect the appropriate devolution
favourable comments within Australasia and
assessments are in line with contemporary of activities to these very important
internationally.
medical education best practice and committees of the College. It is clear that
appropriately aligned with the curriculum. the delivery of educational programs is At various meetings, it has become very
The review will also determine the best heavily dependent on local commitment clear to me the enormous respect that
timing and format for the assessments and leadership. exists for Kevin’s opinions and the high
and take into account the practical and esteem in which he is held in the field of
In addition, there are ‘local’ issues in medical education. Initially the changes
logistical considerations of mounting
which it is appropriate for our Fellows in education that took place within the
clinical examinations for an increasing
to be engaged. Increased appreciation College were not embraced by all, with
number of trainees.
of the important roles of State/Territory some taking the view, ‘If it ain’t broke, don’t
As you are all well aware, the College Committees is reflected in plans for fix it’. Hopefully now, all can appreciate the
is facing a number of challenges, both the upgrading of offices as well as the enormous benefits of the new education
internal and external. It is clear, however, appointment of Medical Education Officers programs, although the barriers that Kevin
that our College is not alone. This was (MEOs) and staff with Policy & Advocacy had to overcome in these early times should
highlighted at a recent Committee skills to the State offices. not be underestimated. The fact that he
of Presidents of Medical Colleges addressed and overcame these difficulties
In 2009 the Board of the College developed
workshop on supervision, where there with tolerance and good grace is testament
a Statement of Strategic Intent (SoSI) that
was remarkable agreement on the to the strength and quality of his character.
outlined the College’s strategic initiatives
generic requirements for supervisors and Under Kevin’s leadership, the Education
for 2009–2012. In July the Board and the
for the supervision environment. The Deanery has increased considerably in size
SLG met to review and refine the SoSI. Even
RACP has had a number of meetings and, commensurate with this, the education
in a year in which the College continues
with the Royal Australasian College output has increased enormously. Although
to develop policies and procedures for
of Surgeons to explore a closer and Kevin will remain in his current role for a
usual College activities, and in which there
mutually beneficial relationship. This number of months, it seems appropriate
have been a number of issues that have
might include such things as sharing to recognise his enormous contribution at
demanded immediate attention, it was
resources, joint educational and other this time and the fact that the College and
pleasing to reflect on the progress that has
endeavours, and common submissions its Fellows owe him a great debt. I am sure
been made in a number of these important
to external agencies. In a similar vein, we you will wish to join with me in sincerely
areas during the last year. The revised SoSI
are having detailed discussions with the thanking Kevin and wishing him every
will be available on the College website.
Royal College of Physicians and Surgeons success in the future.
of Canada with whom we have had joint In June, the Dean, Professor Kevin Forsyth,
John Kolbe
workshops and a close relationship over advised that he would be leaving his
President
the last few years. Far from seeing this current role at the end of December 2010.
as an exclusive relationship, we are also Serving close to five years as Dean and
4 RACP News August 2010
Workforce
LONG-TERM WORKLESSNESS: HEALTH RISK
EQUIVALENT TO SMOKING 10 PACKS OF
CIGARETTES A DAY
‘L
ong-term worklessness,’
Professor Sir Mansel Aylward
said during his recent visit
to Australasia, ‘is one of the
greatest known risks to Public Health.
It has a health risk equivalent to that of
smoking ten packs of cigarettes per day.1
After six months out of work, the suicide
rate in young men is increased forty
times.2 For longer term worklessness, the
general suicide rate is increased six times.3
Worklessness has a health risk and life
expectancy reduction greater than many
“killer diseases”.4 And worklessness is
actually riskier than most dangerous jobs, Professor Sir Mansel Aylward launched the Robin Chase, President of the AFOEM, Professor
including construction and working on Position Statement, Realising the Health Benefits of Sir Mansel Aylward, and Mary Wyatt, Chair,
the North Sea.’5 Work, in Sydney and Auckland during his recent AFOEM Policy and Advocacy Committee, at the
visit to Australasia. Sydney launch.
Sir Mansel, a prominent UK health
reformer, was here as a guest of the and spellbinding in the way he gets • 70 days the chance of ever getting
Australasian Faculty of Occupational and the messages over. We had some great back to work is 35%.7
Environmental Medicine (AFOEM), under feedback afterwards, including statements
the auspices of the Royal Australasian Research demonstrates that
such as “I could have listened to him all
College of Physicians, to launch AFOEM’s unemployment has a significant negative
day!”’
Position Statement, Realising the Health impact on physical health and mental
Benefits of Work. The Position Statement Not all work is good for all people; and health, and results in increased mortality
was launched in Sydney on 18 May 2010 work must be safe. With these provisos, rates. Conversely, research demonstrates
and in Auckland on 25 May 2010. Realising the Health Benefits of Work that not only do the beneficial effects of
makes recommendations for treating work outweigh the risks, but the health
The launches were attended by business practitioners, employers and government, benefits of work are even greater than the
groups, unions, workers’ compensation based on the idea that work, in general, harmful effects of long-term unemployment
authorities, rehabilitation providers and is the most effective means of improving or prolonged sickness absence.8
other stakeholders. In both Australia the wellbeing of individuals, their families
and New Zealand there was enthusiastic and their communities.
support for the message of Realising the
Health Benefits of Work, and considerable Despite the enthusiasm of key
Suitable work has
interest in affecting meaningful change. stakeholders, the message that ‘work been shown to benefit
is generally good for health’ does not people suffering
For Dr David Beaumont, Co-chair of
yet seem to have achieved widespread
AFOEM’s Position Statement Working
Group, ‘The highlight of the Auckland
acceptance in Australia and New Zealand. from a wide range
In fact, according to the Return to Work
launch was the coup of having Sir
Monitor, a survey of workers with work
of psychiatric
Mansel present the keynote and official
launch of the Position Statement—he is injuries that provides an annual snapshot conditions … anxiety,
of return to work trends, over the last
absolutely passionate about the agenda,
three years return to work rates have
depression, bipolar
declined in Australia and over the last two disorders and
Evidence shows years in New Zealand. Last year, 28% of
schizophrenia.
injured workers surveyed in Australia and
that the long- 25% of workers in New Zealand were
term negative not in paid employment six months after
AFOEM now says with confidence that
lodging a workers’ compensation claim
consequences of in Australia or an accident compensation work, in general, is good for health and
wellbeing.
advising a patient to claim in New Zealand.6
Despite this compelling evidence, in
remain away from This is particularly worrying given that
both Australia and New Zealand more
work absence tends to perpetuate itself:
work or to take time that is, the longer someone is off work, and more people with mild to moderate
musculoskeletal and/or mental health
off work … are often the less likely they become ever to return.
problems are being certified as unfit for
If the person is off work for:
greater than those work.9
• 20 days the chance of ever getting
of the original health back to work is 70% Realising the Health Benefits of Work states
that we can begin to address these
problem. • 45 days the chance of ever getting issues by shifting popular perceptions of
back to work is 50%, and common health problems.
RACP News August 2010 5
Workforce
Studies have shown that in most cases Work has already begun on the first of Proceedings of an RSM Symposium. London:
an early return to work (or remaining these recommendations, the consensus Royal Society of Medicine Press; 41–46.
at work) is beneficial for health and statement. Indeed, due to stakeholder 3. Bartley M, Sacker A, Schoon I, Kelly M,
wellbeing, and that people with enthusiasm for the project, the consensus Carmona C (2005). Work, non-work, job
musculoskeletal conditions who are statement is now likely to be endorsed by satisfaction and psychological health: evidence
helped to return to work enjoy better business groups, unions, some workers’ review. Health Development Agency.
health than those who remain off work.10 compensation authorities and other
relevant parties, as well as the medical 4. Aylward M, Waddell G (2005). The scientific
Suitable work has also been shown to community. and conceptual basis of incapacity benefits.
benefit people suffering from a wide London: The Stationery Office.
range of psychiatric conditions. These Dr Mary Wyatt, Chair of the AFOEM’s
conditions include anxiety, depression, Policy and Advocacy Committee, is 5. Aylward M (2008). No one written off:
bipolar disorders and schizophrenia. The determined to maintain the momentum reforming welfare to reward responsibility.
established by the positive reception of Consultation Event DWP; Welfare Reform
potentially negative impacts of work on
Green Paper. Cardiff.
mental health must be balanced against Realising the Health Benefits of Work.
awareness that unemployment may also 6. Statistics New Zealand (2007). Household
‘AFOEM now hopes to further the
have serious consequences for mental Labour Force Survey.
conversation about how the health
health.
and wellbeing benefits of work can be 7. Johnson D, Fry T (2002). Factors affecting
The medical community has a special intensified,’ she said. ‘Our next position return to work after injury: a study for the
responsibility to take the message of statement will examine the evidence Victorian WorkCover Authority. Melbourne:
Realising the Health Benefits of Work on about the relationship between health Melbourne Institute of Applied Economic
board: the evidence shows that the long- and productivity in the workplace.’ and Social Research.
term negative consequences of advising
AFOEM is also seeking financial partners 8. Waddell G, Burton A (2006). Is work good
a patient to remain away from work or to
for an Australasian cost–benefit analysis for your health and well-being? London: The
take time off work, or agreeing with them
of investments in workplace health and Stationery Office.
that time off work is a potentially helpful
wellbeing. International studies indicate
course of action, are often greater than 9. Organisation for Economic Co-operation and
that such investments yield excellent
those of the original health problem. Development (2007). Sickness, disability and
returns, in terms of both value for money work: breaking the barriers (Vol. 2)—Australia,
The key recommendations of Realising the and health outcomes. Luxembourg, Spain and the United Kingdom.
Health Benefits of Work are that: Paris: Organisation for Economic
Both unions and business are behind
this agenda. In Australia, Geoff Fary of Co-operation and Development.
1. The medical community develop
a consensus statement regarding the the Australian Council of Trade Unions 10. Lõtters F, Hogg-Johnson S, Burdorf A
positive relationship between health suggested approaching the Treasurer (2005). Health status, its perceptions, and
and work and the negative Wayne Swan for funding for such a effect on return to work and recurrent sick
consequences of long-term work cost–benefit analysis. In New Zealand, leave. Spine;30:1086–1092. 10.97/01.
absence and unemployment. Paul MacKay of Business New Zealand brs.0000161484.89398.48.
reiterated the need for action. ‘More of
2. The education of treating practitioners this,’ he told the audience at the launch.
incorporate training in workplace ‘And fast!’ In fact, as Mary Wyatt and
occupational health and vocational Robin Chase were leaving the Sydney
rehabilitation, and sickness launch at the Sofitel, as if on cue Wayne
certification practices, and that the
medical community provide leadership
Swan appeared and as quick as a flash HISTORY OF MEDICINE
Mary had provided the Treasurer with
on these issues. a copy of the Position Statement and a
LIBRARY LECTURES 2010
3. Health professionals responsibly 30-second doorstop on why this was such
an important issue. The last two lectures for the year will
promote the health benefits of work to
be held at 6.30 pm at the RACP
their patients. For more information about Realising Education Centre, Level 8, 52 Phillip
4. Governments obtain and publicise the Health Benefits of Work, or to assist Street, Sydney. Join us for wine, coffee
accurate data about the level of work AFOEM with the agenda outlined above, and light refreshments after the lecture.
incapacity in Australia and New please contact Andrew Messner on 02
9256 9602 or go to the AFOEM website: Entry: $10 at the door
Zealand.
http://afoem.racp.edu.au/page/media- Bookings: Phone Liz Rouse
5. Governments launch public health and-news/realising-the-health-benefits- (02) 9256 5413 or email
campaigns, directed at employers, of-work. racplib@racp.edu.au
workers, medical practitioners and the
general public to promote the Dr David Beaumont and Dr Mary Wyatt On Monday, 6 September, Ross Halpin
message that ‘Work, in general, is Australasian Faculty of Occupational & will speak on A Matter of Concern: the
good for health and wellbeing. Environmental Medicine ethical dilemma of using Nazi medical
research data in contemporary medical
6. Employers move beyond legislative References research.
requirements to embrace the spirit of
inclusive employment practices, 1. Ross J (1995). Where do real dangers lie? On Monday, 1 November, Dr Michael
Smithsonian;8:42–53.
workplace safety, health and Kennedy will examine Medicine in Early
wellbeing, and best practice injury 2. Wessely S (2004). Mental health issues. In: Colonial Australia.
management. Holland-Elliot K, ed. What about the workers?
6 RACP News August 2010
TOWARDS A SUSTAINABLE, AFFORDABLE
AND FIT-FOR-PURPOSE NEW ZEALAND
HEALTH WORKFORCE
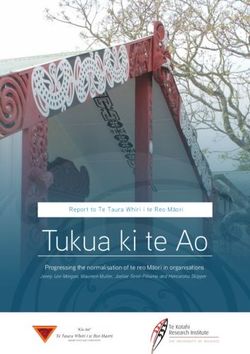
Figure 1: Cumulative percentage change in GDP and health spending in New Zealand
Professor Des Gorman
A
s is true for other OECD nations, Third, our nexus with Australia is agencies and so on which are engaged in
New Zealand faces a demand– problematic and primarily serves some way in health workforce planning
supply–affordability mismatch Australia’s interests. The level of and or training!
in regard to health services. emigration of doctors and nurses
However, our mismatch is exaggerated Seventh, there is a schism between the
to Australia is unsustainable for us;
for a number of reasons. governors of the New Zealand health
remuneration differences in regard to
system and the health workforce. There
First, contextually, and most importantly, some of the less popular-to-work-in
are a number of local drivers of this
New Zealanders regard universal and Australian states is certainly part of the
dislocation that are beyond the scope
unconstrained access to excellent problem, but vocational discomfort is far
of this review, but the workforce is
healthcare as an undeniable birthright. more complex and multi-factorial than demonstrably segregated and tribal. A
This birthright is integral to a core pay, car parks and locker considerations guild model best explains most recent
concept of an enabling and caring alone. behaviour.
society and, in turn, underpins much Fourth, and related to the item above,
of our perspective of citizenship. The Eighth, there is an aggregate of other
New Zealand has a consequential and interactive and confounding and
result is an expectation that is difficult to similarly unsustainable reliance on
meet—already, 20% of our Government’s complex factors that are germane to
immigrant health workers. this discussion, including our Health Act
total spend is on health. In the last two
budgets, health has been allocated Fifth, shortages of key health workers such not requiring the public health system
50% and 40% of all the new money as doctors, midwives, dentists and nurses to attend to the training of the health
respectively. The other 30 odd ministries are exaggerated by these workforces workforce, the nature of our largely
and departments have had to ‘make do’ being poorly distributed against need publicly funded but privately and publicly
with the other half. No one knows for by way of discipline, ethnicity, culture, delivered health system, along with the
sure, but based on factors such as the demography and geography. extraordinary reality of 20 district health
ageing of the New Zealand population boards and more than 80 primary health
and the increase in availability of and organisations (for a country with the
access to end-of-life high technology population of the State of Victoria) and
and often low-utility technologies, the
The New Zealand funding of undergraduate health worker
demand for health services will increase Health System, then, students by an education commission
by somewhere between 40% and 100% that is not imbedded in the health system
over the next decade. My ‘informed’
is both financially or in health system planning.
guess is at the 100% end of this threatened and The New Zealand Health System, then,
spectrum.
threatening (to all is both financially threatened and
Second, compared to many other threatening (to all other agencies of the
members of the OECD, New Zealand is other agencies of the State). A sense of urgency is insightful for
small and relatively poor. Since 1950, State). at least three reasons. The mismatch of
local health expenditure has increased by demand, supply and affordability is great.
417%, compared with a growth in GDP Assuming GDP growth of 3% per annum
over the same period of only 133% (see Sixth, despite being ‘submerged’ in data, and that health continues to receive
Figure 1). It is noteworthy, and worrying, most of our health planning has not been about 20% of Government spend, then
that most of the divergence arises after and is not well informed by intelligence. over the next decade a probable doubling
1999/2000. To date, we have found more than 500 of demand will need to be adequately
RACP News August 2010 7
Workforce
addressed by way of a far more modest of the year we will have completed
40% increase in funding. To avoid the a number of service reviews (e.g.
system substantially failing through acute hospital services, anaesthesia
The New Zealand
differential decreasing access to health services, elective surgery, diabetes, health system has to
services, the conundrum presented gastroenterology, mental health, vision
here will need to be addressed by health) and the outcomes of these will
become increasingly
health workers doing many things very determine the number and scope of New Zealand need-
differently. health worker training positions we fund
in 2011.
centric and there are
The second and third drivers of urgency
relate to the understandable expectation The planning cycle we are using is
many lessons for us
of the health workforce for meaningful illustrated in Figure 2 and our process to learn from how
of service review is shown in Figure 3.
reform of what are often both archaic
and arcane service configurations and In addition to a requirement to meet a
Canada ‘survives
models of care (as compared to the best-guess 100% increase in demand and relatively
over the next decade, but to constrain
churn in governance models) and to our
any funding increase over this period to
prospers’ ...
Government’s expectation that clinical
leadership is at the core of any solution 40% or less, we have agreed some other
that will result in a fit-for-purpose health planning values and principles.
service. My concern here is not the Second, healthcare will be largely
logic of clinical leadership in either a Figure 2: Planning cycle for reform delivered by way of healthcare
clinical or a corporate sense, but the of health services teams that are integrated and multi-
ability of health workers to meet this professional and where team leadership
leadership challenge. Our emphasis on is both contextual and values-based.
professionalism for some time has been All health workers will have clinical and
heavy on ethics and communication and corporate leadership responsibilities. The
light on education and leadership. hidden curriculum of apprenticeship
should be used to develop the broader
The way ahead involves both a structural domains of professionalism and an
change in health system governance Institute of Health Leadership will almost
that establishes the correct relationship certainly be needed.
between a dog (health need) and its
tail (services and models of care, and Third, disruptive innovations of
consequential workforce, IT and capital service configurations and models of
planning), and diversification of the heathcare will become business as
health workforce through intelligence, usual. Nevertheless, role substitution
innovation and clinical leadership. The and scope extensions should be sensible
former is underway and our Minister in the context of what are the values,
of Health has formed Health Workforce skills, knowledge base and culture of
New Zealand (HWNZ), initially as the to-be-extended health profession.
Figure 3: Process of service review
a business unit in the Ministry of Remunerative and other barriers to
Health that reports directly to him, rationalisation of services and models
to consolidate activity and to lead will need to be identified and addressed
the planning, funding, training and without favour.
deployment of the health workforce.
Fourth, the private health sector derives
The mission of HWNZ is to ensure a
both direct and indirect benefit from
fit-for-purpose and sustainable health
workforce. There is a determination to Vote Health and consequently must also
have a whole of health workforce and a contribute to the broader domains of the
whole of educational continuum view New Zealand health service.
and, as cited above, we have adopted Fifth, the New Zealand health workforce
core values of intelligent planning, should look as much as is possible like the
clinical leadership, and innovative community it serves. Selection processes
service configurations and models of First, healthcare must be patient and not need to be accordingly attentive and
care. Already, we are trialling practice practitioner centred. Most often we are both affirmation and immersion schemes
assistants, extended nursing and using an aggregate of ‘idealised patient- will be needed. The New Zealand health
pharmacist roles, and are well underway journeys’ to develop and evaluate system has to become increasingly New
on a comprehensive revision of the services and models for 2020. A broad Zealand need-centric and there are many
training and deployment of general application of a care-navigator scheme lessons for us to learn from how Canada
medical practitioners. The latter will that operates across all social agencies ‘survives and relatively prospers’ alongside
include both community- and hospital- and is known in New Zealand as whanau a bigger and more affluent country that
based scopes of practice. By the end ora is intended. has a relatively greater health expenditure.
8 RACP News August 2010
MANAGING THE
MEDICAL WORKFORCE
Figure 1: Clinical workforce spending as a
The challenge we percentage of all healthcare spending1
face is to ensure a United States 65
national birthright of Germany 62
United Kingdom 60
universal access to Australia 53
excellent healthcare Japan 45
for the future workers as the weekly working hours
generations of all for both men and women in Australia
is in decline (45.4 to 43.7 hours from
New Zealanders. It 2001 to 2005). For example, women
will be deliberately and younger workers tend to work fewer
hours, on average, than their older male
clinically led, counterparts, resulting in fewer productive
Dr Lloyd Nash hours per medical worker.
intelligently
Possibly as a consequence of these policies,
informed and very Fulfilling the promise Australia has struggled to address its
innovative. The great promise of the medical
workforce shortage and maldistribution of
workers, particularly in outer metropolitan,
profession is to heal and care for people, rural and remote areas. An overseas trained
ease pain and suffering, prevent disease workforce has duly provided services to
and mitigate risk. The Australian medical these parts of the community. Australia
Sixth, the New Zealand Health System has
profession now finds itself facing a is a net receiver of medical workers from
to be sustainable and affordable. Given
challenge to deliver on this promise as the international marketplace, with 25%
this principle and the intrinsic uncertainty structural impediments are imposed by of doctors working in Australia overseas
in health planning, ‘slow to train’ and critical shortages and maldistribution of trained, up from 19% in 1996 (44% in
expensive health workers should be medical workers. New Zealand). Many of these fully trained
retained in general scopes of training and workers are from the developing world,
practice as much as and for as long as is A shifting target which takes advantage of poorer source
possible. The health workforce needs to be countries and potentially leaves them with
incentivised in ways that encourage good Critical shortages of workers are driven by
a worker shortage.
practice and we must invest in and value a tight supply of medical workers, but also
by an unpredictable and exponential rising Faced with this reality, Commonwealth
career progression, training and status.
demand for services. Workforce planning governments have made a complete policy
This will help to distinguish New Zealand
is fraught with difficulty because the reversal with a recent impetus to massively
as a desirable place to study, learn and health policy aims of governments are in expand the numbers of new graduates
work. We are in the process of enhancing conflict. On the one hand is the objective by deregulating the medical marketplace
apprenticeships, have introduced a 3-R for better health, as the careful and for higher education, creating new
scheme (retain, repatriate and recruit) responsible management of the wellbeing medical schools and removing the cap
and are trialling very new models of of the population is a key responsibility of on full-fee paying international students.
employment that underpin a focus government. But on the other hand, this This will have the effect of dramatically
on career progression and training. responsibility must be weighed against the increasing supply over the next decade,
The two major training packages are many other responsibilities of government, but is unlikely to abolish our reliance on an
Voluntary Bonding, which is for the and healthcare is indeed a costly and overseas trained workforce, nor adequately
early postgraduate trainee, and Special labour-intensive business. The workforce meet rising demand.
Engagements, which are for the Advanced is by far the largest cost to the health
Trainee, and they will provide support
system; in 2008 Australia spent 53% of its Growing older
total healthcare spending on the clinical
both in New Zealand and overseas. Details
workforce (see Figure 1). It is also the and wider
on these schemes are available on our responsibility of government to contain
website . Workforce shortages have been
those soaring costs.
compounded by increased demand,
In summary, the challenge we face is to Largely as a result of this tension, which has been unprecedented. This is a
ensure a national birthright of universal successive governments have sought result of four main factors: demographic
access to excellent healthcare for the to first reduce the number of medical change, epidemiological transition,
future generations of all New Zealanders. graduates by limiting intakes into medical improved technology, and changing
This challenge is being taken up by schools and then to limit the number community expectation.
HWNZ. It will be deliberately clinically led, of practitioners allowed to operate
intelligently informed and very innovative. independently by separating Medicare Australia’s population is both growing
entitlements from medical registration. and ageing. The population is expected
Professor Des Gorman AFOEM Furthermore, changing patterns of to increase from 18.3 million people in
Executive Chairman of Health Workforce workforce participation have also sought 1996 to 25.6 million by 2021, a 2.7%
New Zealand to reduce the supply of available medical increase. People aged 70 years and over
RACP News August 2010 9
Workforce
are projected to account for 12.1% of encouraging people to take more control caring for their own health and
the total population by the year 2021 of their health, and the fear of losing wellbeing. Productivity is sacrificed as
(compared to 8.3% of the population in health and independence has led to high workload approaches a breakpoint.
1996). The growth rate of those aged demand for screening modalities. The
• Continuous professional development.
85 years and over is projected to be even Australian public have shown little patience
Medical workers need up-to-date
more significant. Between 2006 and 2016 with surgical waiting lists and emergency
knowledge to perform well. Rapid
alone, the number of people over 85 department waiting times, demanding
increases in knowledge and changing
years will have grown by over 60%. The ever more from their health services.
health systems reinforce the need for
changing age profile of the population a systematic, ongoing, cyclical process
has clear implications for the nature of Leadership required of self-directed learning. The system
the burden of disease the workforce should structure professional
With critical shortages across the medical
must respond to. Already Australia has development for all workers through
workforce now and into the future, the
seen a transition to chronic and ‘lifestyle’ formal feedback, mentoring and
workforce will need to become more
diseases; the current top three burdens of productive to maximise performance—that
secondment.
disease for Australian men are ischaemic is, producing the best health services and • Remuneration and incentives.
heart disease, anxiety and depression, and health outcomes possible by reducing Remuneration can distort medical
type 2 diabetes. This is partly driven by an waste of staff time and skills. This will have worker and health system performance.
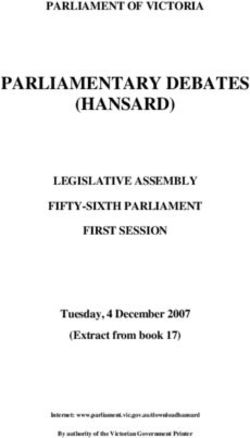
epidemic in obesity (see Figure 2). an immediate impact on the delivery of Gross disparities in remuneration
services and will be associated with better between procedural and non-procedural
A crowded motivation. work in Australia is driving medical
workers to take up higher remuneration
waiting room There are several ways that the health
specialties leaving ‘low status’ areas, such
system can support medical workers to be as aged care, mental health and
As the proportion of the population ages,
more productive: Indigenous health, in shortage.
there will be an increase in the chronic
degenerative diseases seen with age such • Team building and clinical leadership. Remuneration should be brought into
as dementia, osteoarthritis and heart Teamwork can improve wellbeing of line to recognise the value of consultative
failure. New technologies, treatment workers and improve quality of care. medicine and the epidemiological
modalities and pharmaceuticals may Clinical leadership can provide vision, transition to complex care.
change the specific burden of disease in encourage innovation, and create a • Infrastructure. The physical environment
ways that are unpredictable. For example, culture of benchmarking and as well as services and technologies
minimally invasive techniques such as comparison. Teamwork can improve available to workers can improve
coronary angioplasty have reduced the performance, job satisfaction and performance. Essential support might
demand for bypass surgery, but what is motivation by providing mutual include information technology such
certain is that there will be significantly support, education and feedback on as portable wireless devices, electronic
higher numbers of elderly people to be good performance. decision support, electronic health
cared for, with ever more complex care
• Workload management. Workforce recording and prescribing.
needs. Augmenting that demand in
ways not yet clear are the community planning and rostering must take into • Task liberation and new cadres. This
expectations for treatment. With increasing account the competing demands on involves the optimal deployment of
knowledge and wealth, individuals have the time of medical workers to ensure available workforce skills. A doctor is
become more demanding when it comes workers are reasonably capable of a highly skilled practitioner with
to their health needs. Popular media are meeting those demands while also unique ability to make a diagnosis and
recommend a plan of management.
Figure 2: Proportion of obese Australians by age group (1995–2005)2 These complex tasks should remain
the focus of the doctor’s work, where
the doctor can be liberated from other
25.0% tasks. It might involve creating new
cadres of workers to take on new roles
22.1% with limited and specific training in the
20.0% 20.6% area of their work, which might include
18.0% simple procedures or care coordination.
17.9% This could extend health system
15.0%
15.1% performance and improve job
satisfaction and motivation.
19.7%
10.0% 19.0%
16.1%
17.4%
10.4% Health promise into
5.0%
7.0%
12.8%
9.9%
health action
7.6%
Medical workers are the human links that
4.9% 9.8% 11.2% 15.0% 15.7% 12.1% 6.0%
translate health promise into health action.
0.0% But it is difficult to match the supply of
18-24 25-34 36-44 45-54 55-64 65-74 >75
workers with demand for services, because
the challenges faced are constantly
changing. With demographic change
1995 2001 2005
and epidemiological transition, demand
10 RACP News August 2010grows in unpredictable ways depending innovate to maximise the productivity of References
on technological development, new the current workforce, to grow the supply 1. Bhatia N, Meredith D, Riahi F (2009).
treatment modalities and community of medical workers and to manage global Managing the clinical workforce. McKinsey
expectations. What is certain is that migration in ethical ways. Only then can Quarterly; December.
there are massive drivers of demand that our health promise be fulfilled. 2. National Health Workforce Taskforce (2009).
coincide with a current undersupply in Health workforce in Australia and factors for
the Australian medical workforce that new Dr Lloyd Nash current shortages. KPMG.
graduates will only go part of the way to College Trainees’ Committee and
address. We, as clinical leaders, need to Workforce EAG
INTERNATIONAL MEDICAL GRADUATES IN
THE AUSTRALIAN AND NZ WORKFORCE
I
nternational Medical Graduates undergoing Specialist and Area of Need the majority of OTPs assessed are resident
(IMGs) are an incredibly important assessment and is open to all RACP in Queensland (21%) and New South
part of the Australian and New trainees and Fellows to use. Wales (20%) at the time of application.
Zealand workforce, with 20–30% of The hospitals that possess the highest
We will also be rolling out peer review
medical positions in both countries being number of IMGs in Specified Training are
workshops in 2011 similar to our
held by people who have completed Children’s Hospital, Westmead; Sydney
supervision workshops but specifically
some part of their training abroad. Children’s; John Hunter; Royal Children’s,
for Fellows involved in peer reviewing
Ensuring that IMGs and their supervisors Victoria; and Royal Brisbane & Women’s.
OTPs. These workshops will seek to assist
are supported and that IMG assessment
Fellows in understanding our policies The RACP OTP and Workforce Expert
processes are fair, robust and transparent
and procedures in this area as well as Advisory Groups are the policy-making
is a priority for the College.
addressing specific issues that may come bodies in this area and always welcome
It is incredibly daunting for anyone to up for IMGs and their supervisors during feedback on how policy and processes
move to another country, but add the review. can be improved and how we can further
fact that your partner and young children support OTPs and their preparation for
The RACP is also in frequent contact
may be moving with you, that English workforce change.
with the Australian Medical Council, the
may not be your native tongue and that Medical Board of Australia and other key For more information please don’t
registration in Australia and New Zealand stakeholders seeking ways to improve the hesitate to contact us:
is a very complicated process, with many assessment process for IMGs and OTPs
stakeholders involved, and it is easy to while still ensuring patient safety, which OTP Unit
see how stress levels would be extremely is of course our primary responsibility. Education Deanery
high. Royal Australasian College of Physicians
In 2009, the RACP Australian Division 145 Macquarie Street
For supervisors and peer reviewers also, OTP Sub-committees assessed 175 new Sydney NSW 2000
supporting IMGs can create some very applications for Specialist and Area of AUSTRALIA
specific challenges. It is never easy to Need assessment, and progress was
coach team members on cultural and considered for an additional 71 OTPs. Adult Medicine: +61 2 8247 6206
communication issues, especially when The Faculties and Chapters of the RACP Paediatrics & Child Health: +61 2 8247
these are things that we have learned assessed 14 OTPs in the same period. 6205
just by growing up in a particular The RACP also supported 142 Specified Email: otp@racp.edu.au
environment. Training applications for IMGs (previously
known as OTVs), and 25% of Basic The Royal Australasian College
Moving forward, there are several ways in of Physicians
which the RACP is seeking to support and Trainees completed their medical degrees
overseas. 5th Floor, 99 The Terrace
inform IMGs and their supervisors. With (PO Box 10601)
assistance from the Department of Health The five most common countries for Wellington 6036
and Ageing, the RACP has developed an Specified Training applicants were India NEW ZEALAND
OTP Orientation Module. The module is (31%), the United Kingdom (12%),
designed to familiarise applicants with Malaysia (9%), Germany (8%) and the Phone: +64 4 472 6713
the Australian healthcare environment, Philippines (6%). The five most common Email: racp@racp.org.nz
preparing them for practice in Australia. countries of origin for OTPs applying Keith Johnstone
It focuses on professional qualities such for assessment in Australia were India, Senior Executive Officer, Advanced
as ethics and communication, as well as the UK, South Africa, Germany and the
Training and OTP Units
giving an overview of Australian cultural Philippines. Switzerland and Sri Lanka
issues. The module is now a requirement also featured prominently. Estimates from Member of the Expert Advisory Group on
for all Overseas Trained Physicians (OTPs) the Australian Medical Council state that Overseas Trained Physicians
RACP News August 2010 11Workforce
EHEALTH NEWS!
HEALTHCARE IDENTIFIERS
D
id you know that the For example, the pathology organisation eHealth Survey
Healthcare Identifiers Bill was doing blood tests for your patients will
recently passed in the Senate? not be able to see what is stored on your Complete the five-minute Physicians & IT
It happened the day after the computer or on hospital computers. in the Workplace Survey and win a prize!
changeover of PM so it didn’t get a lot of Keep your eye out for an email with a
media coverage. Here is what you need
to know.
What is a shared link to the online survey that will be sent
to a sample of physicians and trainees.
The healthcare identifier is a 16 digit
electronic health There is an increasing demand for clinical
information to be exchanged between
electronic health number that every record? specialists and other healthcare providers
Australian will get (no opt out) with a
gradual rollout from 1 July 2010. This This is now referred to as a Personally and health departments. The recent
number will store each individual’s name, Controlled Electronic Health Record eHealth reform changes have largely been
address and date of birth. No clinical (PCEHR) to emphasise the fact that there made without specialist involvement.
information will be stored with this is in fact more enhanced privacy and Information gathered from this survey
number. control of access with the electronic will enable the College to act on behalf
system than the current old-fashioned of the Fellowship so that specialists have
All healthcare providers, including a stronger voice in the development of
paper record system.
hospitals, specialists, general practitioners future information technologies.
and pathology departments, will use Although everyone will get a Healthcare
this unique number for each patient, Identifier number, not everyone is Please contact Alexandra.Lipman@racp.
which will make communication between compelled to have a personal electronic edu.au for more information regarding
providers easier. the survey.
health record. Those interested (hopefully
However, the information stored on each most Australians) can opt Dr Steven Bollipo FRACP
provider’s desktop will stay there and will in to this system by registering online Chair of the RACP eHealth Expert
not be seen by other providers. from 2012. Advisory Group
SEND IN
GET RACP NEWS YOUR POETRY
DELIVERED STRAIGHT If you have aspirations to
TO YOUR IN BOX be the next Wordsworth,
Whitman, Wright or Wilde,
send in the poems you
GO GREEN, have buried in that bottom
GO PAPERLESS drawer to racpnews@racp.
edu.au. We will consider
all entries for publication.
DO YOUR BIT FOR Something like this, maybe?
THE ENVIRONMENT Love set you going like a
fat gold watch.
To receive an electronic copy The midwife slapped your
footsoles, and your bald cry
of RACP News email Took its place among the
racpnews@racp.edu.au elements.
with Electronic Copy Only Sylvia Plath, from Morning Song,
in the subject field. Colossus
12 RACP News August 2010TAKE UP THE CHALLENGE:
Indigenous Health
and Chronic Disease
Join us for the RACP Congress 2011 in spectacular Darwin from 22 – 25 May 2011.
Held at the Darwin Convention Centre, the Congress will examine the challenges
of indigenous health and chronic disease over a 4-day program.
RACP Congress 2011 will incorporate:
RACP Graduation Ceremony and Reception | AFOEM Annual Training Meeting
(ATM, 21 – 22 May 2011) | RACP Trainees’ Day | Joint Adult Medicine Division /
Internal Medicine Society of Australia and New Zealand Annual Meeting | Paediatrics
& Child Health Annual Meeting | Australasian Faculty of Occupational & Environmental
Medicine Annual Meeting | Australasian Faculty of Public Health Medicine
Annual Meeting
Take the opportunity to participate in what promises to be an exciting Congress
and take some time to discover the natural beauty of the Northern Territory.
For more information and to register your interest
in the Congress visit www.racpcongress2011.com.au
Or contact the Congress Secretariat at WaldronSmith Management
61 Danks Street Port Melbourne VIC 3207 T : 61 + 3 9645 6311
F : 61 + 3 9645 6322 E : racpcongress@wsm.com.au
RACP News August 2010 13Education
PHYSICIAN READINESS FOR
EXPERT PRACTICE (PREP):
ADVANCED TRAINING
FROM THE DEAN Table 1 lists the 38 curricula that have been completed or are in development. Many of
these curricula combine the objectives for adult and paediatric training pathways within
a single document. Completed curricula are available on the College website. Figures 1
and 2 represent the status of curriculum development for each subspecialty.
Table 1: Curricula completed and in development
Completed (13)
Cardiology (Adult) Palliative Medicine
Cardiology (Paediatrics) Respiratory Medicine (Adult)
Dermatology (NZ) Respiratory Medicine (Paediatrics)
Haematology Rheumatology (Adult)
Medical Oncology (Adult) Sleep Medicine (Adult)
Neonatal/Perinatal Medicine Sleep Medicine (Paediatrics)
Occupational and Environmental Medicine
In Development (25)
Addiction Medicine Intensive Care Medicine
Adolescent Medicine Medical Oncology (Paediatrics)
Clinical Genetics Nephrology
Clinical Pharmacology Neurology (Adult)
Community Child Health Neurology (Paediatrics)
Professor Kevin Forsyth
Endocrinology (Adult) Nuclear Medicine
T
he College is developing Endocrinology (Paediatrics) Paediatric Emergency Medicine
Advanced Training programs Gastroenterology Public Health Medicine
using a framework that outlines General Medicine Rehabilitation Medicine (Adult)
the broad set of standards and General Paediatrics Rehabilitation Medicine (Paediatrics)
elements of training that will apply to all
Geriatric Medicine Rheumatology (Paediatrics)
PREP: Advanced Training programs. The
combination of these elements makes up Immunology/Allergy Sexual Health Medicine
the basic structure for the development of Infectious Diseases
Divisions Curricula
all subspecialty PREP: Advanced Training
Figure 1: Divisions curricula
programs across the Divisions, Faculties
and Chapters of the College. Adult Paeds
7
The PREP: Advanced Training Framework
includes: 6
5
• curricula
4
Stage
• formative assessments 3
• teaching and learning 2
1
• programmatic requirements
0
• online environment d y y cs logy alth (NZ) logy logy d s d y y es ne gy Med logy logy Med Med cine logy Med
Me iolog iatr neti Me ed Me olog llerg as dici olo i
nt h o He y ino ro al Pa ic t se l
ta phr
o
ur
o r cy ed ato eep
ce rd yc Ge mac ild olog cr ente ner eral iatr ema y /
A
Di e M
e c
On rina ea
Ne ucl rgen ve M eum
Ca t Ps cal Sl
• supervision Ad
ole
s
e n lini
l P h a r
i t y C h
r m
a t
E n d o
s tro G e
G e n
G e n
H a
o lo g
t i
s r
ou Ca Me l/Pe
d Ne N
m
e
l l i a ti R h
sc C
ica un De Ga un ec ve at
a E
Pa
ole lin omm I m
m Inf ensi on ae
d
A d C t e P
In
• site accreditation ild
& C N
Ch
• certification of training. Figure 2: Chapter and Faculty curriculaChapter and Faculty Curricula
Adult Paeds
Curricula 7
We are developing subspecialty Advanced 6
Training Curricula to outline the broad 5
concepts, related learning objectives, and
the associated knowledge, skills, attitudes
Stage
4
and behaviours required and commonly 3
utilised by graduates of each training
program. 2
All Advanced Training Curricula are to be 1
used in conjunction with the Professional 0
Qualities Curriculum (PQC), which spans Addiction Medicine Palliative Medicine Sexual Health
Medicine
Occupational &
Environmental
Public Health
Medicine
Rehabilitation
Medicine
the life of the PREP program. Medicine
14 RACP News August 2010Legend for Figures 1 and 2 A Case-based Discussion encounter takes Input from this user group is invaluable in
approximately 30 minutes. guiding the College’s resource development
Stages of Curriculum Development Legend and informing the implementation plans
Cases for discussion
Initial stages 1 of the Advanced Training Education
Reasonably progressed 2
Cases for discussion are chosen by the Committees, and we offer our gratitude
assessor. A variety of cases in which the to all those who volunteered their
Review panel 3 trainee has had a significant role in the involvement.
Submitted to Education Deanery for review 4 clinical decision making and patient
management can be used. The discussion A video showcasing a Case-based
Final stages 5 can focus on a single complex case or a Discussion encounter will be available on
Awaiting ratification 6 series of cases that cover a wide range the College website in the coming weeks.
Ratified 7
of clinical problem areas. The discussion
should reflect the trainee’s level of
experience and be linked to the relevant Development and
Formative Assessments Advanced Training curriculum. implementation of
The trainee is responsible for ensuring that
The PREP: Advanced Training Framework
adequate encounters are completed and
PREP: AT programs
includes a range of formative workplace- that all assessable areas outlined in their Advanced Training Education Committees
based assessments to be introduced as respective Advanced Training curriculum
part of PREP: Advanced Training. The are working in partnership with the
are covered. Education Deanery to develop subspecialty
assessment methods in this framework
are in accordance with international best Areas for assessment Advanced Training programs within the
practice. The respective Advanced Training PREP: Advanced Training Framework. This
• Record keeping
Education Committees are considering how involves matching appropriate formative
the PREP: Advanced Training assessments • History taking assessments to the curricula and planning
will be integrated into their curricula. the introduction of resources to support
• Clinical findings and interpretation
teaching and learning in the program.
Case-based Discussion • Management plan
Part of this process will also involve a
Case-based Discussion is one assessment • Follow-up and future planning systematic review of current programmatic
method that will be widely introduced as Trainee responsibilities requirements and processes to ensure
part of PREP: Advanced Training. It has that they are relevant in the context of
already been incorporated into a number • Arrange a Case-based Discussion PREP training. A review of programmatic
of international postgraduate medical encounter with an assessor. requirements is an important step to enable
education courses. • Confirm the case(s) chosen by the the College to prepare for the influx of
assessor. trainees in the future, and to ensure that
Purpose
consistency and alignment between College
• Provide the assessor with a copy of the
A Case-based Discussion encounter aims to training programs are achieved.
standardised RACP Case-based
evaluate the level of professional judgement
Discussion form. Transparent requirements for training will
exercised in clinical cases by the trainee.
Case-based Discussion is designed to: • Complete tasks after the encounter, be documented in specialty-specific training
including entering data into the online program handbooks. These documents
• guide the trainee’s learning through Case-based Discussion tool and will be developed through consultation
structured feedback emailing the completed form to the with Education Committees and Specialty
• help improve clinical decision assessor. Society representatives and will provide
making, clinical knowledge and patient Assessor responsibilities clear information to trainees, supervisors,
management committee members, College staff and the
• Choose the case(s) for discussion. general public.
• provide the trainee with an opportunity
to discuss their approach to the case • Use the RACP Case-based Discussion It is anticipated that implementation of all
and identify strategies to improve their form to rate the trainee. of the elements within each subspecialty
practice • Provide constructive feedback and PREP: Advanced Training program will be
discuss improvement strategies. a gradual process over a number of years.
• be a teaching opportunity, enabling
the assessor to share their professional Advanced Training Education Committees
• Provide an overall judgement on the
knowledge and experience. trainee’s clinical decision-making skills. will plan the implementation of programs
and set transitional arrangements that will
Overview A number of Advanced Training supervisors be practical and achievable for trainees and
recently volunteered to take part in a trial of supervisors in the context of the workplace.
A Case-based Discussion encounter involves Case-based Discussion with trainees in their
a comprehensive review of clinical cases workplace. The feedback collected from Kevin Forsyth FRACP
between an Advanced Trainee and an the participants of this trial regarding their Dean
assessor. The trainee is given feedback from experiences using this assessment method
an assessor across a range of areas relating will be evaluated and reported on. (See the Susi McCarthy
to clinical knowledge, clinical decision first report from Associate Professor Benny Curriculum Development Officer
making and patient management. Katz on page 17). Education Deanery
RACP News August 2010 15You can also read